Management of Children with Amelogenesis Imperfecta: Case Series
Elelmi Y1*, Chayma BA2*, Masmoudi F3, Baaziz A3, Maatouk F3, Ghedira H3
1 Assistant Professor, Pediatric Department, Faculty of Dental Medicine, Monastir, Tunisia.
2 Resident, Pediatric Department, Faculty of Dental Medicine, Monastir, Tunisia.
3 Professor, Pediatric Department, Faculty of Dental Medicine, Monastir, Tunisia.
*Corresponding Author
ELELMI Yamina,
Pediatric And Preventive Dentistry Department, Monastir Dental Faculty, Tunisia.
Tel: 00 216 52 933 588
E-mail: yamina_elelmi@yahoo.fr
BEN ARBIA Chayma,
Pediatric And Preventive Dentistry Department, Monastir Dental Faculty, Tunisia.
Tel: 00 216 55 159 339
E-mail: chaymaba12@gmail.com
Received: January 09, 2020; Accepted: February 07, 2020; Published: February 10, 2020
Citation:Elelmi Y, Chayma BA, Masmoudi F, Baaziz A, Maatouk F, Ghedira H. Management of Children with Amelogenesis Imperfecta: Case Series. Int J Dentistry Oral Sci. 2020;7(2):718-722. doi: dx.doi.org/10.19070/2377-8075-20000141
Copyright: Elelmi Y, Chayma BA©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Amelogenesis imperfecta (AI) is a heterogeneous inherited disorder that disturbs the developing enamel structure. This enamel anomaly affects both the primary and permanent dentitions.
The aim of this article was to describe through a series of cases, the therapeutic management of children with AI.
The purpose of the treatments were to eliminate tooth sensitivity while enhancing aesthetics and restoring masticatory function.
Treatment planning is related to the age of the patient, the type and severity of the disorder, and the oral health of the patient.
Early diagnosis, preventive care and timely treatment are important to improve oral health in children with AI.
2.Introduction
3.Case Presentation
3.1 Case Report 1
3.2 Case Report 2
3.3 Case Report 3
3.4 Case Report 4
4.Discussion
5.Conclusion
6.References
Keywords
Amelogenesis Imperfecta; Therapeutics; Mouth Rehabilitation; Nephrocalcinosis; Dental Enamel hypoplasia.
Introduction
Amelogenesis imperfecta (AI) is a group of hereditary conditions that primarily affect the quality and/or the quantity of dental enamel, with a variable occurrence of approximately 1/700-1/14,000.
In general, the inheritance pattern is usually autosomal dominant or recessive, or X linked [1-5, 7-11, 15].
Witkop’s classification is the most frequently cited one in the literature. Four major categories based primarily on phenotype (hypoplastic [HP], hypomaturation [HM], hypocalcified [HC], HM/HP with taurodontism) subdivided into 15 subtypes based on clinical phenotype and mode of inheritance [4].
AI has been associated with different dental anomalies including discolored teeth, microdontia, congenitally missing teeth, taurodontism, pulpal calcification, hypercementosis, crown and root resorption. In addition, AI was shown to be associated with malocclusions such as open bite and cross bite [5]. Apart from these difficulties, this condition also brought psychological problem and lack of self-confidence due to the appearance of their teeth. There are also other difficulties of managing AI including dental inexperience and anxiety of a child and parental expectation all of which further complicate its management.
Amelogenesis imperfecta affects deciduous dentition as well as a permanent dentition and requires a specific preventive and restorative care approach.
The aim of this article was to present the dagnostic elements of AI and the different therapeutic management.
A 13‑year‑old boy was referred to the department of Pediatric and Preventive Dentistry, Monastir Dental Faculty, Tunisia, with an aesthetic chief complaint. Apart from the consanguineous marriage, his parents had past dental and medical history that were noncontributory. There was no family history of AI and his elder male siblings showed normal dental development.
Intraoral examination revealed yellow to yellowish-brown teeth with rough surfaces, conspicuous and irregular defects, a lack of contact points and gingival hypertrophy. The enamel alterations were generalized affecting both lower and upper teeth (Figure 1.a.b.c).
The panoramic radiography showed deciduous teeth and incomplete permanent dentition with a delayed eruption and several impacted teeth.
No density difference was observed between enamel and dentin. The molars presented intrapulpal calcifications.(Figure 1.d).
A diagnosis of hypoplastic AI was made, transmission of the genes took place by autosomal recessive mode. The patient was further investigated. Ultrasound of kidney, ureter, bladder showed medullary nephrocalcinosis with bilateral multiple calculi. Based on the systemic investigation, patient has been diagnosed to have bilateral medullary calcinosis (Figure 1.e).
A treatment plan was developed which the main objective was to:
- reduce sensitivity
- improve esthetics
- restore masticatory function.
First, the patient was advised to brush with warm water and to use a normal fluoride toothpaste.
Second, a gingivectomy and gingivoplasty were performed to adjust the height of the cervical line.
Finally, stainless steel crowns were made on the permanent molars to slightly increase and maintain vertical dimension. Polycarbonate crowns were made on the permanent incisors, canines and premolars (Figure 1.f.g.h).
The patient was addressed to the nephrologist and the orthodontist.
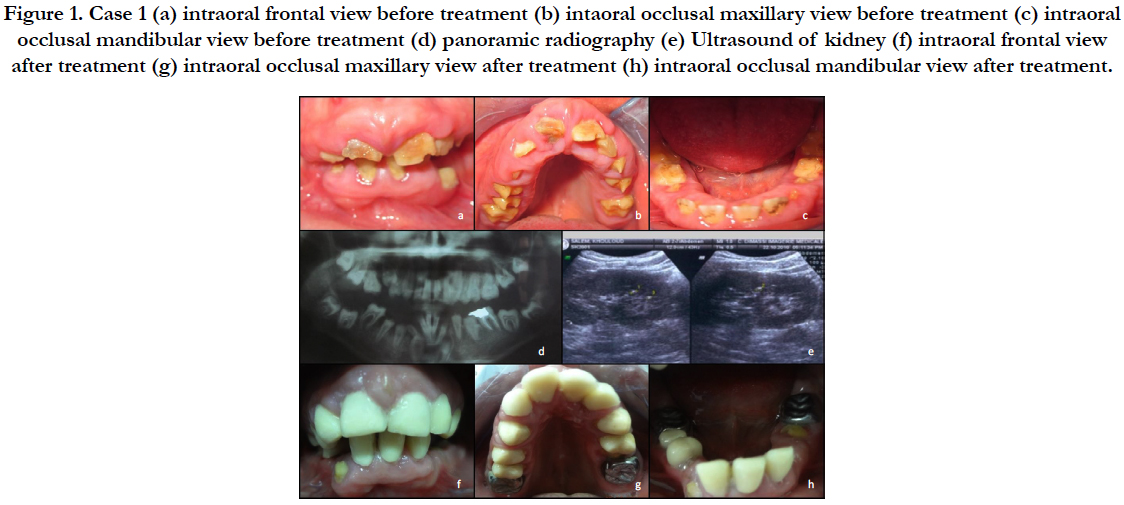

Figure 1. Case 1 (a) intraoral frontal view before treatment (b) intaoral occlusal maxillary view before treatment (c) intraoral occlusal mandibular view before treatment (d) panoramic radiography (e) Ultrasound of kidney (f) intraoral frontal view after treatment (g) intraoral occlusal maxillary view after treatment (h) intraoral occlusal mandibular view after treatment.
A girl aged 14 years old, referred to the department of Pediatric and Preventive Dentistry, Monastir Dental Faculty, Tunisia, regarding the unsightly teeth and dental hypersensitivity.
The patient came from a consanguineous marriage and her sister had the same dental anomaly. Her general, physical, and clinical findings were normal.
Intraoral examination showed generalized gingival inflammation, poor hygiene, anterior open bite deformity, yellow-brown rough fractured enamel of all the teeth and dilapidated maxillary permanent molar (16) ( Figure 2.a.b.c).
Radiographic examination revealed no density difference between enamel and dentin, inclusion of the following teeth ( 32; 43; 23) and persistence of the left primary maxillary canine (63) (Figure. 2.d).
The patient was diagnosed with AI (hypoplastic and hypomineralized type) via an X- linked-gene transmission mode.
Ultrasound of kidney, ureter, bladder were done and revealed no link between AI and nephrocalcinosis syndrome.
Treatment objectives taken into account were:
- Preservation of tooth integrity and vitality of permanent teeth
- Reducing sensivity and improve esthetics
- Normalization of oral functions
Treatment included oral prophylaxis, gingivectomy, and extraction of dilapidated permanent molar (16) and persistent primary canine (63).
Esthetic rehabilitation of decayed anterior teeth (incisors, canine and premolar) was done with polycarbonate crowns. Stain steel crowns was made on the permanent molars and removable partial denture for the extracted molar to obtain normal occlusion. (figure. 2.e.f.g)
The patient was referred to the orthodontic department to correct the anterior open bite.
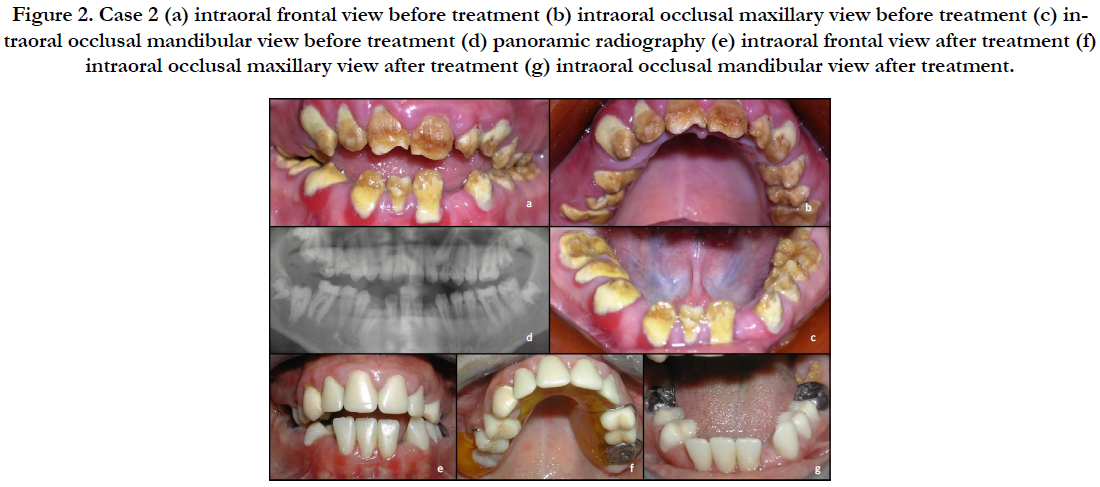

Figure 2. Case 2 (a) intraoral frontal view before treatment (b) intraoral occlusal maxillary view before treatment (c) intraoral occlusal mandibular view before treatment (d) panoramic radiography (e) intraoral frontal view after treatment (f) intraoral occlusal maxillary view after treatment (g) intraoral occlusal mandibular view after treatment.
An 11-year-old boy consulted the department of Pediatric and Preventive Dentistry, Monastir Dental Faculty, Tunisia, regarding the enhancing appearance of his teeth. He had a familial history of AI affecting her father, grandmother and several aunts and sister.
Oral examination revealed yellow-brown teeth with rough enamel, some enamel breaks in the anterior teeth generalized gingival inflammation, a lack of contact points and an anterior open bite ( Fig.3.a.b.c).
Panoramic radiography showed a reduction in the enamel thickness, a similar X-ray density between enamel and dentin, and the absence of the right second mandibular premolar: 45. (Figure 3.d)
A clinical diagnosis of hypoplastic AI was made and the mode of gene-transmission took place by X.
The patient was further investigated. Ultrasound of kidney, ureter, bladder were normal: The diagnosis of nephrocalcinosis was eliminated.
A treatment plan was developed with the following objectives:
- To improve the esthetics
- To reduce the reported sensitivity of the teeth
- To restore the masticatory function.
Restoration of anterior teeth with polycarbonate crowns and posterior teeth with stainless steel crowns was planned (Figure 3.e.f.g).
The patient was referred to the orthodontic department to correct the anterior open bite.
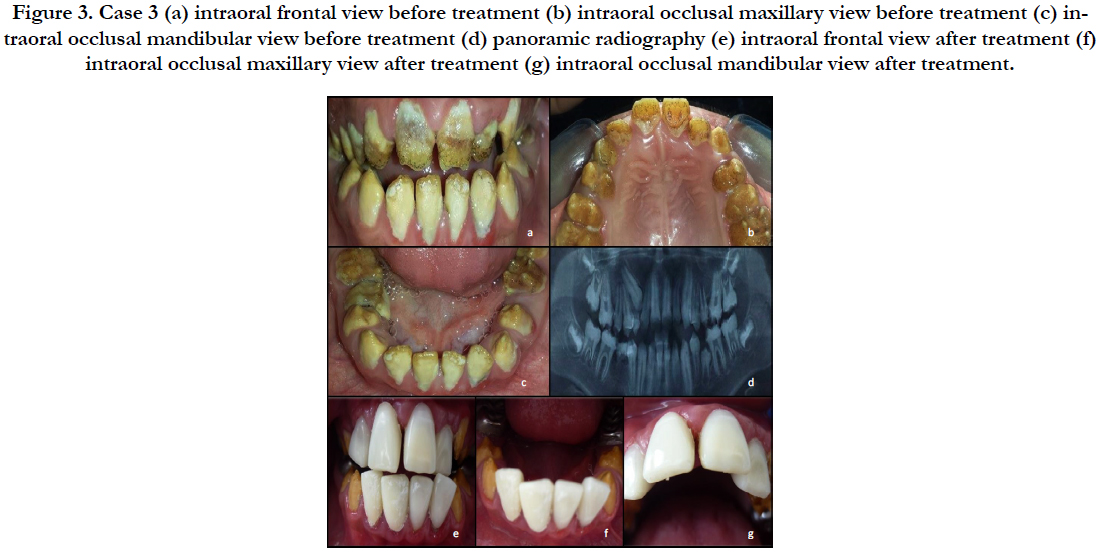

Figure 3. Case 3 (a) intraoral frontal view before treatment (b) intraoral occlusal maxillary view before treatment (c) intraoral occlusal mandibular view before treatment (d) panoramic radiography (e) intraoral frontal view after treatment (f) intraoral occlusal maxillary view after treatment (g) intraoral occlusal mandibular view after treatment.
A 9 years old girl referred to the department of Pediatric and Preventive Dentistry, Monastir Dental Faculty, Tunisia, with a complaint of esthetic inadequacy of his teeth and dental hypersensitivity. Her family history confirmed the consanguinity between her parents and showed normal dental development.
The patient general condition was good but she showed a very low self-esteem because of her poor appearance.
Intraoral examination revealed mixed dentition, yellow permanent teeth with rough surfaces, a lack of contact points and gingival hypertrophy. ( Figure 4.a.b.c).
On the panoramic radiography, no density difference was observed between enamel and dentin. (Figure 4.d).
A diagnosis of hypoplastic AI was made with an autosomal recessive gene-transmission mode.
Treatment was discussed according to several objectives:
- Functional restoration
- Aesthetic restoration
- Non-invasive rehabilitation that allowed evolution during growth
Treatment contained oral prophylaxis, gingivectomy, polycarbonate crowns on the incisors and canines to rehabilitate aesthetic of decayed anterior teeth and stain steel crowns on the molars to obtain normal occlusion. (Figure 4.e.f).
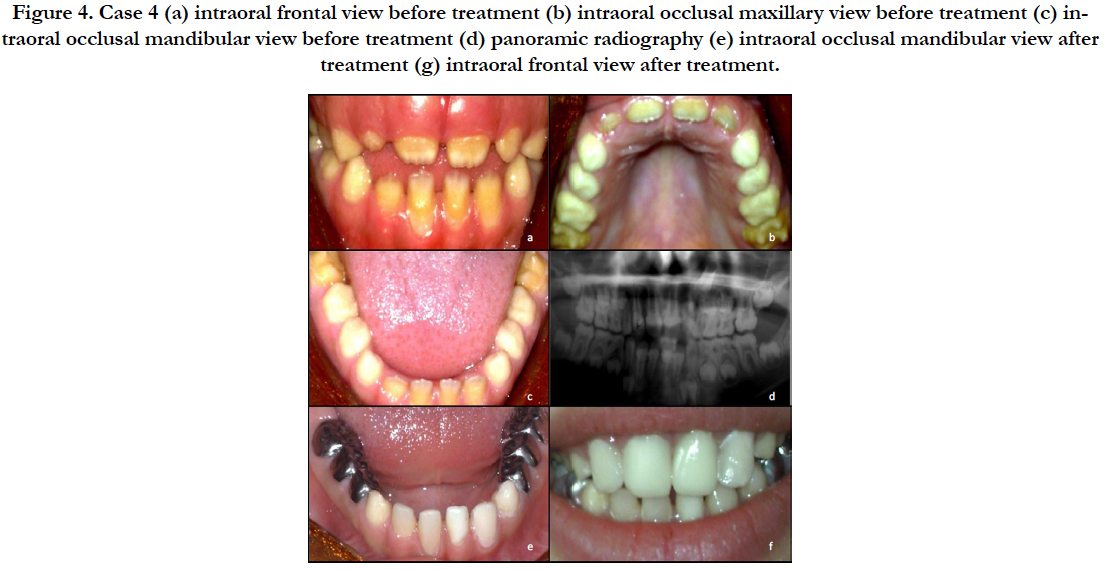

Figure 4. Case 4 (a) intraoral frontal view before treatment (b) intraoral occlusal maxillary view before treatment (c) intraoral occlusal mandibular view before treatment (d) panoramic radiography (e) intraoral occlusal mandibular view after treatment (g) intraoral frontal view after treatment.
Discussion
Amelogenesis imperfecta is a developmental disturbance that interferes with normal enamel formation [10].
Pediatric dentists are often the first to encounter children with AI and it is imperative that treatment requires an overall comprehensive plan that will also include a rough draft of future treatment needs [6].
Early identification of the disorder and preventive measures are crucial for children with AI [6].
Diagnosis is based on the family history, pedigree plotting, meticulous clinical and radiological observation. Dental radiographs of AI teeth provide important information to the clinician with respect to the degree of enamel mineralization to design an appropriate treatment plan [11, 12].
However, this could be challenging to achieve aesthetic improvement and functional rehabilitation in AI patients [1, 6].
Poor aesthetics, worn dentition, and interocclusal space problems (both insufficient space and open bite) complicate the treatment course of AI patients [6].
Oral hygiene can be particularly difficult for these patients due to the sensitivity while brushing. The use of warm water for tooth brushing will go some way towards relieving symptoms while rinsing. Also, regular use of fluoride mouthwashes can help to reduce sensitivity and prevent caries [3, 12].
The progression of treatment during childhood has been described as a temporary phase followed by a transitory phase.
In infancy, the primary dentition is protected by the use of preformed metal crowns on posterior teeth. Either polycarbonate crowns or composite restorations are used on anterior teeth [12, 13].
In the mixed dentition, stainless steel crowns, onlays for permanent molars, composite resin or glass ionomer cement for primary and permanent teeth [12, 13]. For permanent incisors, direct or indirect composite veneers will improve aesthetics, reduce sensitivity and reduce incisal wear. Good periodontal health and eruption process are important for long-term success of restorative treatments [12].
However, there is still no standard formula, current protocol or guideline for successful treatment. Initial treatment should be planned depending on AI type, severity and oral health habits of the patient [3, 13].
The success of bonding of composite resins to teeth affected by AI type is related to how the enamel responds to acid etching. High failure rates with adhesive restorations in patients with AI have been described, especially with HC AI. In this type of AI, the enamel has a higher protein content, which might reduce the bonding of restorations. Although deproteinization in HC AI has been reported to enhance the bonding of composite restorations, recent studies concluded that the procedure of deproteinization had no significant effect on the success of the adhesive restorations [14, 18].
In some of the previous case reports, it has been suggested that children with apparently autosomal recessive AI should, at least, have a renal ultrasound examination to exclude the association with nephrocalcinosis syndrome [15-17].
In fact, since nephrocalcinosis is often asymptomatic and can be associated with impaired renal function, pediatric-dentists who see children with a generalized and thin hypoplastic AI should consider a renal ultrasound scan and referral to a Nephrologist. Children with nephrocalcinosis should also be considered for a dental check [15-17].
Conclusion
AI is a disorder that should be diagnosed in an early stage to minimize the destructions of the teeth and to avoid its deleterious consequences.
The treatment plan should be based on patient’s age, type of defects and individual needs of the patients.
An interdisciplinary approach should be used to treat the patient starting at the first stage, not only due to functional and aesthetic reasons, but also for the positive psychological impact on young patient.
References
- Koruyucu M, Bayram M, Tuna EB, Gencay K, Seymen F.Clinical findings and long-term managements of patients with amelogenesis imperfecta. Eur J Dent. 2014 Oct;8(4):546-552.Pubmed PMID: 25512739.
- Ayers KMS, Drummond BK, Harding WJ, Salis SG, Liston PN. Amelogenesis imperfecta – multidisciplinary management from eruption to adulthood. Review and case report. N Z Dent J. 2004 Dec;100(4):101-4. Pubmed PMID: 15656432.
- Sabandal MMI, Schäfer E. Amelogenesis imperfecta: review of diagnostic findings and treatment concepts. Odontology. 2016 Sep;104(3):245-56. Pubmed PMID: 27550338
- Aldred M, Savarirayan R, Crawford P. Amelogenesis imperfecta: a classification and catalogue for the 21st century. Oral Dis. 2003 Jan;9(1):19-23. Pubmed PMID: 12617253.
- Leevailoj C, Lawanrattanakul S, Mahatumarat K. Amelogenesis Imperfecta: Case Study. Oper Dent. 2017 Sep/Oct;42(5):457-469. Pubmed PMID: 28829932.
- Markovic D, Petrovic B, Peric T. Case series: clinical findings and oral rehabilitation of patients with amelogenesis imperfecta. Eur Arch Paediatr Dent. 2010 Aug;11(4):201-8. Pubmed PMID: 20840832.
- Pathak A, Goenka P, Singhal R. Amelogenesis Imperfecta with Anterior Open Bite: A Rare Case Report. Int J Clin Pediatr Dent. 2011 Sep-Dec; 4(3): 245–247. Pubmed PMID: 27678235.
- Kamble VD, Parkhedkar RD. Multidisciplinary Approach for Restoring Function and Esthetics in a Patient with Amelogenesis Imperfecta: A Clinical Report. J Clin Diagn Res. 2013 Dec;7(12):3083-5. Pubmed PMID: 24551735.
- Akin H, Tasveren S, Yeler DY.Interdisciplinary Approach to Treating a Patient with Amelogenesis Imperfecta: A Clinical Report. J Esthet Restor Dent. 2007;19(3):131-5. Pubmed PMID: 17518900.
- American Academy of pediatric Dentistry. Guideline on dental management of heritabledental developmental anomalies. Pediatr Dent. 2013 Sep- Oct;35(5):E179-84. Pubmed PMID: 24290548.
- Reddy SS, Aarthi Nisha A, Harish BN. Hypoplastic amelogenesis imperfecta with multiple impacted teeth: report of two cases.. J Clin Exp Dent. e207:11.
- Crawford PJ, Aldred M, Bloch-Zupan A. Amelogenesis imperfecta. Orphanet J Rare Dis. 2007 Apr 4;2:17.Pubmed PMID: 17408482.
- Athanasiou A, Dimopoulou E, Vlasakidou A, Alachioti X. Amelogenesis imperfecta and anterior open bite: Etiological, classification, clinical and management interrelationships. J Orthod Sci. 2014 Jan;3(1):1-6. Pubmed PMID: 24987656.
- Neto NL, Paschoal MA, Kobayashi TY, Rios D, Silva SM. Early oral rehabilitation of a child with amelogenesis imperfecta. J Health Sci Inst. 2010;28(3):246-8.
- Vani SK, Varsha M, Sankar YU. Enamel renal syndrome: a rare case report. . J Indian Soc Pedod Prev Dent. 2012 Apr 1;30(2):169.
- Hunter L, Addy LD, Knox J, Drage N. Is amelogenesis imperfecta an indication for renal examination? . Int J Paediatr Dent. 2007 Jan;17(1):62-5. Pubmed PMID: 17181581.
- Patel A, Jagtap C, Bhat C, Shah R. Bilateral nephrocalcinosis and amelogenesis imperfecta: A case report. Contemp Clin Dent.6(2):262. Pubmed PMID: 26097369.
- Sönmez IS, Aras S, Tunç ES, Küçükeşmen C. Clinical succes of deproteinization in hypocalcified amelogenesis imperfecta. Quintessence Int. 2009 Feb;40(2):113-8. Pubmed PMID: 19169442.





