Clinical and Radiographic Evaluation of the Extract of Allium Sativum in Pulpotomy of Primary Molars: A Randomized Clinical Trial
Ghada Rezk Gomaa1, Gehan G. Allam2*
1 Egyptian Ministry of Health.
2 Associate Professor of Pediatric Dentistry & Dental Public Health, Faculty of Dentistry Ain Shams University, Egypt.
*Corresponding Author
Gehan G.Allam,
Associate Professor of Pediatric Dentistry & Dental Public Health, Faculty of Dentistry Ain Shams University, Egypt.
Tel: 002/01223793534
E-mail: gigimm14@yahoo.com
Received: May 19, 2020; Accepted: June 18, 2020; Published: June 22, 2020
Citation:Ghada Rezk Gomaa, Gehan G. Allam. Clinical and Radiographic Evaluation of the Extract of Allium Sativum in Pulpotomy of Primary Molars: A Randomized Clinical Trial. Int J Dentistry Oral Sci. 2020;7(6):747-752. doi: dx.doi.org/10.19070/2377-8075-20000147
Copyright: Gehan G. Allam©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The objective of this study was to evaluate the potential success of A. sativum extract and compare it to formocresol as pulpcapping agent after pulpotomy of primary molars.
Materials and Methods: A total of 68 primary molars indicated for pulpotomy in children aged from 4 to 7 years were included in the study. In every molar, pulpotomy procedure was performed, and the radicular pulp tissue of molars in group (A) was capped with A. sativum extract, whereas it was capped with formocresol in molars of group (F). Then the pulpotomized molars in both groups were evaluated clinically and radiographically at 6 and12 month, using standard clinical and radiographical criteria.
Results: Vital pulpotomy of primary molars with Allium sativum extract was given 88.3% success rate while that with formocresol was 89.3% after 12 months. Statistically, the results revealed no significant radiographic difference between the two materials.
Conclusion: A. sativum extract is a biocompatible material that is compatible with vital human pulp tissue. It offers a good healing potential comparable to formocresol (the gold standard).
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusions
7.References
Keywords
Allium Sativum; Formocresol; Pulpotomy.
Introduction
Dental extraction is the most common form of treatment options of exposed carious primary molars in developing countries in spite of its negative consequences for both dentitions which occur from this premature loss of primary teeth [1-3].
The primary objective of pulp therapy is to maintain the vitality of the pulp of an affected carious tooth by so preserving its integrity and health [4-6].
During pulpotomy, the coronal pulp is amputated, and the remaining vital radicular pulp tissue surface is treated with manyclinically-successful medicaments such as ferric sulfate, MTA, sodium hypochlorite,etc. However, none of them had met the same degree of effectiveness and success rate as formocresol which is considered the gold standard, but due to its possible hazards (cytotoxicity, carcinogenicity, immunologic…), the demand for natural medicament to replace it as a pulp dressing material become essential [7, 8].
One of the most widely researched plants in the field of medicine is Allium sativum (Garlic). The oil of this plant was recently used in pulpotomy. The antibacterial effects of the fresh garlic extract have been thoroughly researched via literature and have been found that the extract will inhibit growth of various Grampositive and Gram-negative bacteria [9-12].
To our knowledge, no study has been conducted to evaluate the extract of A. sativum in vital pulpotomy in primary molars.
That is why the aim of this study was to evaluate A. sativum extract clinically and radiographically and compare it to formocresol in vital pulpotomy in primary molars.
Aqueous garlic extract was prepared in Oncology Diadnostic Unit, Faculty of Medicine, Ain Shams University, Egypt. Fresh garlic bulbs were extracted according to the Bakri and Douglas method with minor modifications [13]. Garlic bulbs were peeled, cleaned, washed, dried and blended. 5 grams of the blended garlic were taken and after which 10 ml of sterile water was added. Then, for 30 minutes rotation was applied at a frequency of 1-minute rotation and 2-minute break until a dough-like mixture obtained.Then the dough was placed on a 15 cm What man filter paper to be filtered.10 ml of aqueous garlic extract was obtained, diluted to reach concentration of 8μ/ml. Finally, the produced extract was sterilized via a bacteriological millipore filter in the Department of Microbiology, Faculty of Pharmacy, Ain Shams University, Cairo, Egypt and then kept in refrigerator until use [13, 14].
An approval was obtained from the Ethical Committee of Dental Research at the Faculty of Dentistry, Ain Shams University. Informed consent and assent were obtained from caregivers prior to initiation of the investigation.
The predicted sample size (n) was a total of (46) cases i.e. (23) cases per group. Sample size calculation was performed using G*Power version 3.1.9.2.
About one hundred primary molars indicated for pulpotomy in patients with age ranged from 4 to 7 years were screened from outpatient clinic of Pediatric Dentistry Department, Faculty of Dentistry, Ain Shams University, Egypt. From these molars, sixty eight were randomly allocated by using computer generated random numbers into 2 groups similar to each other in all aspects except in the medicament used for the pulpotomy procedure.
A comprehensive medical and dental history was obtained. A thorough clinical examination was conducted. A periapical radiograph of the intended tooth was achieved before treatment using standardized parallelling technique.
1. Patient and parent cooperation.
2. At least one primary molar needs pulpotomy therapy and stainless steel crown restoration.
3. Free medical history.
4. Absence of clinical signs or symptoms suggesting a non-vital tooth such as:
• Spontaneous pain
• Tooth mobility
• Soft tissue swelling
• Tenderness to percssion
• History of facial swelling or
• Unsuccessful hemorrhage control [9, 15].
1. Symptomatic tooth (presently or history of symptoms).
2. Previous pulpal treatment on the tooth.
3. Necrotic pulp (9).
1. Absence of pathological external or internal root resorption.
2. Absence of periapical radiolucency.
3. No furcation involvement.
4. No calcific pulp degeneration.
5. No widening of periodontal membrane space [9, 15].
Molars to be treated in both groups were locally anaesthetized using one carpule of Septanest SP - France (contains articaine hydrochlorite 4% with 1:100,000 epinephrine). After the tooth was isolated with rubber dam, cavity outline was established with a sterile high-speed large sized (5 or 6) round shaped carbide bur with air/water spray [9]. All caries was removed. Access to pulp chamber was done followed by removal of pulpal roof and removal of the coronal pulp tissue was achieved using large sharp spoon excavator. Hemorrhage control was obtained by applying light pressure to dry, sterile cotton pellets placed over the pulpal stumps for 5 minutes [15].
Following hemostasis, pulp stumps were dressed with a cotton pellet damped with one drop of either 2 medicaments according to the sample group in which the treated molar was included:
• Group A: the cotton pellet was damped with one drop of A. sativum extract for 5 min [9].
• Group F: the cotton pellet was damped with one drop of formocresol for 5 minutes.
Then the pellet was removed, and the pulp stumps of molars treated were dressed with a thick paste prepared by:
• Group A: mixing one spoon of zinc oxide powder with one drop of A. sativm extract
• Group F: mixing one spoon of zinc oxide powder with one drop of eugenol [5].
Molars of both groups were restored with a suitable intermediate restorative material (zinc phosphate base) and then with stainless steel crowns and cemented with glass ionomer cement [15].
Clinical success was evaluated at 6 and at 12 month by:
1. No history of pain related to the treated molar.
2. Intact restoration.
3. No sensitivity to percussion.
4. Absence of tooth mobility.
5. No signs of erythema, swelling or the presence of the fistulous tract in the surrounding gingival tissues and mucosa [16, 17].
All treated molars were followed up, by radiographic examination using the previously mentioned paralleling technique. Radiographic follow up was performed at 6 and 12 month. Radiographic success was determined by the following criteria:
1. Absence of periapical radiolucency.
2. No interradicular bone destruction.
3. Absence of pathologic internal or external root resorption.
4. Absence of widening in the periodontal membrane [5, 16, 17].
Statistical analysis was performed between the clinical and radiographic effects of A.sativum extract and those of formocresol in vital pulpotomy in primary teeth using Chi-square, and the level of significance was taken at α = 0.05.
After 12 month, statistical analysis revealed no significant difference between the incidences of clinical findings in both groups.
Comparisons between the clinical findings of vital pulpotomy in primary molars treated with A. sativum extract and those of formocresol are presented in Figure (1). Statistical analysis revealed no significant difference.
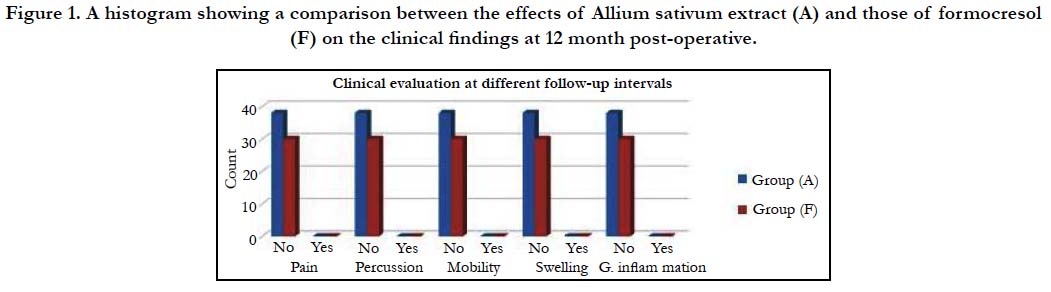

Figure 1. A histogram showing a comparison between the effects of Allium sativum extract (A) and those of formocresol (F) on the clinical findings at 12 month post-operative.
Odds Ratio of Clinical Findings at Different Follow-up Intervals:
Odds of clinical findings at different follow-up intervals were presented in table (1)
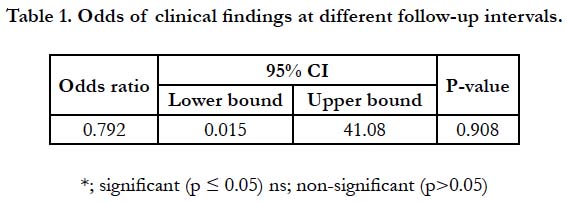

Table 1. Odds of clinical findings at different follow-up intervals.
Comparisons between the radiographic findings of vital pulpotomy in primary molars treated with A. sativum extract and those of formocresol after 6 month are presented in Figure (2).
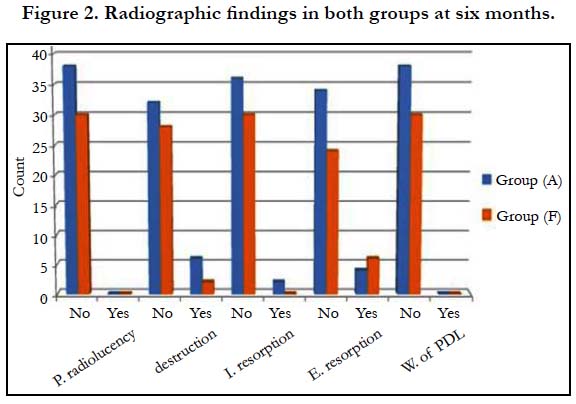
Figure 2. Radiographic findings in both groups at six months.
Odds of radiographic findings at six month were presented in table (2). Group (A) had lower odds ratio of developing periapical radiolucency, widening of periodontal membrane and pathologic external root resorption. While group (F) had lower odds of developing inter radicular bone destruction and pathological internal root resorption. There was no statistical difference between both groups for all findings as the p-value was non-significant. Statistically, there was no significant difference between the incidences of radiographic findings in both groups after 12 month figure (3).
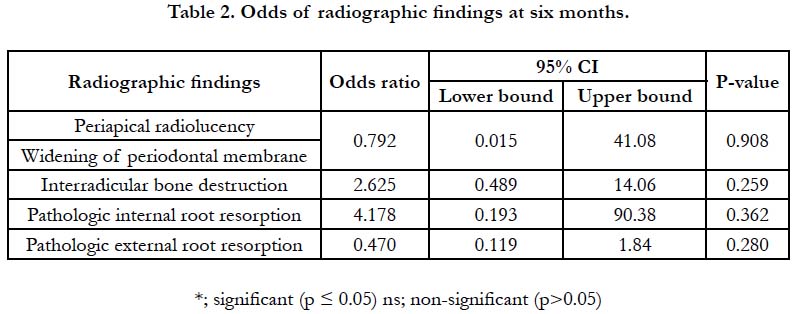
Table 2. Odds of radiographic findings at six months.
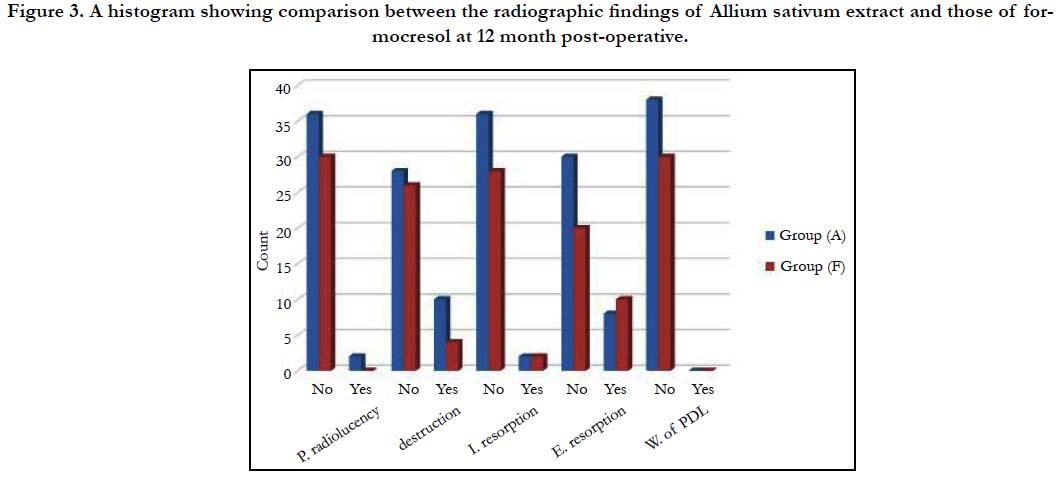
Figure 3. A histogram showing comparison between the radiographic findings of Allium sativum extract and those of formocresol at 12 month post-operative.
The majority of the participants of both groups did not show radiographic findings (Figures 4, 5). Pairwise comparisons showed that all the participants of both groups did not show widening of periodontal membrane. Group (F) showed a higher percentage of participants who did not show periapical radiolucency and inter radicular bone destruction. While Group (A) had a higher percentage of participants who did not show pathologic internal and external root resorption table (3).
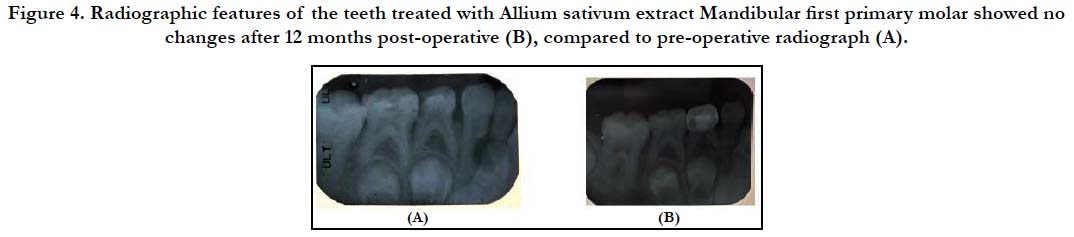
Figure 4. Radiographic features of the teeth treated with Allium sativum extract Mandibular first primary molar showed no changes after 12 months post-operative (B), compared to pre-operative radiograph (A).
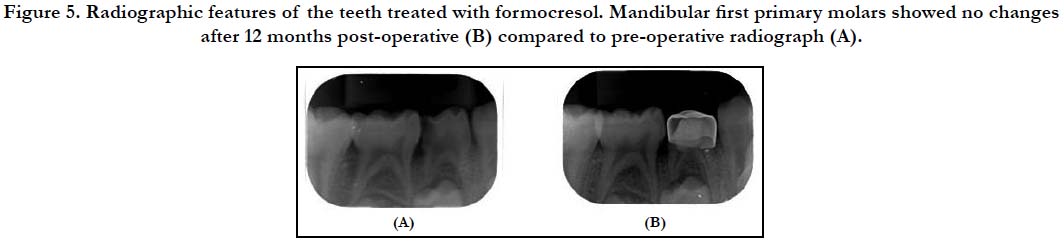
Figure 5. Radiographic features of the teeth treated with formocresol. Mandibular first primary molars showed no changes after 12 months post-operative (B) compared to pre-operative radiograph (A).
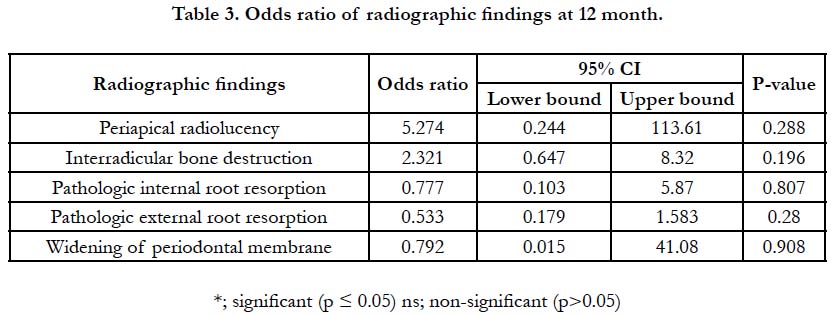
Table 3. Odds ratio of radiographic findings at 12 month.
Discussion
In the present study, a randomized clinical trial was done to evaluate the effect of Allium sativum extract pulpotomy clinically and radiographically and compare it to the formocresol (the gold standard).
In our study we chose to use the extract not the oil as previous studies, as we believe it will be more effective. The aqueous Allium sativum extract applied in the current study was manually fabricated and sterilized to ascertain the exact quality and quantity as well as sterilization of the included ingredients [17].
The concentration of the extract that was used in the present study was 8μ/ml. This concentration was selected according to the study done by Ramezan AA et al [14]; as it was the minimum inhibitory concentration for bacterial strains determined when he evaluated the antibacterial effect of Allium Sativum extract on isolated bacteria from an operating room.
For radiographic assessment, a standardized paralleling technique was applied to ensure maintenance of the same vertical dimension post-operative as well as during the follow up period. A digital system was used for patient safety to decrease the patient radiational exposure and to eliminate the detrimental effects on improper film processing on its diagnostic quality. Size 0 film was used to be comfortable in the smaller floor of mouth in children and did not cause pain thus ensuring more patient cooperation.
Natural agents used in pulpotomy have been a recent trend and they are reporting a great clinical success that appears to be a viable replacement to formocresol. From these agents is honey,Kumari et al., (18) reported 100% clinical success rate and 91.3% radiographic success rate of honey as a pulpotomy agent at 6 months interval. Also Purohit et al., (19), used turmeric powder in pulpotomy of primary molars which gave 100% success rate both clinically and radiographically at 6 months interval.
In our study pulpotomy using Allium sativum extract showed a clinical success rate of 100% and a radiographic success rate of 88.3% after 12 months with no statistical difference comparing to formocresol pulpotomy which revealed 100% clinical success rate and 89.3% radiographic success rate after 6 months follow up [20].
This success rate can be explained that garlic extract has strong antioxidant and anti-inflammatory effects. The high polyphenol and flavonoids content present in the extract are responsible for its antioxidant potential, which are essential for the synthesis of collagen, angiogenesis, and the inhibition of inflammation.
These results were approximating to those given by Shukry Gamal M et al., [9], who used the oil of the same herb (Allium sativum oil) in vital pulpotomy of primary molars. The oil gave 90% clinical and radiographic success rate at 6 month follow up period.
Conclusions
Since there were no statistically significant differences at 6 and 12 month follow up between primary molar pulpotomies performed with formocresol and aqueous Allium sativum extract clinically and radiographically, aqueous Allium sativum extract can be used in pulpotomy as an alternative to formocresol pulpotomy.
Further randomized clinical trials with different concentrations utilizing aqueous Allium sativum extract as a pulpotomy agent with longer follow up periods are recommended.
References
- Sandra Aremy López-Gómez, Juan José Villalobos-Rodelo, Leticia Ávila-Burgos, Juan Fernando Casanova-Rosado, Ana Alicia Vallejos-Sánchez, Salvador Eduardo Lucas-Rincón, et al. Relationship between premature loss of primary teeth with oral hygiene, consumption of soft drinks, dental care, and previous caries experience.Sci Rep. 2016; 6: 21147. PMID: 26916132.
- Arikan V, Kizilci E, Ozalp N, Ozcelik B. Effects of Fixed and Removable Space Maintainers on Plaque Accumulation, Periodontal Health, Candidal and Enterococcus FaecalisCarriage. Med Princ Pract. 2015;24(4):311-317. PMID: 26044443.
- Silva PV, Noberto JSL, Del Papa ABR, Simões CAD, Berger SB, Aranha AMF. Aesthetic-Functional Fixed Appliance as Treatment of Premature Loss of primary Anterior Teeth.J Health Sci. 2019Dec 20;21(5):454-8.
- López-Gómez SA, Villalobos-Rodelo JJ, Burgos LA, Casanova-Rosado JF, Vallejos-Sánchez AA, Lucas-Rincón SE, et al. Relationship between premature loss of primary teeth with oral hygiene, consumption of soft drinks, dental care, and previous caries experience. Sci Rep. 2016; 6: 21147. PMID: 26916132.
- Fuks AB, Kupietzky A, Guelmann M. Pulp therapy for the primary dentition. InPediatric Dentistry 2019 Jan 1; 329-351.
- Mctigue DJ, Nowak AJ, Fields HW, Casamassiomo PS. Pediatric dentistry: Infancy through adolescence (5th Edtn), Missouri: Elsevier. 2013;45.
- Subcommittee PT, Clinical Affairs Committee, American Academy of Pediatric Dentistry. Guideline on pulp therapy for primary and immature permanent teeth. Reference Manual. 2014 Apr 24;37(6):244-52.
- Hugar SM, Kukreja P, Hugar SS, Gokhale N, Assudani H. Comparative Evaluation of Clinical and Radiographic Success of Formocresol, Propolis, Turmeric Gel, and Calcium Hydroxide on Pulpotomized Primary Molars: A Preliminary Study. Int J Clin Pediatr Dent. 2017;10(1):18–23. PMID: 28377649.
- Shukry Gamal M, RaheelSA, Baroudi K. Clinical and radiographic evaluation of Allium sativum oil as a new medicament for vital pulp treatment of primary teeth.J Int Oral Health. 2014;(6):32-36. PMID: 25628480.
- Wen-Ru Li, Qing-Shan Shi, Huan-Qin Dai, Qing Liang, Xiao-Bao Xie, Xiao- Mo Huang, et al. Antifungal activity, kinetics and molecular mechanism of action of garlic oil against Candida albicans. Sci Rep. 2016; 6:22805.
- Marčetić M, PetrovićS, Milenković M, Niketić M. Composition, antimicrobial and antioxidant activity of the extracts of Eryngium palmatum Pančićand Vis. (Apiaceae). Open Life Sciences. 2014;9:149–155.
- Mohammad Sadegh Safari, Mehrnaz Keyhanfar, Rasoul Shafiei. Investigating the antibacterial effects of some Lactobacillus, Bifidobacterium and acetobacter strains killed by different methods on Streptococcus mutans and Escherichia coli. J Indian Mol Biol Res Commun. 2019;8(3):103-111. PMID: 31998811.
- Hassan Mohamed1, El Amin Ibrahim Elnima, Ibrahim Ahmed. Inhibitory Effect of Garlic Extract on Porphyromonas Gingivalis Isolated from Sudanese Aggressive Periodontitis Patients Compared to Chlorhexidine Digluconate 0.2%. J. Chem. Pharm. Res.2017; 9(4):259-263.
- Ramezan AA, Hassan Araqizade, Rezvan Yoosefi, Ali MT, Mohammad HA.Effect of Allium sativum extract on Erythromycin and Methicillin resistant bacteria isolated from hospital operating room; J Med Bacteriol. 2016;5:7-14.
- Tzu-Ying Li, Li-Chuan Chuang, Aileen ITsai. A retrospective study of sodium hypochlorite pulpotomies in primary molars. Journal of Dental Sciences. 2016; 11: 261-265. PMID: 30894982.
- Dhar V, Marghalani AA, Crystal YO, Kumar A, Ritwik P, Tulunoglu O, et al. Use of vital pulp therapies in primary teeth with deep caries lesions. Pediatr Dent. 2017;39(5):e146-e159.
- Bandi Madhuri, Mallineni Sreekanth Kumar, Nuvvula Sivakumar.Clinical applications of ferric sulfate in dentistry: A narrative review.J Conserv Dent. 2017; 20(4): 278-281. PMID: 29259368.
- Kumari KK, Sridevi E, Sai Sankar AJ, Gopal AS, Pranitha K, Manoj Kumar M G. In vivo evaluation of honey as a new medicament for vital pulp therapy in primary teeth. SRM J Res Dent Sci. 2017; 8(2): 58-63.
- Purohit Rajiv N, Bhatt M, Purohit K, Acharya J, Kumar R, Garg R. Clinical and radiological evaluation of Turmeric powder as a pulpotomy medicament in primary teeth: An in vivo Study. Int J Clin Pediatr Dent. 2017; 10(1):37-40.
- Sahbaz A, Isik H, Aynioglu O, Gungorduk K, Gun BD. Effect of intraabdominal administration of Allium sativum (garlic) oil on postoperative peritoneal adhesion. Eur J Obstet Gynecol Reprod Biol. 2014;177:44-7. PMID: 24793933.





