Evaluation of the Effectiveness of Sodium Hypochlorite Gel Application in Removing Dental Plaque Before Pit and Fissure Sealant Placement: A Randomized Controlled Clinical Trial
Lilian Azrak1, Nada Bshara2, Muaaz Alkhouli3*
1 PhD, MSc, DDS, Department of Pediatric Dentistry, Faculty of Dentistry, Damascus University, Syria.
2 Professor at Department of Pediatric Dentistry, Faculty of Dentistry, Damascus University, Syria.
3 MSc, DDS, Department of Pediatric Dentistry, Faculty of Dentistry, Damascus University, Syria.
*Corresponding Author
Muaaz Alkhouli MSc, DDS,
Department of Pediatric Dentistry, Faculty of Dentistry, Damascus University, Syria.
Tel: 00963966133383
E-mail: muaaz.alkhouli@outlook.com
Received: May 07, 2020; Accepted: July 08, 2020; Published: July 15, 2020
Citation:Lilian Azrak, Nada Bshara, Muaaz Alkhouli. Evaluation of the Effectiveness of Sodium Hypochlorite Gel Application in Removing Dental Plaque Before Pit and Fissure Sealant Placement: A Randomized Controlled Clinical Trial. Int J Dentistry Oral Sci. 2020;7(7):776-780. doi: dx.doi.org/10.19070/2377-8075-20000152
Copyright: Muaaz Alkhouli©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objectives: To evaluate the cleaning efficacy of 2.2% sodium hypochlorite gel compared to pumice powder on the permanent
first molars before applying the sealant.
Materials and Methods: Sixty sound molars were recruited from30 patients (7-10 years) in which their plaque on the occlusal
surfaces of permanent first molars was stained (Mira-2-Tone) and photographed. Molars were selected randomly and divided
into 3 groups: G1 pumice powder (n=30 molars) G2: sodium hypochlorite gel applied for 30 seconds (n=30 molars), G3:
sodium hypochlorite gel reapplied for another 30 seconds (n=30 molars).Then the Mira- 2tone was applied and photographed
before and after the cleaning. In a conventional picture editing program.The occlusal surface and plaque were measured in pixels
and the relative proportion of occlusal plaque was calculated. Samples from eachgroup were etched with 37% phosphoric
acid gel for 15 seconds followed by placement of a sealant.
Results: There was astatistically significant difference between after and before cleaning in the three analyzed groups (T test:
p<0.05). The percentage of variation in coloring rate was 68%for the G3 group, while the percentage of variation in coloring
rate G2 and G1 group was 44%, 39% respectively.
Conclusion: The use of 2.2% Na0Cl gel for 60 seconds had a better cleaning efficacy comparing pumice powder and was
able to remove dental plaque before applying the sealant.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusions
7.References
Keywords
Sodium Hypochlorite Gel; Pits and Fissures; Variation in Coloring Rate.
Introduction
As dental caries becomes a public health problem over the last
few decades, a big advance has been made in caries prevention.
suppression of dental plaque formation, mechanical removal of
dental plaque, fluoride treatment either topically or systemically,
pit and fissure sealants application and dental health educationalprograms
have had an undeniable effect on caries prevention
recently [1].
Pit and fissure sealants are considere done of the effective modes
in the prevention of dental decay in caries-susceptible teeth by
creating a physically protective barrier that keeps the cariogenic
bacteria away from the nutrients needed and prevents the enamel
surface from being demineralized. These preventive characteristicsare
mainly obtained and maintained as long as the sealantsremain
completely intact and bonded in place [1, 2].
On the other hand, sealant placement is a very sensitive technique
because there is a risk of leaving some residual material, moisture,
or air bubbles inside of the fissures preventing proper sealant
penetration and endangering optimal retention and structural
integrity [2, 3]. Moreover, inadequate removal of dental plaque
before etching can harm sealant retention or lead to microleakageincreasing
the probability of caries development [4].
Both invasive and non-invasive methods are used in the purpose of cleaning and preparing the enamel fissures prior to etching and
sealant application. However, those methods have delivered contrasting
and even contradictory results [5, 6]. Dry brushing, pumice
prophylaxis with rubber cups, fissure burs, adhesive agents,
lasers, abrasion with air, sodium bicarbonate, or aluminum oxide
particles and prolonging the etching time are some examples of
techniques currently suggested in pediatric dentistry to reduce the
plaque content within pits and fissures [7, 8].
Despite the hypothesis that mentioned that pumice powder has
some residues in the pits and fissures after 60 seconds from washing
or 30 seconds from etching [9], Pumice prophylaxis is still
used as a routine basis before sealant application [10, 11]. In return,
sodium hypochloritegel has not been studied as a plaque
removal agent within pits and fissures before sealant application
to the best of our knowledge although it has been used widely in
dental procedures due to its antibacterial and deproteinizingeffect.
Therefore, this trial was aimed to evaluate the use of different
methods to clean occlusal pits and fissures: pumice prophylaxis,
30 seconds application of NaOCl gel 2.2% and 60 seconds application
of NaOCl gel 2.2%.
This study was a randomized controlled clinical double-blinded
trial composed of two teeth of each participant (split mouth
study). Thirty cooperative children (15 male and 15 female) aged
between 7-10 years participated in this trial. They were all recruited
from pediatric dentistry department of Damascus University.
In total, 60 molars were enrolled in the study and they werelower
first permanent molars which were caries free based on visual examination
according to ICDAS II detection system (code 0). The
trial was conducted in accordance with the declaration of Helsinki
and approved by the Research Ethics Committee of Faculty
of Dentistry of Damascus University.
The teeth were assigned into three groups; Group 1: teeth were
cleaned with pumice powder (control group) (n=30 molars),
Group 2: teeth were cleaned with sodium hypochlorite gel applied
for 30 seconds (n=30 molars), Group 3: teeth of Group 2
were washed thoroughly and reapplied sodium hypochlorite gel
for another 30 seconds (n=30 molars). Randomization was done using the website www.randomizer.org in order to aid in allocating
teeth into groups randomly.
A signed informed consent was obtained from the parents of all
enrolled children. The plaque was detected using plaque disclosing
agent (Mira-2-tone, Hager & Werken, Germany) before cleaning
of the pits and fissures and after cleaning them in order to evaluate
the effectiveness of the cleaning method used. The following
steps were followed for each tooth: 1-rubber dam isolation. 2 -
Cleaning pit and fissure surfaces either by using pumice powder,
NaOCl gel for 30 seconds or NaOCl gel for 60 seconds 3-Rinsing
and drying 4 - Etching pits and fissures for 30 seconds (Etchant
37%, 3M, USA) 4 - Rinsing and drying again 5- Application of
sealant material (Helioseal,IvoclarVivadent, Liechtenstein). 6- polymerization
using light cure device for 20 seconds. 7 - Occlusion
assessment using articulation paper.
Teeth were photographed from over the occlusal surface in order
to digitaize the images through transferring them to the program
Adobe Photoshop (V6.0, Adobe Systems Ltd, Europe) and
measuring a definite outlined surface in these reformatted images
in pixels. First, an outline of the occlusal surface was done by
connecting lingual and buccal cusp tips through the descending
cutting edges of the cusps and marginal ridges of the occlusal
surfaces (Figure 1). Then, the outline of the disclosed area of the
pits and fissures surface was taken and the ratio between both the
occlusal surface and the disclosed surface was calculated to get the
relative proportion of occlusal plaque, this was named the color
coefficient average of the occlusal plaque, which is calculated using
the following equation:
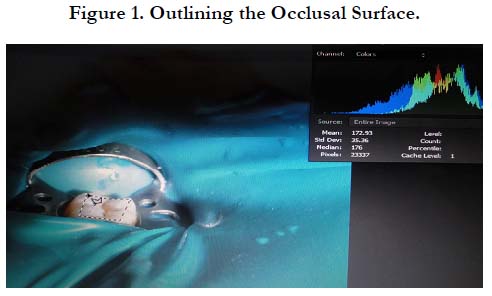
Figure 1. Outlining the Occlusal Surface.
Color coefficient average of the occlusal plaque = (coloration of pits and fissure (pixel))/(occlusal surface (pixel))×100
Two blinded examiners carried out the outlining and this method was done twice for each tooth (before and after cleaning).
The collected data were introduced into SPSS software version 23
(IBM Corp., Armonk, USA). Kolmogorov-Smirnov test was used
to check if the data are normally distributed, and it concludes that
they were normally distributed. The level of significance (P-value)
was set at 0.05 and the power of study was 90%. T-student test
was used to conclude if there is a difference in the level of cleaning
that is statistically significant within each group. Bonferroni Test was also used to show if the dual difference between the
groups was significant.
Results
Data were collected from 30 children (15 male and 15 female),
from whom 60 teeth were randomly assigned into the three
groups. The mean age of children in control group, NaOCl (30
sec) group and NaOCl (60 sec) group was 9.1, 8.6 and 7.9 years,
respectively. Figure 2 shows the CONSORT flow chart concerning
the participants of this trial.
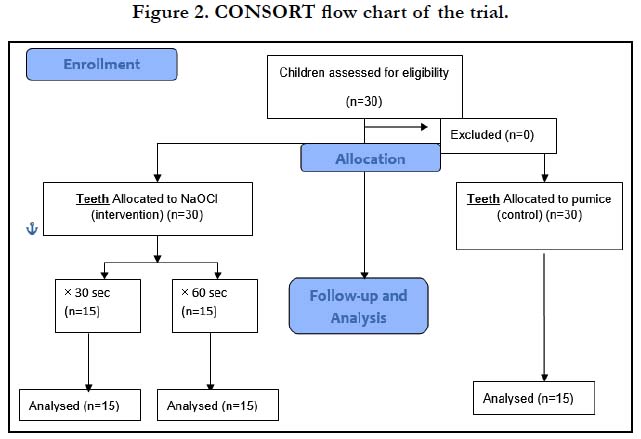

Figure 2. CONSORT flow chart of the trial.
The plaque disclosing agent was used twice for each tooth, before and after cleaning. After each application, the color coefficient average of the occlusal plaque was calculated. Then, the variance between the two values (before and after) was calculated. The variance values were as follows: The use of NaOCl for 60 seconds had the highest variation in coloring rate (-19.59), then the use of NaOCl for 30 seconds, then pumice powder (-13.78, -9.22), respectively.
The study data were distributed normally. For that reason, t-student test was done in order to study the dual differences between the color coefficient averages before and after cleaning of each method (Table 1). T-student test showed that all methods of cleaning were effective in plaque removal as there was a significant difference (P=0.000) when comparing the two stages of intervention (before and after cleaning). In addition, in figure 3, the change in Color coefficient average of the occlusal plaque (Pixels) is demonstrated within each group.
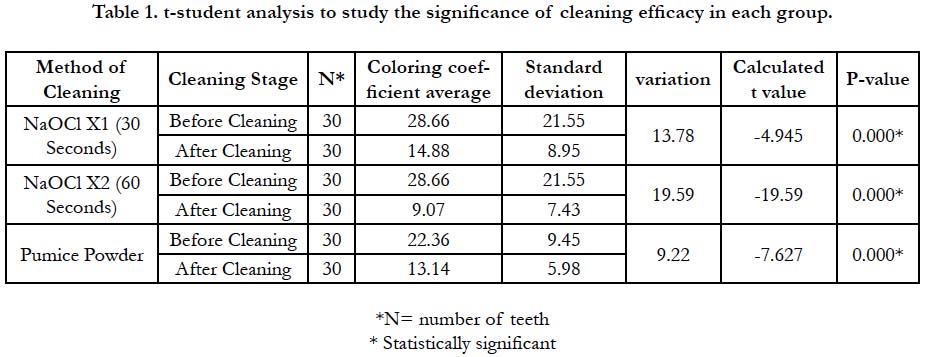

Table 1. t-student analysis to study the significance of cleaning efficacy in each group.
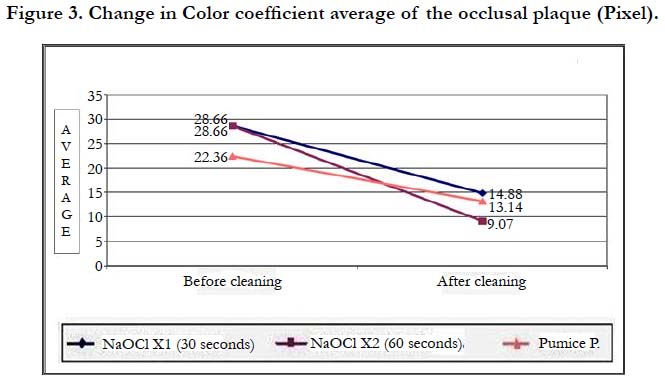
Figure 3. Change in Color coefficient average of the occlusal plaque (Pixel).
Bonferroni test was used to report dual differences between the percentages of variation in coloring rate according to the method of cleaning. There werestatistically differences between the use of NaOCl for 60 seconds and pumice powder (P-value<0.05) in the percentages of variation in coloring rate (Table 2).
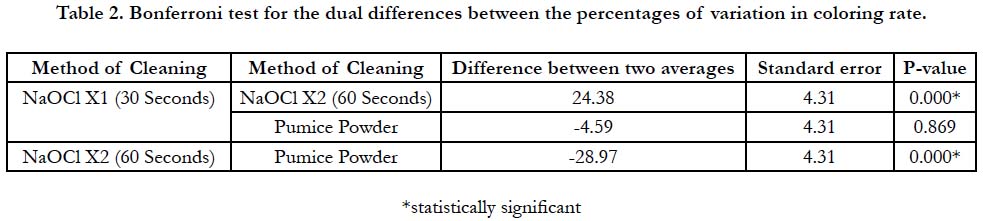
Table 2. Bonferroni test for the dual differences between the percentages of variation in coloring rate.
The success of the cleaning method was measured by the percentage of variation in coloring rate in the occlusal surface, considering this the applying of NaOCl for 60 second was the best cleaning method with percentage of 67.92%.
Discussion
Resin-based pit and fissure sealant is a caries preventive agent that
is applied to caries-susceptible teeth by bonding to the enamel
surface micromechanically, averting access by cariogenic bacteria
to the place of nutrients [5]. Acid etching does not eliminate the
organic content on the enamel surface, which is primarily composed
of protein [12]. The collagen fibril network remained undamaged
after dentin demineralization with phosphoric acid. The
organic content comprises only 1% of the enamel and it cannot
be entirely removed with forgetting the enamel crystals' proteins
[3]. This arise the need of an appropriate preparing method that
can achieves a total removal of the dental plaque and helps etching
to be effective [13].
The present study consisted of 60 erupted permanent molars in
children between 7 years and 10 years of age. Pumice powder,
NaOCl gel for 30 seconds and NaOCl gel for 60 seconds were
the groups to which teeth were randomly allocated for cleaning
of the pit and fissure surface with the use of phosphoric acid for
etching. The study was designed as a split mouth study to standardize
patient associated factors such as the cooperation during
the procedure and the oral hygiene.
Plaque disclosing agent was applied two times for each tooth, before
and after cleaning. In order to assess the effectiveness of
each agent in plaque removal, the occlusal surface was photographed
and digitalized to calculate the surface of plaque in pixels.
Furthermore, the color coefficient average was taken by calculating
the ratio between the occlusal surface and the coloration of
the pit and fissure surface. This aids in overcoming the possible
problems associated with distance difference between the lens of
the camera and the occlusal surface. This method is a valid and
reliable one according to many studies [14, 15].
In this trial, the method of pretreating the enamel surface by deproteinising
with sodium hypochlorite gel (NaOCl) for 60 seconds
prior to etching has proven to be an effective method (68%).
This can be justified for improving the quality of conditioning by significantly removing organic elements and denaturing proteins
present in both the enamel and the acquired pellicle.
The findings of this study is in agreement with Espinoza et al.,
in vitro study, which demonstrated that the deproteinisation process
of NaOCl increases the conditioned area and improves the
quality of enamel acid etching, optimizing the retentive surface
and sealant bond strength. However, their study used the solution
form of the NaOCl [16].
Sodium hypochlorite is introduced commercially in two different
forms, the solution and the gel. The later form (gel) was used to
dentistry to overcome some of the solution related disadvantages.
The gel form was used in this study as it is more controllable in
application than the solution.
NaOCl solution has been used in endodontics for its antimicrobialpropertiesand
ability to dissolve the organic material from
the root canal space without damaging intact dentinal tissues
[17]. Moreover,incleaning the enamel surface, sodium hypochloritereachesthe
organic components and distinct chemical reactionsdevelop
including saponification and neutralization. These
reactions lead to liquefaction of the organicmaterial in enamel
without injuring the enamel structure, a process referred to as
deproteinisation [18]. Because the gel has the same active components
and properties with the solution, this may explain the better
results of using NaOCl gel in this study comparing with pumice
powder thatdoes not have the similar mechanism of action.
According to the in vitro study conducted by Garrocho, the deproteinisation
caused by NaOCl prior to acid etching improved
the bonding to enamel. This was caused by increasing the surface
area of etched enamel after pretreatingthe occlusal enamel
with 60 seconds of NaOCl solution. Therefore, he suggested the
enamel treatment method prior toacid etching to increase the useful
clinical life of resin sealants placed on primary orpermanent
molars [19].
This study revealed that the use of NaOCl for 30 seconds was effective
in relatively equal percentage to the use of pumice powder
(44%) and (39%), respectively. While the application of NaOCl
gel for 60 seconds was more effective with 68% success rate. This
can be due to the time of NaOCl applying according to Gomes et
al, who indicates the increasing results of the cleaning capacity of
NaOCl with the increasing time of applying [20].
Conclusions
Within the limitations of this study, we can conclude that applying
NaOCl gel for 60 seconds is effective in cleaning the pit and
fissure surface to remove the dental plaque prior to sealant placement,
with success rate of 68%.
References
- Simonsen RJ. Pit and fissure sealant: review of the literature. Pediatr Dent. Sep-Oct 2002;24(5):393-414.Pubmed PMID:12412954.
- Simonsen RJ. Retention and effectiveness of dental sealant after 15 years. J Am Dent Assoc. 1991 Oct;122(10):34-42.Pubmed PMID:1835987.
- Ramakrishna Y, Bhoomika A, Harleen N, Munshi AK. Enamel deproteinization after acid etching-is it worth the effort. Dentistry. 2014 Jan 1;4(2):2-6.
- Cooley RL, McCourt JW. Evaluation of by SEM, microleakage, and fluoride release. Pediatric dentistry. 1990 Feb;12(1):39.
- Hegde RJ, Coutinho RC. Comparison of different methods of cleaning and preparing occlusal fissure surface before placement of pit and fissure sealants: An in vivo study. Journal of Indian Society of Pedodontics and Preventive Dentistry. 2016 Apr 1;34(2):111.
- Camacho Castro, L. and A. Claudia Galvão, Comparison of three different preparation methods in the improvement of sealant retention. J Clin Pediatr Dent. 2004 Spring;28(3):249-52.Pubmed PMID:15163154.
- Agrawal A, A Shigli, Comparison of six different methods of cleaning and preparing occlusal fissure surface before placement of pit and fissure sealant: an in vitro study. J Indian Soc Pedod Prev Dent. Jan-Mar 2012;30(1):51-5. Pubmed PMID:22565518.
- Muller‐Bolla M, Lupi‐Pégurier L, Tardieu C, Velly AM, Antomarchi C. Retention of resin‐based pit and fissure sealants: a systematic review. Community dentistry and oral epidemiology. 2006 Oct;34(5):321-36.
- Asquinazi ML, Jasmin JR, Muller M, Magne J. In vitro study of 99m-Technetium labeled pumice: Penetration in fissures. Journal of Dentistry for Children. 1999 Nov 1;66(6):387-9.
- Blackwood JA, Dilley DC, Roberts MW, Swift EJ. Evaluation of pumice, fissure enameloplasty and air abrasion on sealant microleakage. Pediatr Dent. 2002;24(3):199-203.Pubmed PMID:12064490.
- Ansari G, Oloomi K, Eslami B. Microleakage assessment of pit and fissure sealant with and without the use of pumice prophylaxis. Int J Paediatr Dent. 2004 Jul;14(4):272-8.Pubmed PMID:15242384.
- Van Landuyt K, De Munck J, Coutinho E, Peumans M, Lambrechts P, Van Meerbeek B. Bonding to dentin: smear layer and the process of hybridization. InDental Hard Tissues and Bonding. Springer, Berlin, Heidelberg. p. 89-122.
- Gwinnett, A. Histologic changes in human enamel following treatment with acidic adhesive conditioning agents. Arch Oral Biol. 1971 Jul;16(7):731-8. Pubmed PMID:5283531.
- SSmith RN, Brook AH, Elcock C. The quantification of dental plaque using an image analysis system: reliability and validation.JClinPeriodontol. 2001 Dec;28(12):1158-62.Pubmed PMID:11737514.
- Splieth CH, Nourallah AW. An occlusal plaque index. Measurements of repeatability, reproducibility, and sensitivity. Am J Dent. 2006 Jun;19(3):135- 7.Pubmed PMID:16838474.
- Espinosa R, Valencia R, Uribe M, Ceja I, Saadia M. Enamel deproteinization and its effect on acid etching: an in vitro study. J Clin Pediatr Dent. 2008 Fall;33(1):13-9. Pubmed PMID:19093646.
- Mohammadi Z. Sodium hypochlorite in endodontics: an update review. Int Dent J. 2008 Dec;58(6):329-41.Pubmed PMID:19145794.
- Ahuja, B, Yeluri R, Baliga S, Munshi AK., Enamel deproteinization before acid etching–A scanning electron microscopic observation. J Clin Pediatr Dent. Winter 2010;35(2):169-72.Pubmed PMID:21417119.
- Garrocho-Rangel A, Lozano-Vázquez C, Butrón-Tellez-Girón C, Escobar- García D, Ruíz-Rodriguez S, Pozos-Guillén A. In vitro assessment of retention and microleakage in pit and fissure sealants following enamel pre-etching with sodium hypochlorite deproteinisation. Eur J Paediatr Den. 2015 Sep;16(3):212-6.Pubmed PMID:26418924.
- Gomes BP, Ferraz CC, ME V, Berber VB, Teixeira FB, Souza‐Filho FJ. In vitro antimicrobial activity of several concentrations of sodium hypochlorite and chlorhexidine gluconate in the elimination of Enterococcus faecalis. Int Endod . 2001 Sep;34(6):424-8.Pubmed PMID: 11556507.





