Attitude and Knowledge of Orthodontics among General Dentists and Non-Orthodontic Specialists: A Questionnaire Based Survey
Mohamed AboshamaMuhanad L. Alshami1, Nada K. Imran2*, Mustafa R Abdurazaq1, Krunal Narendrakumar3
1 Department of Dentistry, Dijlah University College, Baghdad, Iraq.
2 College of Dentistry, University of Baghdad, Baghdad, Iraq.
3 College of Dentistry, University of Birmingham, Birmingham.
*Corresponding Author
Nada K Imran,
College of Dentistry, University of Baghdad, Bab Al-Muada’am, Medical City of Baghdad, Iraq.
Tel: 07806808016
E-mail: ali.periodontics@gmail.com
Received: August 15, 2020; Accepted: September 07, 2020; Published: September 16, 2020
Citation:Muhanad L. Alshami Nada K. Imran, Mustafa R Abdurazaq, Krunal Narendra Kumar. Attitude and Knowledge of Orthodontics among General Dentists and Non-Orthodontic Specialists: A Questionnaire Based Survey. Int J Dentistry Oral Sci. 2020;7(9):814-819. doi: dx.doi.org/10.19070/2377-8075-20000160
Copyright: Nada K Imran©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim: This study aimed to assessing orthodontic knowledge and attitude among general dentists and non-orthodontic specialists.
Background: Early detection of orthodontic disorders is essentialin motivating patients to intervene prior to long term complications
when the disorders are not recongised.
Methods: A questionnaire was distributed amongst dentistsother than orthodontists. This questionnaire consisted of three
sections. The first one aimed to collect demographic, educational level and practice type information. Further two sections
consisted of closed-end questions designed to evaluateknowledge and attitude of orthodontics.
Results: A total of 313 responses to the survey were submitted. No significant correlation was observed, except for the specialty
and qualification towards orthodontics knowledge. In terms of gender demographics, females had significantly higher
attitude toward orthodontics compared to males.
Conclusion: The results emphasise the vital role of continuing education programs and updating the curricula of dental colleges
in the promotion of knowledge and attitude toward orthodontics among dentists.
Clinical Significance: Knowledge and attitude of general practitioners and non-orthodontic specialists toward orthodontic
issues is crucial in diagnosis and referral to receive proper treatment at early stages.
2.Introduction
3.Material and Method
4.Results
5.Discussion
6.Conclusions
7.References
Keywords
Orthodontics; Knowledge; Attitude; Dentists.
Introduction
Malocclusionis the abnormality of eruption process of permanent
or deciduous teeth in jaws, considered to being one of the
most important factors, next to dental caries that causes significant
oral pathology. Examples include tooth decay, defects in the
temporo mandibular joint and gingival diseases. Beside the psychological
effect of people who suffer from defects in the appearance
of the teeth that may negatively impact his/her social
life [1-4]. Orthodontics is the treatment option that corrects these
issues which arise from alteration in morphogenesis and physiology
of dentofacial apparatus over time [5]. The awareness and
benefits of orthodontic treatments among patients is significant
in changing attitudes and enhancing the outcomes of orthodontic
therapies [6]. The task of educating the patient lies largely upon
the dentists who do not have a specialist knowledge in orthodontics.
Their role is important in identifying the patient who needs
to undergo a correction in dental occlusion or other orthodonticrelated
treatments [7]. Assessing the knowledge of dentistsin orthodontics
is necessary to ensure that they are able to diagnoseany
problemsin patients and they are subsequently referred to orthodontic
specialists for treatment [8].
The aim of this study was to evaluate the knowledge and attitude
towards orthodontics among dentists and non-orthodontic specialists.
This study wasa cross-sectional investigation among general practitioners
and non-orthodontic specialists working in different institutions
and dental clinics. The ethical approval was obtainedfollowing
Helsinki declaration prior to conducting the survey. The
study was carried out from March 2020 to May 2020 during which
the questionnaire was distributed via e-mail. Informed consent
was obtained from each participant before responding to the
questions.
The questionnaire template was based on previous study [9]. Sections
of the questionnaire used for this study are illustrated in
Table 1. The first part of the questionnaire was designed in collecting
the demographic and other practice-related information such as area of work and number of patients treated/day. The
second part of the questionnaire (from question No. 1 to No. 13)
aimed to assess the knowledge about orthodontic treatment approaches,
its effect on facial appearance, diagnosis, components
of orthodontic appliances, habits, and the suitable age of orthodontic
treatment. The last part (from question No. 14 to No. 20)
was designed to evaluate the attitude of the participants about
these principles and practice.
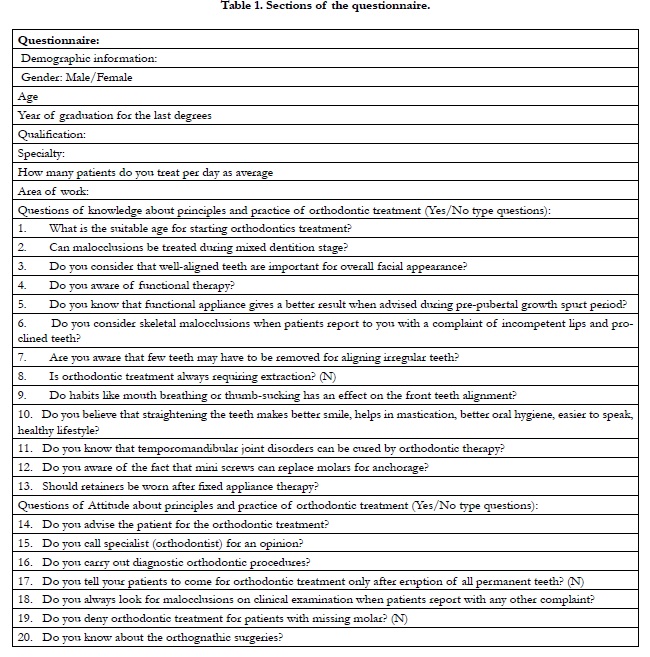

Table 1. Sections of the questionnaire.
The questions were of Yes/No type and each correct answer was given a score 1 and score 0 was given for any incorrect answer. Frequency of correct/incorrect responses were used to assess knowledge and attitude to orthodontics and their association with different variables included in this study.
Descriptive statistics was used to express the mean scores and
standard deviation. Scores were calculated based on the responses given by participants and the individual scores were summed up
to calculate the number of correct/incorrect answers. Inferential
analysis was performed by using Linear regression and Pearson’s
correlation coefficient (r), strength of association for attitude and
knowledge with different variables was calculated by Chi-square
test.Significant level was set at p<0.05. Statistical analysis was
done using SPSS software (Version 21, IBM, USA).
Results
Responses from 313 dentists were analysed. Descriptions of all
variables included in this study were summarized in Table 2. According
to the knowledge section, the positive responses were the
highest for the ninth question, which included the effect of bad
habits on aligning the teeth.The lowest number of positive responses
was knowing the appropriate age to start the orthodontic
treatment (first question). Within the attitude section, most
of the participants were advising patients to choose orthodontic
treatment (question 14) with less than half of the dentists (133)
indicating that they had not performed any checks on orthodontic
problems (question 16) (Figure 1). Regression analysis was used
to test the relation of these variables with the level of knowledge
and attitude of the dentists towards orthodontic treatment.
Among all independent variables entered only qualification and
specialty remained as significant predictors of the knowledge and
the gender as predictor of the attitude Table 3. Both qualification
and specialty showed significant and positive correlation with the
level of knowledge about orthodontic treatment Table 4. Gender
was shown to have a positively significant correlation with the
attitude towards orthodontics Table 5. Further analysis for association
for these predictors showed that dentists with higher degreeshave
higher knowledge compared to bachelor degrees (OR 1.206) holders, with same applied to the specialists as compared
to the general practitioners (1.192) Table 6. The attitude towards
orthodontic treatment was significantly associated with the female
than male counterparts (OR 1.311) Table 6.
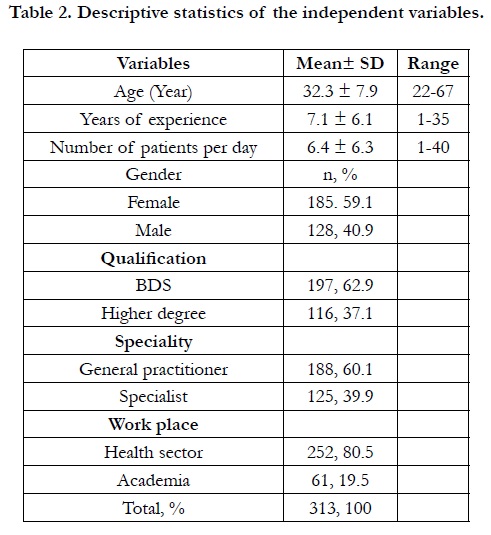
Table 2. Descriptive statistics of the independent variables.
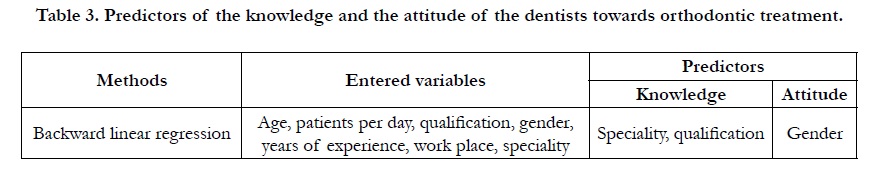
Table 3. Predictors of the knowledge and the attitude of the dentists towards orthodontic treatment.
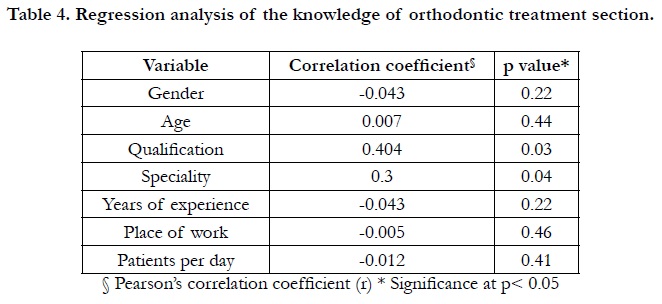
Table 4. Regression analysis of the knowledge of orthodontic treatment section.
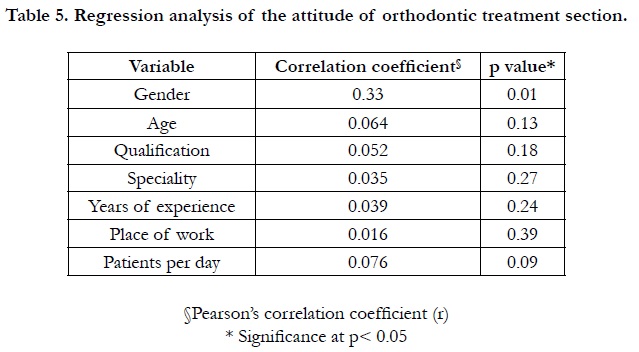
Table 5. Regression analysis of the attitude of orthodontic treatment section.
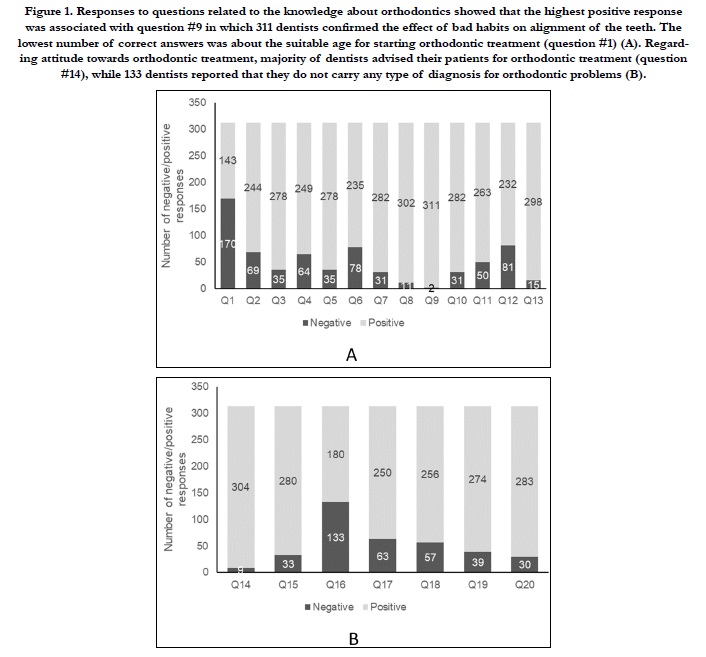

Figure 1. Responses to questions related to the knowledge about orthodontics showed that the highest positive response was associated with question #9 in which 311 dentists confirmed the effect of bad habits on alignment of the teeth. The lowest number of correct answers was about the suitable age for starting orthodontic treatment (question #1) (A). Regarding attitude towards orthodontic treatment, majority of dentists advised their patients for orthodontic treatment (question #14), while 133 dentists reported that they do not carry any type of diagnosis for orthodontic problems (B).
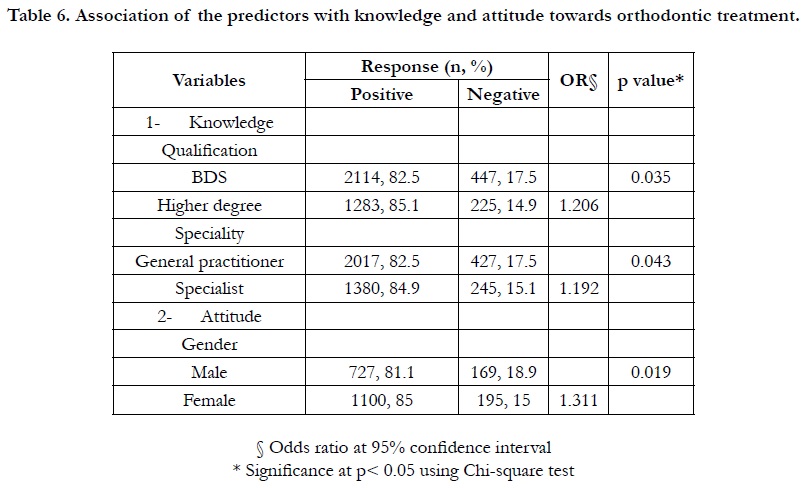
Table 6. Association of the predictors with knowledge and attitude towards orthodontic treatment.
Discussion
The results of this study showed that specialty and qualification
were significantly correlated with knowledge and the females has
higher attitude towards orthodontics. Malocclusion is the most
prevalent dental pathology after dental caries that interfere with
facial profile and dental appearance [10]. Improvement of dental
occlusion by orthodontic treatment could be helpful in enhancing
the general face appearance and restoring normal function as
much as possible [11, 13]. Therefore, the orthodontic treatment
has a key-role in esthetic and psychological aspects.
The degree of understanding of orthodontic treatment and its
benefits among the general public largely depends on the degree to
which dentists generally know the reasons for orthodontic treatment
and the ability to diagnose and refer a patient who needs to
consult an orthodontist [14]. Habits such as finger sucking, finger
biting and lip sucking have the worst effect on the growth of jaws,
teeth position and surrounding tissue which should be obvious to
the dentist during examination [15, 16]. Knowledge of the effect
thatbad habits have on the alignment of the teeth was high among
the participants.
The appropriate age for treating an orthodontic problem depends
on the severity of the condition, its causes and the expertise of
the orthodontist [17]. Several studies mentioned that Early treatment
contributes to reducing complications with increasing age
and reducing the extent/duration of treatment [18, 19]. The suitable
age for treating orthodontic-related problem was not known
to half of the participants in the study, this may affect the advice
and referral of the patient who suffers from problems in orthodontics
and make the treatment take longer [20]. The improvement
of skill and knowledge of dentists to diagnose the problems
associated with orthodontic is essential in ensuring the correct
referral of a patient to an orthodontist [21], the current study
indicated a defect in this aspect among the dentists.
Qualification and specialty showed significant and positive correlation
with the level of knowledge about orthodontic treatment.
This may be due to the increase in the number of years of experience
and the number of patients who were treated before obtaining
the qualification or familiarity of other specialists with aspect
of orthodontic treatment directly or indirectly interfere with their
specialties. These results came in line with other previous studies
that showed a significant difference in knowledge toward the orthodontics
treatment when comparing general practitioners with
those who have specialty other than orthodontic [7-9]. Although
some studies find no significant difference when conducting the
same comparison [22].
According to gender, the present study showed that females expressed
higher attitude than males towards the treatment of malocclusion,
similar findings were mentioned in previous studies
[23]. The explanation could be that females are more knowledgeable
and are more concerned about the appearance, hencefemales
can easily identify defects in the aesthetics of the teeth compared tomales, which probably motivate them to gain more knowledge
about orthodontics.This finding at the same time differs from
other studies which state that males were higher than females in
knowledge and attitudeabout the principles of malocclusion correction
[7].
The major limitation of this study is that the degree of attitude
and knowledge evaluation of non-orthodontic specialists was
based mainly on their theoretical background only and not on
clinical experience which alter their judgment on orthodontic
treatment. In addition, answers to questions may not represent
the actual clinical practice of the respondents. Therefore, generalizability
of the current findings to all dental community must be
dealt with caution.
Conclusions
The current study showed that most of the respondents have
information about orthodontics, but with varying degrees. The
qualification of the dentists had the most significant impacton the
awareness and referral the patient to a specialist. Dentists should
pay attention to participation in continuous medical education
that synchronize with updates in the field of orthodontics.
References
- Siddegowda R, Rani M. An epidemiological survey on awareness towards orthodontic treatment in South Indian school children. Open J Dent Oral Med. 2013; 1: 5-8.
- Essamet M, Darout. Knowledge and attitude toward orthodontic treatment among treated subjects compared with untreated subjects and correlation with atient–orthodontist communication. World J Dent. 2017; 8: 218-23.
- Moshkelgosha V, Kazemi M, Pakshir H, Safari R. Parental knowledge and attitude towards early orthodontic treatment for their primary school children. Iran J Orthod. 2017; 12.
- Klages U, Bruckner A, Zentner A. Dental aesthetics, self-awareness, and oral health-related quality of life in young adults. Eur J Orthod. 2004; 26: 507- 14. PMID: 15536839.
- Rastogi S, Jatti R, Keluskar K. Assessment of Awareness and Social Perceptions of Orthodontic Treatment Needs in Adult Age Group: A Questionnaire Study. Journal of Oral Health & Community Dentistry. 2014; 8.
- Soni U, Baheti M, Dash S, Toshniwal N, Baldawa R. Knowledge and awareness of malocclusion among rural population in India. Asian Pac J Health Sci. 2014; 1: 329-34.
- Sastri MR, Tanpure VR, Palagi FB, Shinde SK, Ladhe K, Polepalle T. Study of the knowledge and attitude about principles and practices of orthodontic treatment among general dental practitioners and non-orthodontic specialties. Journal of international oral health: JIOH. 2015; 7: 44-8. PMID: 25878478.
- Kapoor D, Bhatia S, Garg D. Assessment of the Attitude and Knowledge of the Principles and Practices of Orthodontic Treatment Among the Nonorthodontic Specialists and General Practitioner Dentists. J NEPAL MED ASSOC . 2018; 56: 766-769. PMID: 30387466.
- Alnusayri MO, KuraymAlenazi KK, Patil SR, Aileni KR, Rao KA. Knowledge and attitude regarding principles and practices of orthodontic treatment among general dental practitioners and non-orthodontic specialists of Saudi Arabia: A preliminary study. J Res Med Dent Sci. 2017; 5: 59-62.
- Parmesh H, Mathur V. National Oral Health Care Program. Indian Pediatr. 2002; 39: 1001.
- Al Fawzan A. Reasons for seeking orthodontic treatment in Qassim region: a Pilot Study. Int Dent J Stud Res. 2013; 1: 58-62.
- Pandey M, Singh J, Mangal G, Yadav P. Evaluation of awareness regarding orthodontic procedures among a group of preadolescents in a cross-sectional study. J Int Soc Prev Community Dent. 2014; 4: 44-7. PMID: 24818094.
- Baswaraaj JB, Kumarswamy K, Padmini M, Chandralekha B. Oral self perception of esthetics among dental students. Arch Oral Sci Res. 2013; 3: 85- 94.
- Siddegowda R, Rani M. An epidemiological survey on awareness of orthodontic treatment in school children from four divisions of Karnataka State, India. World J Med Med Sci, 2014; 2: 1-6.
- Joelijanto R. Oral habits that cause malocclusion problems. IDJ. 2012; 1.
- Kamdar RJ, Al-Shahrani I. Damaging oral habits. Journal of international oral health: JIOH. 2015; 7: 85-87. PMID: 25954079.
- Pietilä I, Pietilä T, Pirttiniemi P, Varrela J, Alanen P. Orthodontists' views on indications for and timing of orthodontic treatment in Finnish public oral health care. Eur J Orthod. 2008; 30: 46-51.
- Fleming P. Timing orthodontic treatment: early or late?. Aust Dent J. 2017; 62: 11-19. PMID: 28297091.
- Grippaudo C, Pantanali F, Paolantonio EG, Saulle R, Latorre G, Deli R. Orthodontic treatment timing in growing patients. Eur J Paediatr Dent. 2013; 14: 231-6. PMID: 24295010.
- Abdelkarim A, Jerrold L. Strategies for improved interdisciplinary care and communication in orthodontics. Am J Orthod Dentofacial Orthop. 2017; 152: 717-21. PMID: 29103450.
- Chew MT, Aw AKL . Appropriateness of orthodontic referrals: self‐perceived and normative treatment needs of patients referred for orthodontic consultation. Community Dent Oral Epidemiol. 2002; 30: 449-54. PMID: 12453116.
- Acharya A, Mishra P, Shrestha RM, Shah P. Orthodontic treatment knowledge among general dentists and non-orthodontic specialists. Orthod J Nepal. 2019; 9: 40-4.
- Polychronopoulou A, Kawamura M. Oral self‐care behaviours: comparing Greek and Japanese dental students. Eur J Dent Educ. 2005; 9: 164-70. PMID: 16194248.





