Clinical Behavior of Cl IV Direct Composite Restorations
Altukroni AA*, Alabduh MA, Khatiri MA
Ministry of Health, Saudi Arabia.
*Corresponding Author
Abdulbadea A Altukron,
Ministry of Health, Saudi Arabia.
Tel: 0034644422729
E-mail: dr-de3o@hotmail.com
Received: January 27, 2020; Accepted: March 16, 2020; Published: March 18, 2020
Citation:Altukroni AA, Alabduh MA, Khatiri MA. Clinical Behavior of Cl IV Direct Composite Restorations. Int J Dentistry Oral Sci. 2020;7(3):727-732.doi: dx.doi.org/10.19070/2377-8075-20000143
Copyright: Abdulbadea A Altukroni©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: The aim of this study, based on individual participant data from several studies, was to investigate the influence of materials related to Failure of class IV direct resin composite restorations and reason of failure. We conducted a search resulting in 5 longitudinal studies of class IV direct resin composite restorations with follow-up between two to twenty years. Main reasons for failure were luck of retention and fracture.
Materials and Methods: This is a review study. The research sources utilized were PubMed, Google scholar, MEDLINE and Complutense university Library. The keywords which were selected based on Medical Subject Heading (MeSH) terms and PICOS criteria were Class IV Direct Composite Restoration , Failure of Class IV Direct Composite Restoration, longevity of Class IV Direct Composite Restoration and survival rate of Class IV Direct Composite Restoration. For the period from 2010 to 2019. The number of subjects who restored with Nano filled resin composite (FiltekSupream) was 12, 13 subjects restored with Nano hybrid (Ceram X Duo), 13 subjects restored with polyacid modified resin composite (compomer), 7 subjects restored with resin-modified glass ionomer cement, 8 subjects restored with universal composites (Herculite XR), 16 subjects estored with universal composites (Charisma), 7 subjects restored with Highly Filled Hybrid Composite (TPH), 11 subjects restored with non specific resin composite and 2 subjects restored with microhybrid composite, Amaris (Voco).
Results: Nanofilled resin composite (FiltekSupream) and Nano hybrid (Ceram X Duo) both have the same longevity between two to five years in direct class IV composite, loss of restorations for lack of retention and fracture of restorations is the main reason of failure for both. Universal composites (Herculite XR) the most reason of failure in this type of composite is the anatomic form change, in the other hand, universal composites (Charisma) the esthetic reasons are the main reasons of failure. Both of them have long longevity until fifteen years. Polyacid-modified resin composite (compomer) and resin-modified glass ionomer cement have the same reason of failure that is restorations fracture in seven year more or less. Highly Filled Hybrid Composite (TPH) and microhybrid composite, Amaris (Voco) loss of restoration for lack of retention is the main reason of failure for both. However, they have short longevity between two to three years.
Conclusion: Three things decide the success rate, the survival rates and the longevity of direct class IV composite restorations, the dentist, the material and the patient. The study show failure reasons for different composite risen materials and the longevity. Fracture of restorations and loss of restorations for lack of retention are the most failure reasons. Patients must be educated about the expected life of these restorations as well as their advantages and disadvantages, so they can make an informed decision on a treatment option. There is lack of information about the longevity, survival rates, failure reasons of class IV direct composite in last 10 years. This study evaluate the reason of failure regarding to the studies that we showed.
2.Material and Methods
3.Discussion
4.Conflict of Interest
5.Conclusion
6.References
Introduction
The first tooth-colored composite was silicate cement, which was introduced in 1870s. This composite formulation was based on alumino-fluro-silicate glasses and phosphoric acid. However, were brittle, required mechanical retention, and had an average longevity of only a few years [1]. Then first polymeric tooth-colored composite used was based on polymethylmethacrylate, this material was developed in the 1940s, Although these materials were initially esthetic, they were plagued with a variety of problems, including poor color stability, high polymerization shrinkage, a lack of bonding to tooth structure, and a large coefficient of thermal expansion (CTE) [1]. Then the first polymer matrix composite incorporating silica fillers was introduced in the 1950s. These composites had improved mechanical properties and good esthetics; However, did not bond to tooth structure, and still exhibited significant polymerization shrinkage. In addition, there was no significant bonding between the silica particles and the polymer matrix. Consequently, these composites did not have good wear resistance clinically, because the filler particles were easily dislodged [1].
Composite classify according to their filler characteristics, such as chemical composition, shape, and especially particle size. Depend on the size of filler particles and their size distribution like microfills, hybrids, packables, and compomers. In addition, subclassifications, including flowables, and nano- and microhybrids [1]. Composites with smaller filler particles prevent the wear of the resin matrix and minimize the surface alteration deriving from the particles’ detachment [2]. Composite have been changed, in an attempt to achieve the best possible mechanical properties while maintaining esthetics. Changes in restorative treatment patterns improved restorative materials and techniques, effective preventive programs, enhanced dental care, and growing the longevity of dental restorations [3].
Restoration of anterior tooth fractures is a common dental procedure. Both direct and indirect options are clinically acceptable to repair fractured teeth. Anterior tooth fractures are usually result of sporting activities or accidents and tend to occur more often on the maxillary incisors [4].
In the 1970s, degradation or wear was considered the main reason for failure of composite restorations. Then Twenty years later, studies revealed secondary caries to be the new cause of failure [1].
The aim of this study, based on individual participant data from several studies, was to investigate the influence of materials related to Failure of class IV direct resin composite restorations and reason of failure. We conducted a search resulting in 5 longitudinal studies of class IV direct resin composite restorations with follow-up between two to twenty years. Main reasons for failure were luck of retention and fracture.
Material and Methods
Description of search strategy of relevant literature.
The objective of this study was to evaluate reasons of failure in direct composite class VI restorations.
Criteria for considering studies (PICO)
The studies considered for inclusion in this review include case series, cohort studies, and randomized clinical trial studies (Table 1).
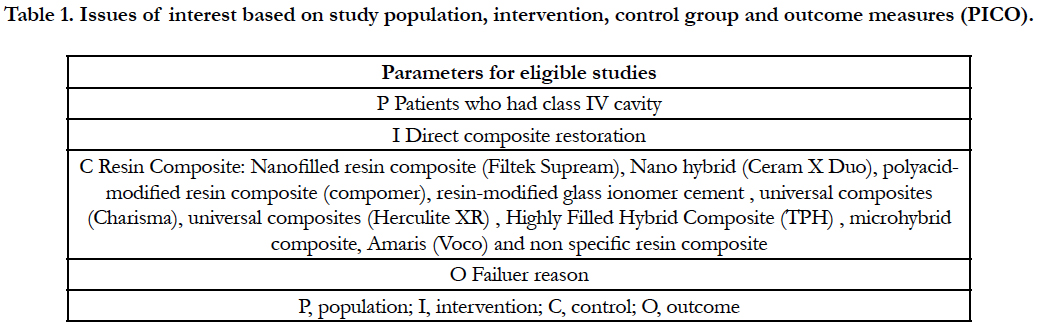

Table 1. Issues of interest based on study population, intervention, control group and outcome measures (PICO).
The PubMed (MEDLINE) database, Universidad de Complutense Library and Google scholar. The keywords were selected based on Medical Subject Heading (MeSH) terms and PICOS criteria. The keywords for search included: Class IV Direct Composite Restoration, Failure of Class IV Direct Composite Restoration, longevity of Class IV Direct Composite Restoration and survival rate of Class IV Direct Composite Restoration. To avoid any missing article, the references of each selected manuscript was rechecked manually through Mendeley Program.
A protocol was used for establishment of the inclusion and exclusion criteria. Full-text articles in English language were assessed for the following inclusion criteria including:
(1) Patients who had class IV cavities
(2) The technique was direct composite
(3) 3) Evaluate (C) in Direct clinical evaluation criteria (modified USPHS criteria)(Table 3) or (3) World Dental Federation (FDI) criteria (Table 4) as a failure
(4) The follow-up time was documented. Studies were excluded if they were animal or in vitro studies. Duplicate publications (risk of bias), articles without diagnosis information were removed from the study.
In an initial search, 47 articles were identified through electronic database. After removing duplications 28 articles were evaluated. Five articles were choose (Table 3). The total subject (Failed Class IV Direct Composite Restorations) number was 89 (Table 3). The medium follow up time was between two to twenty years. Restored with 8 different composite materials (Table 2).
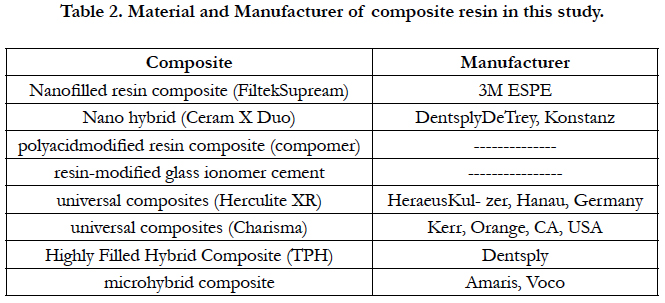
Table 2. Material and Manufacturer of composite resin in this study.
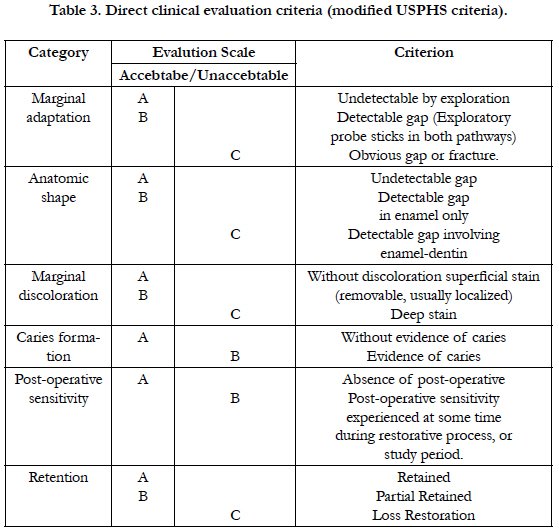
Table 3. Direct clinical evaluation criteria (modified USPHS criteria).
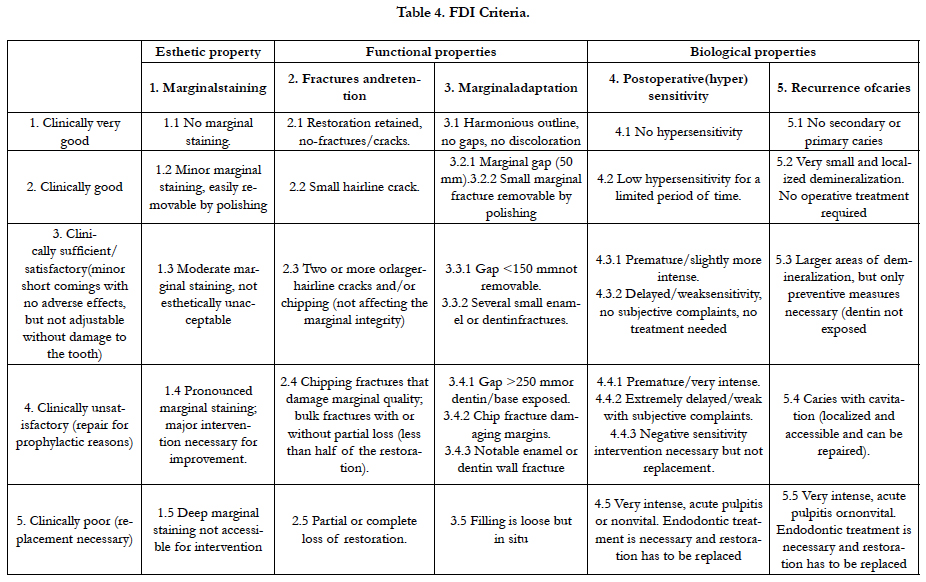
Table 4. FDI Criteria.
The number of subjects who restored with Nanofilled resin composite (FiltekSupream) was 12, 13 subjects restored with Nano hybrid (Ceram X Duo), 13 subjects restored with poly acid modified resin composite (compomer), 7 subjects restored with resin modified glass ionomer cement, 8 subjects restored with universal composites (Herculite XR), 16 subjects restored with universal composites (Charisma), 7 subjects restored with Highly Filled Hybrid Composite (TPH), 11 subjects restored with non specific resin composite and 2 subjects restored with microhybrid composite, Amaris (Voco).
In 12 subjects who restored with Nano filled resin composite (FiltekSupream), the failure reason in 9 subjects was lack of retention and in 3 subjects was restorations fracture in follow up time between 2 to 5 years. In 13 subjects who restored with Nano hybrid (Ceram X Duo), the failure reason in 10 subjects was lack of retention and in 3 subjects was restorations fracture in follow up time between 2 to 5 years. In 13 subjects who restored with polyacidmodified resin composite (compomer), the failure reason in all subjects was restorations fracture in follow up time 7 years and 6 months. In 7 subjects who restored with resin-modified glass ionomer cement, , the failure reason in all subjects was restorations fracture in follow up time 7 years. In 8 subjects who restored with universal composites (Herculite XR), the failure reason in 2 subjects was esthetic reason, in 2 subjects was restorations fracture, in 4 subjects was anatomic form change in follow up time between 10 to 20 years. In 16 subjects who restored with universal composites (Charisma), the failure reason in 9 subjects was esthetic reason, in 3 subjects was restorations fracture, in 2 subjects was marginal breakdown and in 2 subjects was anatomic form change in follow up time between 0 years to 20 years. In 7 subjects who restored with Highly Filled Hybrid Composite (TPH), the failure reason in 6 subjects was lack of retention and in 1 subject was restorations fracture, in follow up time 3 years. In 2 subjects who restored with microhybrid composite, Amaris (Voco), the failure reason in all subjects was lack of retention in follow up time 2 years. In 11 subjects who restored with non specific resin composite, the failure reason in all subjects was fracture restorations in follow up time 10 years.
Discussion
The longevity of composite restorations has been a topic of discussion for many years. There are Many variables affect longevity of composite restorations, including type of dentition, location and size of restoration, reasons for placement, type of material, adhesion, etc. The main reasons for replacement of anterior composite restorations are typically surface discoloration, secondary caries, and/or fracture of the restoration [5].
The reasons of failure can be loss of restoration for lack of retention, fracture of the restoration, esthetic reason (dis), restoration anatomical form change or restoration marginal breakdown Direct clinical evaluation criteria (modified USPHS criteria) (Table 4).
Class IV restorations had higher failure rates than Class III or V restorations. Longevity of large Class IV composite restorations placed in fractured anterior teeth has been shown to be relatively short. This is attributed to the relatively great amount of stress applied to these restorations during occlusal function [5].
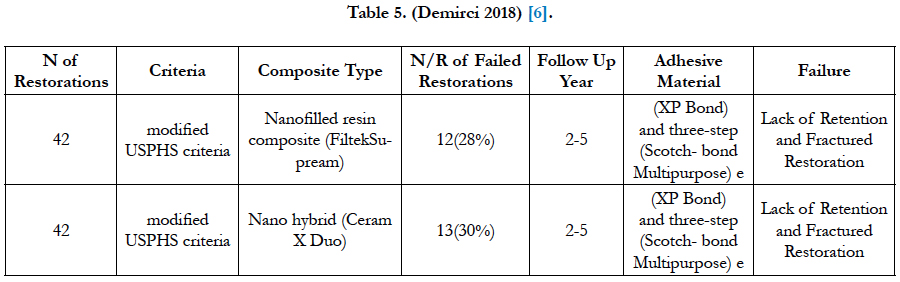
Table 5. (Demirci 2018) [6].
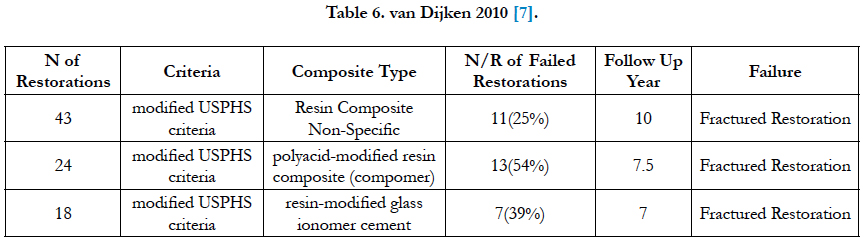
Table 6. van Dijken 2010 [7].
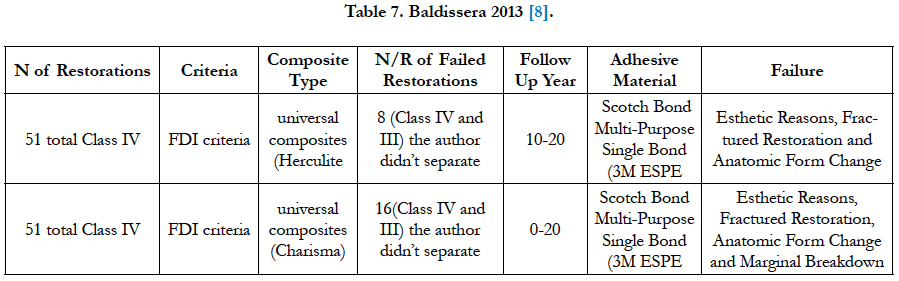
Table 7. Baldissera 2013 [8].
This study show reasons of failure of direct class IV composite restoration in some composite materials and the longevity of these materials. Hybrid composites as traditional hybrids, micro-, and nanohybrids. Contain of submicron inorganic filler particles (0.04 mm) and small particles (1 mm-4 mm), to improve the physical properties as well as acceptable levels of polishability. These improvements in wear resistance and fracture strength, along with good polishability, make hybrids the material of choice for Class III and Class IV restorations, 1, Nanofilled resin composite (FiltekSupream) and Nano hybrid (Ceram X Duo) both have the same longevity between two to five years in direct class IV composite, loss of restorations for lack of retentionand fracture of restorations is the main reason of failure for both.
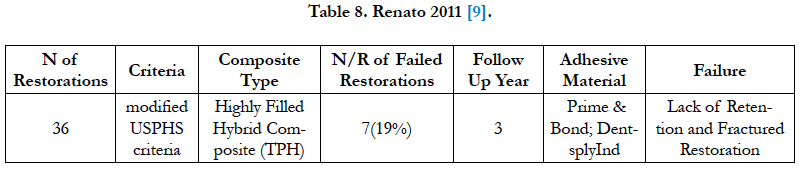
Table 8. Renato 2011 [9].
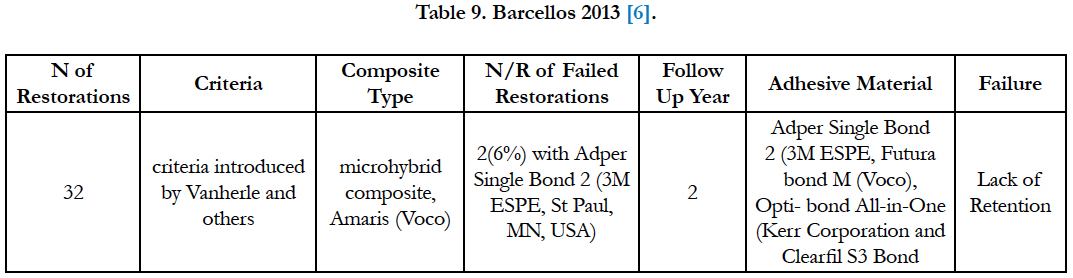
Table 9. Barcellos 2013 [6].
Universal composites (Herculite XR) the most reason of failure in this type of composite is the anatomic form change, in the other hand, universal composites (Charisma) the esthetic reasons are the main reasons of failure. Both of them have long longevity until fifteen years.
Polyacid modified resin composite (compomer) and resin-modified glass ionomer cement have the same reason of failure that is restorations fracture in seven year more or less.
Highly Filled Hybrid Composite (TPH) and microhybrid composite, Amaris (Voco) loss of restoration for lack of retention is the main reason of failure for both. However, they have short longevity between two to three years.
One of the factors that could greatly influence the longevity of direct composite resin restorations is the strength and long-term reliability of the adhesion to the tooth structure [10].
Regarding to the data that we collected in this study, of 89 failed direct class IV composite restoration, in follow up time between 2 to 20 years, by using 8 different types of composite. Fracture of the restorations is the most reason of failure with 43(48.3%) failed restorations, then loss of restorations for lack of retention with 27(30.3%) failed restorations, then then failure for esthetic reasons with 11(12.3%) failed restorations, then failure for change in the anatomical form of restorations with 6(6.7%) failed restorations and the less reason of failure is restoration marginal breakdown with 2(2.2%) failed restorations.
Conflict of Interest
The authors of this manuscript certify that they have no proprietary, financial, or other personal interest of any nature or kind in any product, service, and/or company that is presented in this article.
Conclusion
Three things decide the success rate, the survival rates and the longevity of direct class IV composite restorations, the dentist, the material andthe patient. The study show failure reasons for different composite risen materials and the longevity. Fracture of restorations and loss of restorations for lack of retention are the most failure reasons. Patients must be educated about the expected life of these restorations as well as their advantages and disadvantages, so they can make an informed decision on a treatment option. There is lack of information about the longevity, survivalrates, failure reasons of class IV direct composite in last 10 years. This study evaluate the reason of failure regarding to the studies that we showed.
References
- Puckett AD, Fitchie JG, Kirk PC, Gamblin J. Direct composite restorative materials. Dent Clin N Am. 2007 Jul 1;51(3):659-75.
- Angerame D, De Biasi M. Do nanofilled/nanohybrid composites allow for better clinical performance of direct restorations than traditional microhybrid composites? A systematic review. Oper dent. 2018 Jul;43(4):E191-209.
- Fahl Jr N. Step-by-step approaches for anterior direct restorative challenges. J Cosmet Dent. 2011;26(4):42-55.
- Romero MF, Austin JG, Todd M. Restoration of a large class IV fracture using direct composite resin: A clinical report. J Prosthet Dent. 2017 Oct 1;118(4):447-51.
- Experts G, Macedo G, Raj V, Ritter A V. Ask the Experts LONGEVITY OF ANTERIOR COMPOSITE RESTORATIONS. J Compil. 2006;18(6):310-311.
- Barcellos DC, Batista GR, Silva MA, Pleffken PR, Rangel PM, Fernandes Jr VV, Di Nicoló R, Torres CR. Two-year clinical performance of self-etching adhesive systems in composite restorations of anterior teeth. Oper Dent. 2013 Apr;38(3):258-66.
- van Dijken JW, Pallesen U. Fracture frequency and longevity of fractured resin composite, polyacid-modified resin composite, and resin-modified glass ionomer cement class IV restorations: an up to 14 years of follow-up. Clin oral invest. 2010 Apr 1;14(2):217-22.
- Baldissera RA, Corrêa MB, Schuch HS, Collares K, Nascimento GG, Jardim PS, Moraes RR, Opdam NJ, Demarco FF. Are there universal restorative composites for anterior and posterior teeth?. J Dent. 2013 Nov 1;41(11):1027-35.
- Moura FR, Romano AR, Lund RG, Piva E, Rodrigues Júnior SA, Demarco FF. Three-year clinical performance of composite restorations placed by undergraduate dental students. Braz Dental J. 2011;22(2):111-6.
- Batalocco G, Lee H, Ercoli C, Feng C, Malmstrom H. Fracture resistance of composite resin restorations and porcelain veneers in relation to residual tooth structure in fractured incisors. Dental Traumatol. 2012 Feb;28(1):75-80.





