Multidisciplinary Approach in Management of Fractured Anterior Teeth: Case Report
Rym Mabrouk1*, Nihel Charfi2, Souha Yahia3, Rim Bibi4, Afef Oueslati5, Nadia Frih6
1 Associate Professor in Endodontics and Restorative Dentistry, Faculty of Dental Medicine of Monastir. Department of Dental Medicine, Hospital
of Charles Nicolle Tunis. Tunisia.
2 Resident in Removable Partial Prosthodontics, Service of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia.
3 Resident in in Endodontics and Restorative Dentistry. Service of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia.
4 Professor in Removable Partial Prosthodontics, Faculty of Dental Medicine of Monastir, Department of Dental Medicine, Hospital of Charles Nicolle Tunis. Tunisia.
5 Professor in Endodontics and Restorative Dentistry, Faculty of Dental Medicine of Monastir, Departement of Dental Medicine, Hospital of Charles Nicolle Tunis. Tunisia.
6 Professor in Forensic Dentistry and Head of Service, Faculty of Dental Medicine of Monastir, Department of Dental Medicine. Hospital of Charles Nicolle Tunis. Tunisia.
*Corresponding Author
Rym Mabrouk,
Associate Professor in Endodontics and Restorative Dentistry, Faculty of Dental Medicine of Monastir,
Department of Dental Medicine. Hospital of Charles Nicolle Tunis. Tunisia.
Tel: (+216)55760730
E-mail: dr.rym.mabrouk@gmail.com
Received: April 28, 2020; Accepted: June 16, 2020; Published: June 18, 2020
Citation:Rym Mabrouk, Nihel Charfi, Souha Yahia, Rim Bibi, Afef Oueslati, Nadia Frih. Multidisciplinary Approach in Management of Fractured Anterior Teeth: Case Report. Int J Dentistry Oral Sci. 2020;7(6):762-765. doi: dx.doi.org/10.19070/2377-8075-20000149
Copyright: Rym Mabrouk©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Restoration of anterior non vital traumatized teeth represents one of the greatest challenges of the clinician. As there is a loss of structural integrity, loss of moisture, loss of dentin toughness and change in values for the Young modulus and even a reduction of the level of proprioception, endodontically treated teeth require special care during treatment. The prognosis of endodontically treated teeth depends not only on the success of the endodontic treatment but also on the type of reconstruction. Restoration of anterior non-vital teeth should respond to aesthetic, functional requirements while preserving the integrity of remaining tooth structure.Nowadays, there is an increasing looking for alternative methods to build up the core of non-vital teeth. One of the modern methods is fiber reinforced composite post (FRCP).
The purpose of this paper was to present a multi-multidisciplinary approach in restoring aesthetic and function of a fractured lateral incisor using fiber reinforced composite post and ceramic crown.
2.Introduction
3.Case Presentation
4.Discussion
5.Conclusion
6.References
Keywords
Nonvital Tooth; Trauma, Fiber Reinforced Composite Post; Ceramic Crown.
Introduction
Traumatism in anterior teeth refers to common lesions that lead to functional, esthetic and psychological sequelae frequently requiring multiple interventions. Traumatic impact on the anterior teeth often compromises their vitality leading to endodontic treatment [1, 2]. Non vital teeth are generally weaker than sound teeth because of loss of tooth structure caused by trauma and endodontic procedures [3]. Retreatment may cause additional loss to tooth tissue during the procedure and further weaken the tooth structure increasing the susceptibility to fracture during function. The fracture resistance of endodontically treated tooth is highly dependent on the remaining dentine thickness around post and core systems [4]. Teeth are more susceptible to fracture as the remaining walls are thin, and the restoration of these teeth requires techniques that will not compromise the integrity of the remaining radicular tooth structure. The restoration of endodontically teeth is often achieved with post and core when most ofthe coronal structure of endodontically treated teeth has been lost. The decision regarding the treatment plan and post insertion should be based onthree aspects: position of tooth in the arch, amount of remaining tooth structure and esthetic requirements. The main goal of the post insertion is to provide an optimum retention for the core which eventually supports the crown [3]. Failure of traditional metal post restorations are mainly caused by vertical root fracture because of the varying modulus of elasticity of the root structure and metal post or core [4-7]. Rigid metal posts resists to lateral forces without distorsion, resulting in stress transfer to the less rigid dentin and therefore potentially causing root fracture. Furthermore, the presence of a metal post can cause shadowing the soft tissues adjacent to the root surface and this adversely affects the esthetic outcome in the anterior region [8, 9]. Recently, the introduction of aesthetic fiber reinforced composite posts challenged conventional treatment modalities replacing metallic post and core. Thus, the main goal of this new build up protocol is, besides to responding to the aesthetic and functional requirements, preservation and reinforcement of the remaining sound tooth structure [10, 11]. The introduction of materials that can bond to dentine has created an alternative option for the reconstruction and rehabilitation of root canals. As bondable reinforcement fibers, they can be used to build up endodontic postsand cores; moreover, they adapt to the root canal walls without requiring additional enlargement of the root canal after endodontictreatment [4]. Their association with resin composite core besides esthetic properties would provide a positive behavior of the complex: tooth /post due to its modulus of elasticity (13, 5GPa) which is closer to the human dentin tissue [12]. Moreover, physical and functional properties are also establishing preventing restored teeth from excessive stress and fracture.
This paper’s aim was to describe and illustrate the clinical procedure of restoring endodontically treated traumatized lateral incisor using fiber reinforced composite post and ceramic crown.
Case Presentation
A 52 years old female presented in the department of Dental Medicine, Hospital of Charles Nicolle Tunis, Tunisia with a chief complaint: the fracture of her lateral left upper incisor 22. The history of the patient showed that the 22 was a root filled teeth with an old restoration of composite resin. Medical history was non-relevant. Intra-oral and extra-oral examination showed no apparent trauma of the soft tissue. Clinical and radiographic examination revealed that the trauma involved the cervical third of the anterior restoration of the 22, with a presence of an attached metallic screw post (Figure 1, a). At this stage the probing pocket depth was 3 mm and the width of attached gingiva was 4 mm. Crown lengthening with minor gingivectomy was planned exposing an additional 1 mm of tooth structure.
The restoration of the tooth with a fiber reinforced composite post and ceramic crown was proposed and discussed with the consent of the patient.
Canal retreatment was applied in the first meeting after the retrieval of the metallic post. Chemical and mechanical disinfection of the root canal system followed by an optimum sealing of the root canal system was achieved (Figure 1 b, c).
The following meeting, the restorative material was removed; the tooth was isolated with a rubber dam. Access cavity was opened and gutta percha was partially removed off the 2/3 of the canal system leaving an amount of 3 mm of the filling to maintain a good seal. A radiographic check confirmed that the gutta-percha has been removed (Figure 1d). The post was chosen basing on the volume of the canal and its placement was prepared using the correspondent post drill (Dentoclic drill, ITENA®) (Figure 1, e, f).
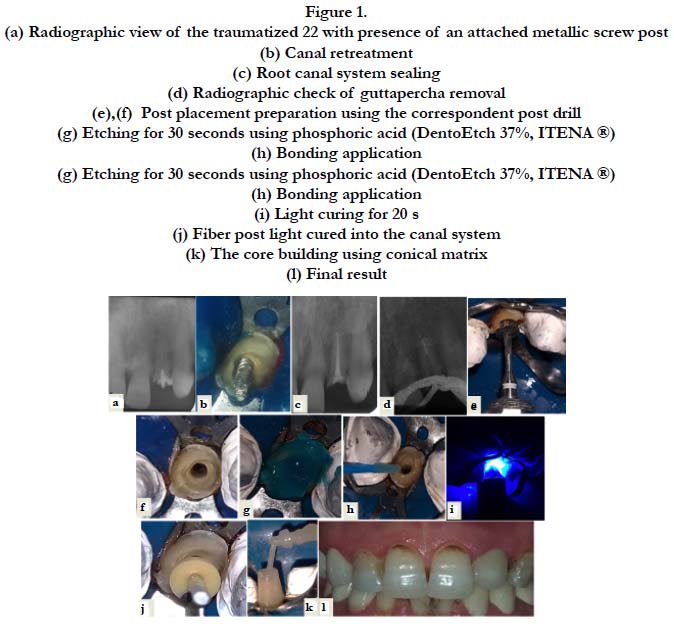
Figure 1.
Enamel and dentin were etched for 30 seconds using phosphoric acid (DentoEtch 37%, ITENA®) (Figure 1, g). The etchant was removed; the cavity and the root canal system were abundantly rinsed for 30 second directly collected into the aspiration. The canal was dried using paper points. The canal walls were coated with a mixture of (Iperbond Ultra Activator, ITENA) ® and (Iperbond Ultra,ITENA®), universal bond, dried gently for 5s using anoil-free compressed air to evaporate the volatiles. A second layer of the mixture was applied and dried for another 5s. Next, the canal system was light cure for 20s. (Figure 1,h,i). A universal adhesive system ( Iperbond Ultra, ITENA®) was placed carefully on the coronal cavity, gently air thinned to evaporate solvent and light cured for 20 s.
An adhesive dual curing luting composite resin (Dentocore Body, ITENA®) was injected in the canal system. The post, coated with (Silanea-ITENA®), was carefully seated into the canal using a light pressure. The complex fiber post- composite dual resin was light cured for 40s to ensure complete polymerization of the fiber composite complex into the canal (Figure 1,j). The core of the tooth was next built by the injection of the dual curing luting composite resin (Dentocore Body, ITENA®) the in the conical matrix previously adjusted (Figure 1, k). The next step involved the dental impression after the tooth preparation. A temporary crown was than cemented onto the tooth. The following meeting, the tooth was restored with an esthetic ceramic crown and the patient was satisfied by her new smile (Figure 1,l). For the restoration of her molars, a treatment plan involving implants and ceramic crowns was discussed with the patient in order to re-establish her function.
Discussion
A pleasing smile is a desirable part of overall appearance and self-esteem. The restoration of a traumatized anterior tooth may require minimally invasive or more extensive treatment options. The aim should be to provide a tooth restoration complex that closely mimics the functional and aesthetic qualities of an intact tooth for as long as possible.
The choice of the definitive restoration of traumatized teeth with a treated root canal system is strongly dependent of the amount of the remaining tooth structure, the morphology of the tooth, its position in the dental arch, functional and esthetic requirements [13]. It’s generally accepted that endodontically treated teeth with a minimal loss of coronal tooth structure should be restored conservatively with a direct composite resin to obturate the access cavity [13, 14]. Posts or crowns are not required until a great deal of teeth structure is lost as a result of caries or trauma since fracture resistance of endodontically treated teeth is mainly attributed to the remaining tooth structure. The current emphasis on preservation of natural dentition combined with successful endodontic treatment has resulted in various methods to restore non vital teeth with the evolution of new adhesive systems offering excellent bonding to the tooth surface. Now, the restoration of endodontically treated teeth has become simpler and shows good results. Fiber reinforced composite post can be a good alternative to conventional post systems [6].
Anterior teeth must resist to lateral and shearing types of forces, and the pulp chambers are too small to provide adequate retention and resistance without a post in case of a large coronal restoration [14-16]. The requirements for an ideal post and core system should consider physical properties such as modulus of elasticity, compressive strength and coefficient of thermal expansion that are close to that of dentin. Additionally, posts should demonstrate high retention good biocompatibility esthetics and retrievability [13]. Fiber reinforced composite posts consist of a resin matrix, in which structural reinforcing carbon or quartz/glass fiber are embedded. The main goal of fiber reinforced composite posts is to establish a unity among post, luting agent, root canal dentin and coronal restoration in order to imitate the original tooth structure. Moreover, fiber reinforced composite post have the advantage to avoid root fractures due to their modulus of elasticity close to that of dentin [13, 17]. The litterature reported that metal free esthetic fiber posts have been used with satisfactory results and demonstrated advantages compared with metal core posts including less rigidity with improved distribution of forces transmitted to the tooth minimizing the risk of root fracture reinforcement of the remaining tooth structure and improved esthetic properties ( such translucency refractive index and transmission of colors) [1]. The favorable optical properties of glass/quartz fiber posts, which are consistent with natural teeth in their ability to conduct light, optimize the purpose of esthetic restorations. It results in restoration with natural translucency without causing corrosion and discoloration with high biocompatibility [7].
This technique is easy to perform and safe for both patient and dentist. The post can be processed in a single visit that eliminates the laboratory step, due to the direct technique in combination with an adhesive composite build-up. This procedure seems to be noninvasive and preserving tooth residual tooth sound [18, 19].
Continuing improvement of adhesive systems in their performance and clinical applications results in reliable and reproductible clinical protocols. These reconstructions constitute within the limit of their indications, a real alternative to cast posts and cores [19].
Conclusion
The restoration of a traumatized anterior tooth may require minimally invasive or more extensive treatment options. The aim should be to restore aesthetics and function for the long term. Fiber post reinforced composite post is a conservative approach in restoring the endodontically treated teeth with minimal tooth tissue left. Knowledge of both curing and adhesive technique is the key to achieve this goal.
References
- Cohen-Carneiro F, Sponchiado EC, Garcia Ldo F, Yurtsever FV, Pontes DG, Sena A.Coronal reconstruction following anterior teeth traumatism: multidisciplinary treatment.Gen Dent.2013; 61(5):47-9. PMID: 25419251.
- Faria AC, Rodrigues RC, de Almeida Antunes RP, de Mattos Mda G, Ribeiro RF. Endodontically treated teeth: characteristics and considerations to restore them.J Prosthodont Res.2011; 55(2):69-74.PMID: 20709618.
- Belli S, Erdemir A, Yildirim C. Reinforcement effect of polyethylene fiber in root-filled teeth: comparison of two restoration techniques.Int Endod J.2006; 39(2):136-42.PMID: 16454794.
- Mortazavi V, Fathi MN, Shahnaseri S, Badrian H, Khalighinejad N, Najmeh Katiraei.Fracture resistance of structurally compromised and normal endodontically treated teeth restored with different post systems: An in vitro study.Dent Res J (Isfahan). 2012; 9(2): 185–191. PMID: 22623936.
- Liddelow G, Carmichael G. The restoration of traumatized teeth.Aust Dent J. 2016 Mar; 61 Suppl 1:107-19.PMID : 26923452.
- Deliperi S. Direct fiber-reinforced composite restoration in an endodontically-treated molar: a three-year case report.Oper Dent. 2008;33(2):209-14. PMID :18435197.
- Verma L, Passi S. Glass Fibre-Reinforced Composite Post and Core Used in Decayed Primary Anterior Teeth: A Case Report. Case Rep Dent.2011; 2011: 864254. PMID: 22567447.
- Gaikwad AP. Reinforcing esthetic with fiber post. International Journal of Dental Clinics.2011; 3(2):89-90.
- Zarow M, Ramírez-Sebastià A, Paolone G, de Ribot Porta J, Mora J, Espona J, et al. A new classification system for the restoration of root filled teeth. Int Endod J.2018 ; 51(3):318-334.PMID:28853160.
- Deliperi S, Bardwell DN. Reconstruction of nonvital teeth using direct fiber-reinforced composite resin: a pilot clinical study. J Adhes Dent. 2009; 11(1):71-8. PMID : 19343930.
- Ayna B, Celenk S, Atakul F, Uysal E.Three-year clinical evaluation of endodontically treated anterior teeth restored with a polyethylene fibre-reinforced composite.Aust Dent J. 2009; 54(2):136-40.PMID:19473155.
- D.Dietschi,S Bouillaguet. Restoration of the endodontically treated tooth. Cohen’s Pathways of the Pulp (10th Edtn). 2010; 777-807.
- Manhart J.Fabricating fiber-reinforced composite posts.Dent Today. 2011; 30(3):84, 86, 88-92.PMID :21485884.
- Deliperi S, Bardwell DN, Coiana C.Reconstruction of devital teeth using direct fiber-reinforced composite resins: a case report.J Adhes Dent. 2005; 7(2):165-71.PMID:16052766.
- Bitter K, Kielbassa AM. Post-endodontic restorations with adhesively luted fiber-reinforced composite post systems: a review.Am J Dent.2007; 20(6):353-60.PMID:18269124.
- Peroz I, Blankenstein F, Lange KP, Naumann M.Restoring endodontically treated teeth with posts and cores--a review.Quintessence Int. 2005; 36(9):737-46.PMID:16163877.
- T. Rocc, S.Bouillaguet. Alternative treatments for the restoration of non-vital teeth. Rev Odont Stomat. 2008; 37:259-272.
- Asmussen E, Peutzfeldt A, Heitmann T. Stiffness, elastic limit, and strength of newer types of endodontic posts.J Dent. 1999; 27(4):275-8. PMID:10193104.
- Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: a literature review.J Endod.2004; 30(5):289-301. PMID:15107639.





