Maxillary Expansion Effects on Mandibular Transverse Dimension: Comparison of Different Activation Protocols
Ugolini A*
Department of Orthodontics, University of Genoa, Italy.
*Corresponding Author
Alessandro Ugolini,
Faculty of Dentistry, College of Medicine,
Department of Orthodontics, University of Genoa, Italy.
Tel: 3475971340
E-mail: alessandro.ugolini@unige.it
Received: February 25, 2020; Accepted: March 17, 2020; Published: March 26, 2020
Citation:Alessandro Ugolini. Maxillary Expansion Effects on Mandibular Transverse Dimension: Comparison of Different Activation Protocols. Int J Dentistry Oral Sci. 2020;7(3):733-736. doi: dx.doi.org/10.19070/2377-8075-200000144
Copyright: Alessandro Ugolini©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The purpose of this prospective study was to investigate medium-term indirect effects of Maxillary Expansion (RME) therapy on mandibular arch dimensions using two different clinical protocol activation. Sixty patients in mixed dentition (mean age 7.8 y) showing maxillary deficiency and/or unilateral or bilateral cross-bite were treated with RPE (Haas type) on second deciduous molars. For patient in RME group (rapid maxillary expansion), treatment protocol consisted of 2 turns per day: For patient in SME (slow maxillary expansion) group treatment protocol consisted of 2 turns per week. Study models were taken before (T1) and after expansion (T2) with 12 ± 4 months interval. Dental cast were digitized with a 3D scanner (3Shape, DK) and a set of landmarks was digitized on each digital model. Mandibular intermolar distance (MID), mandibular molar torque (MMT), mandibular intercanine distance (MIcD) and mandibular canine torque (MCT) were assessed. At T1, no differences at baseline were found between groups. At T2, in RME group, mandibular intermolar distance (MID) increased 1.2 mm and MMT increased 6.5°. In SME group MID increased 1.3 mm and mandibular molar torque (MMT) increased 6.2°. There was a significant effect on mandibular intercanine distance (MIcD) (RME +0.8 mm, SME +0.9 mm) and on and mandibular canine torque (MCT) (RME +3.4°, SME +3.8°). The improvement in transversal and torque measurement did not differ between groups. In conclusion, both rapid and slow maxillary expansion protocols have a significant medium-term widening effect on the mandibular first molars and canines.
2.Introduction
3.Materials and Methods
4.Statistical Analysis
5.Results
6.Discussion
7.Conclusion
7.References
Abbreviations
Dentistry; Orthodontics; Rapid Expansion; Slow Expansion; Mandibular Transverse Dimension; Craniofacial
Growth; Digital Dental Casts.
Introduction
Maxillary expansion is a well recognize efficient therapy to treat skeletal maxillary deficiency [1, 2] and dental and skeletal crossbite [3-5] with a few side effects [6, 7], such functional impairments, injuries to the periodontal tissues and pain [8-11]. Maxillary expansion efficacy in widening the transverse dimension of the maxilla has been extensively reported in literature, both in the short and long term [3, 4, 12]. Several studies also claim for a spontaneous indirect widening effect on the transverse dimension of the mandible. Some Authors [13, 14] postulated as spontaneous mandibular transverse widening effect is due to occlusal changes in the maxillary arch that forcing the mandibular molars toward a buccal inclination. Other theories attributed the widening effect to a change of extra-oral tissue stiffness and masticatory muscles cinematics mediated by expansion of the maxillary arch (lip-bumper effect), causing a buccal inclination of the mid and posterior lower teeth [15]. Haas [16] was the first to report a spontaneous increase in buccal inclination of mandibular teeth after rapid maxillary expansion in pigs. In 1977 the study Wertz and Dreskin [17] assessed a mandibular intermolar increase of 0.46 mm as a short-term result of maxillary expansion, while in the long term (48 months) there was no difference between treated patients and controls. Gryson [14] in a short term clinical study evaluated the effect of maxillary expansion on mandibular arch compared to an historical control group [18] and reported a significant increase (+0.31 mm) in intermolar mandibular width , but a non-significant difference in intercanina width (+0.17) Adkins et al., [13] reported a slight indirect buccal uprighting of the mandibular molars, caused by to the modification in occlusal contacts and forces. Lima and co-Authors [19] carried out a long-term study on the effect of maxillary expansion on mandibular arch and their findings corroborated the long-term spontaneous mandibular response after palatal expansion in patients with transverse maxillary skeletal discrepancies. Most of the cited studies were designed to assess rapid maxillary expansion and its skeletal and dentoalveolar effects but mandibular changes were reported only as a side effect. Aim of the present study is to describe the differences in the medium-term effects of maxillary expansion on the mandibular arch using two expansion protocol (rapid and slow).
Materials and Methods
Sixty patients in mixed dentition showing maxillary deficiency and/or unilateral or bilateral cross-bite were included in the study. Subjects were divided in 2 group according to their maxillary expansion protocol. RME group were treated with rapid maxillary expansion protocol comprised 30 subjects (13 male and 17 females, mean age 7.5 ± 0.8 years); SME group were treated with slow maxillary expansion protocol comprised 30 subjects (14 male and 15 females, mean age 8.1 ± 0.9 years). The patients were consecutively treated in orthodontic private practice private practice between 2016 and 2019 and were selected according to the following criteria: maxillary deficiency and/or unilateral or bilateral cross-bite; early or mixed dentition stage; cervical vertebral stage 1 through 3 (CVS method 1-3); underwent rapid or slow maxillary expansion therapy (Haas type,); no subsequent comprehensive orthodontic treatment was implemented in either the maxilla or the mandible. The exclusion criteria for selection were: previous orthodontic treatment; hypodontia in any quadrant excluding third molars; arthritis or craniofacial abnormalities (e.g. cleft lip and palate). Three-dimensional digital dental casts were obtained pretreatment (T1) and post-treatment (T2, 12±4 months interval). The maxillary expanders were cemented and activated according to the following protocol: the appliances in the RME group was activated 2 quarter turns per day (0.4 mm/day). The appliances in the SME group was activated 2 quarter turns per week (0.4 mm/ week). Expansion was considered adequate when the occlusal aspect of the maxillary lingual cusp of upper first molars contacted the occlusal aspect of the facial cusp of the mandibular lower first molars. Then the appliance remained in situ for a retention period of 12 ± 4 months. Cast Analysis. The sample consisted of 120 cast models scanned by a 3SHAPE D640 SCANNER (3 Shape, Copenhagen, DK) 3D digital model (*.stl) were thus obtained. 3D digital model assessment was cast analysis were accomplished with a multi-step analysis reported in a previous study [20]. Briefly, the first step consisted of points input on each model via inForm™ (Vectra System Software).
The whole set of points was then exported into a .txt file. The .txt file was imported into an Excel matrix and data for the x, y and z axis were divided into three columns. Data were then divided on a tooth by tooth basis inserting manually a 3D point close to the origin (thus having x, y and z values close to 0). The task could be semi-automatically accomplished with an Excel Matrix. Finally, the .xls file was analysed with a custom software for 3D arch analysis (Figure 1).
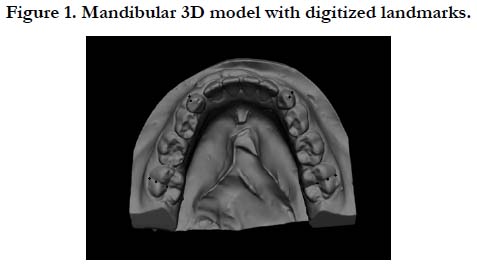

Figure 1. Mandibular 3D model with digitized landmarks.
The process can be repeated for each model (upper and lower arch) to build a whole set of data which can be statistically analyzed to check for the influence of maxillary expansion on the mandibular arch. Measurements were made directly on scanned maxillary and mandibular dental casts allowed the data to be directly digitized in the ad-hoc software with a spreadsheet program. If cusp tips were worn, the centers of the resulting facets were used as landmarks. When either the deciduous teeth were missing or the permanent teeth were not fully erupted, the measurement for that variable was eliminated. Lingual measurements for mandibular intermolar width were made at the point of the intersection of the lingual groove with the cervical gingival margin and for intercanine width at the cervical margins of the tooth from the point of greatest convexity bilaterally, according to Mc- Dougall et al., [21]. The occlusal intermolar width was measured as the distance between mesiobuccal cusps tips of the first permanent molars bilaterally and the intercanine width as the distance between cusp tips bilaterally. Additional maxillary intermolar arch width data from the same patients and measured the same way were obtained from mandibular cast. Moreover, mandibular and maxillary molar and canine torque was obtained. Two points per teeth allowed to trace the Facial Axis Clinical Crown (FACC) of the first molars and the deciduous canines. Also, three lingual point were used as a reference point.
Method error. Measurements were repeated on 8 randomly selected casts to determine error of the method between first and second measures. Standard deviations were found to be in the range of 0.07 to 0.18 mm for all measurements (average variation, 0.1 mm). Clinically, 0.1 mm is not considered significant. Intraclass correlation coefficients were calculated to compare withinsubjects variability to between-subjects variability, were greater than 0.95.
Statistical Analysis
Descriptive statistics were computed for each mandibular variable: vestibular and lingual intermolar distance; intercanine distance; molar and canine mean torque values. Shapiro-Wilks test showed that data were normal distributed, therefore parametric statistics were applied. Patients’ data were compared between groups using parametric t-tests. Probabilities of less than 0.05 were accepted as significant in all statistical analyses. The power of the study was adequate (greater than 0.85), calculated a priori using the mean values and standard deviations of mandibular molar expansion after RME therapy found by Ugolini et al., [20], at an alpha of .05.
Results
Descriptive analyses of the mandibular variables at two assessment stages for all 60 subjects are shown Table I. Only fully erupted teeth were assessed and if a deciduous tooth was replaced during the treatment no measurement was taken. According to this inclusion protocol for MID and MMT the sample was RME=27, SME=26; for MIcD and MCT the sample was RME=26, SME=25.
At T1, no differences at baseline were found between groups. At T2, in RME group, mandibular intermolar distance (MID) increased 1.2 mm and MMT increased 6.5°. In SME group MID increased 1.3 mm and mandibular molar torque (MMT) increased 6.2°. There was a significant effect on mandibular intercanine distance (MIcD) (RME +0.8 mm, SME +0.9 mm) and on and mandibular canine torque (MCT) (RME +3.4°, SME +3.8°). The improvement in transversal and torque measurement did not differ between groups (Table 2).
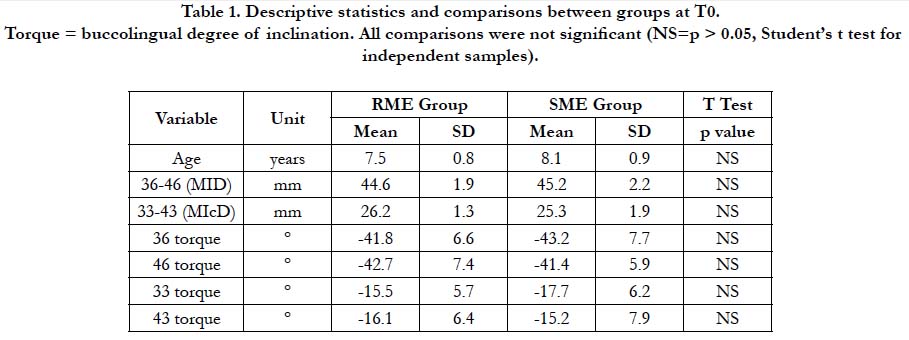

Table 1. Descriptive statistics and comparisons between groups at T0. Torque = buccolingual degree of inclination. All comparisons were not significant (NS=p > 0.05, Student’s t test for independent samples).
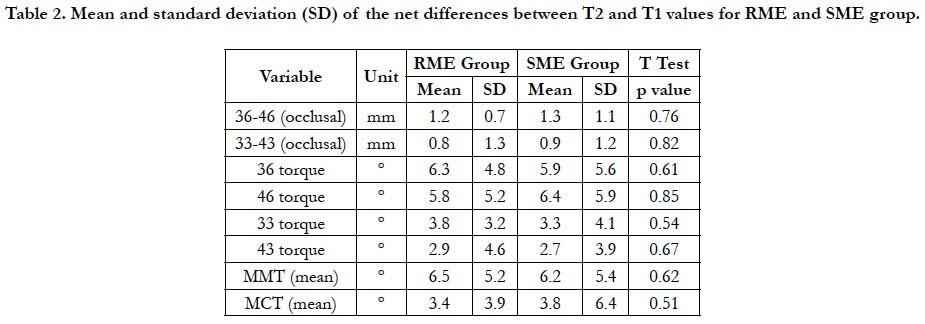
Table 2. Mean and standard deviation (SD) of the net differences between T2 and T1 values for RME and SME group.
Discussion
Indirect and spontaneous mandibular response after maxillary expansion has been reported in several studies as treatment side effect [14, 17, 22] and very few published studies focused their assessment of this topic [19, 20]. In this study, we assessed the medium term spontaneous mandibular response after maxillary expansion therapy with two different activation protocol (rapid and slow). Mandibular intermolar/canine distance and molar/canine torque were analysed and results were compared with other expansion studies and with longitudinal studies of untreated subjects.
In this study, RME group and SME, from pre-expansion (T1) to the post expansion (T2), showed a significant increase (p<0.01) for all the variables considered: RME group reported MID + 2.2 mm, MMT + 11°, MIcD + 1.2mm, MCT + 4.9°; SME group reported MID + 1.7mm, MMT + 10°, MIcD + 1.1mm, MCT + 4.2°. These increases were comparable or greater than the mandibular widening values previously reported.
From T1 to T2, increases mentioned above in both in RME and SME group suggest a slight uprighting and this hypothesis is corroborated by the torque values. From T1 to T2 mandibular molar and canine torque were significantly increased (molars: RME + 11°, SME + 10°; canines: RME + 4.9°, SME + 4.2°). Ulrich [23] reported a 0.99 mm intermolar width increase and Sandstrom et al., [24] and Moussa et al., [25], showed larger increases in intermolar width 2.3 and 2.8 mm, respectively. These values, comparable with those found in the present study, should be compared with growth mandibular values reported in the longitudinal studies of untreated patients. Sinclair and Little [26] found no significant increases in intermolar width for male patients, whereas female patients showed a statistically significant loss of 0.88 mm. The analysis of the intercanine width showed a little effect on intercanine distance on canine torque values. Similar results were reported by Lima et al., [19]. In contrast, Haas [22] reported no change for intercanine width in 50% of the sample analyzed; however, the age range was 9 to 18 years, rather than 6.7 to 9.1 years in the present study. Most of the studies that reported molar intercanine distance, showed very scattered value for these variables, ranging from 0.5 to 5 mm, which might be attributed mainly to the differences in sample selection. Ulrich [23] reported an increase in intercanine width of 0.69 mm, in contrast Haas [22] found an increase up to 5 mm. Moussa et al., [25] suggested as the width increase induced by the active expansion, tends to decrease in and after the retention period, as similarly occurs in untreated patients during growth. In fact Moussa et al., [25] reported that intercanine width increase at post-treatment of 1.8 mm, followed by a decrease of 1.1 mm post-retention, with a mean net loss of 0.7 mm. Studies on untreated subjects [18, 27], reported continues decrease in the intercanine width (0.5-1.5 mm) during the maturation of the permanent dentition. And Sinclair and Little [26] found that intercanine width have a decrease more in female than in male patients aged from 13 to 20 years.
Conclusion
Mandibular arch width increased significantly after maxillary expansion with a Haas-type appliance with both rapid and slow activation protocol. There were a significant widening effects on molar and intercanine distance and on molars and canine torque.
References
- Silvestrini-Biavati A, Angiero F, Gambino A, Ugolini A. Do changes in spheno-occipital synchondrosis after rapid maxillary expansion affect the maxillomandibular complex?. Eur J Paediatr Dent. 2013 Mar;14(1):63-7. Pubmed PMID: 23597224.
- Kilic N, Oktay H. Effects of rapid-slow maxillary expansion on the dentofacial structures. Aust Orthod J. 2010 Nov;26(2):178-83. Pubmed PMID: 21175029.
- Agostino P, Ugolini A, Signori A, Silvestrini-Biavati A, Harrison JE, Riley P. Orthodontic treatment for posterior crossbites. Cochrane Database Syst Rev. 2014 Aug 8;(8):CD000979.
- Cerruto C, Ugolini A, Di Vece L, Doldo T, Caprioglio A, Silvestrini-Biavati A. Cephalometric and dental arch changes to Haas-type rapid maxillary expander anchored to deciduous vs permanent molars: a multicenter, randomized controlled trial. 2017 Sep;78(5):385-393. Pubmed PMID: 28397083.
- Ugolini A, Cerruto C, Di Vece L, Ghislanzoni LH, Sforza C, Doldo T, Silvestrini- Biavati A, Caprioglio A. Dental arch response to Haas-type rapid maxillary expansion anchored to deciduous vs permanent molars: a multicentric randomized controlled trial.Angle Orthod. 2015 Jul;85(4):570-6. Pubmed PMID: 25314034.
- Ugolini A, Salamone S, Agostino P, Sardi E, Silvestrini-Biavati A. Trends in early childhood caries: an Italian perspective. Oral Health Prev Dent. 2018 Jan 1;16(1):87-92. Pubmed PMID: 29459908.
- Feldmann I, Bazargani F. Pain and discomfort during the first week of rapid maxillary expansion (RME) using two different RME appliances: A randomized controlled trial. Angle Orthod. 2017 May;87(3):391-396. Pubmed PMID: 28029266.
- Silvestrini-Biavati A, Salamone S, Silvestrini-Biavati F, Agostino P, Ugolini A. Anterior open-bite and sucking habits in Italian preschool children. Eur J Paediatr Dent. 2016 Jan 1;17(1):43-6. Pubmed PMID: 26949238.
- Rota E, Evangelista A, Ciccone G, Ferrero L, Ugolini A, Milani C, et al. Effectiveness of an educational and physical program in reducing accompanying symptoms in subjects with head and neck pain: a workplace controlled trial. J Headache Pain. 2011 Jun;12(3):339. 12(3):339-45. Pubmed PMID: 21249417.
- Mongini F, Evangelista A, Rota E, Ferrero L, Ugolini A, Milani C, Ceccarelli M, Joffrain L, Ciccone G, Galassi C. Further evidence of the positive effects of an educational and physical program on headache, neck and shoulder pain in a working community. J Headache Pain. 2010 Oct;11(5):409.Pubmed PMID: 20563879.
- Mongini F, Evangelista A, Rota E, Ferrero L, Ugolini A, Ceccarelli M, et al. Long-term benefits of an educational and physical program on headache, and neck and shoulder pain, in a working community. J Pain. 2009 Nov 1;10(11):1138-45.Pubmed PMID: 19398381.
- Geran RG, McNamara Jr JA, Baccetti T, Franchi L, Shapiro LM. A prospective long-term study on the effects of rapid maxillary expansion in the early mixed dentition. Am J Orthod Dentofacial Orthop. 2006 May 1;129(5):631-40. Pubmed PMID: 16679203.
- Adkins MD, Nanda RS, Currier GF. Arch perimeter changes on rapid palatal expansion. Am J Orthod Dentofacial Orthop. 1990 Mar 1;97(3):194-9. Pubmed PMID: 2178393.
- Gryson, JA. Changes in mandibular interdental distance concurrent with rapid maxillary expansion. Angle Orthod . 1977 Jul;47(3):186-92. Pubmed PMID: 332017.
- Hnat WP, Braun S, Chinhara A, Legan HL. The relationship of arch length to alterations in dental arch width. Am J Orthod Dentofacial Orthop.2000 Aug;118(2):184-8. Pubmed PMID: 10935959.
- Haas AJ. Gross reaction to the widening of the maxillary dental arch of the pig by splitting the midpalatal suture. Am J Orthod. 1959;45:868-9.
- Wertz R. and Dreskin, M. Midpalatal suture opening: A normative study. Am J Orthod. 1977 Apr;71(4):367-81. Pubmed PMID: 322499.
- Barrow GV, White JR. Developmental changes of the maxillary and mandibular dental arches. Angle Orthod. 1952 Jan;22(1):41-6.
- Lima AC, Lima AL, Filho RM, Oyen OJ. Spontaneous mandibular arch response after rapid palatal expansion: a long-term study on Class I malocclusion. Am J Orthod Dentofacial Orthop. 2004 Nov;126(5):576-82. Pubmed PMID: 15520690.
- Ugolini A, Doldo T, Ghislanzoni LT, Mapelli A, Giorgetti R, Sforza C. Rapid palatal expansion effects on mandibular transverse dimensions in unilateral posterior crossbite patients: a three-dimensional digital imaging study. Prog Orthod. 2016 Dec;17(1):1-7. Pubmed PMID: 26746202.
- McDougall PD, McNamara JA Jr, Dierkes JM. width development in Class II patients treated with Fränkel appliance. Am J Orthod. 1982 Jul;82(1):10- 22.Pubmed PMID: 6760718.
- Haas AJ. Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod. 1961 Apr;31(2):73-90.
- Ulrich DE, Oyen OD, Tsay TP, Grud SJ, Ayer WA. Mandibular width changes associated with maxillary expansion. Northwestern Dental Research. 1997;8:14-9.
- Sandstrom RA, Klapper L, Papaconstantinou S. Expansion of the lower arch concurrent with rapid maxillary expansion. Am J Orthod Dento facial Orthop. 1988 Oct 1;94(4):296-302.
- Moussa R, O'Reilly MT, Close JM. Long-term stability of rapid palatal expander treatment and edgewise mechanotherapy. Am J Orthod Dentofacial Orthop. 1995 Nov;108(5):478-88. Pubmed PMID: 7484967.
- Sinclair PM, Little RM. Maturation of untreated normal occlusions. Am J Orthod. 1983 Feb;83(2):114-23. Pubmed PMID: 6572039.
- Sillman JH. Dimensional changes of the dental arches: longitudinal study from birth to 25 years. Am J Orthod.1964 Nov 1;50(11):824-42.





