Evaluation of Root Canal Morphology of Lower Lateral Incisors using Cone Beam Computed Tomography in an Indian Subpopulation
Jerry Jose1, Ajitha P2*
1 Post Graduate Student, Department of Conservative Dentistry and Endodontics, Saveetha Dental College, Saveetha Institute of Medical and Technical
Sciences, Saveetha University, Chennai, India.
2 Professor, Department of Conservative Dentistry and Endodontics, Saveetha Dental College, Saveetha Institute of Medical and Technical Sciences,
Saveetha University, Chennai, India.
*Corresponding Author
Ajitha P,
Professor, Department of Conservative Dentistry and Endodontics, Saveetha Dental College, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai,
India.
Tel: +91 9444174551
E-mail: ajitharijesh@gmail.com
Received: Ocotber 08, 2020; Accepted: December 02, 2020; Published: December 10, 2020
Citation:Jerry Jose, Ajitha P. Evaluation of Root Canal Morphology of Lower Lateral Incisors using Cone Beam Computed Tomography in an Indian Subpopulation. Int J Dentistry Oral Sci. 2020;7(12):1193-1196. doi: dx.doi.org/10.19070/2377-8075-20000236
Copyright: Ajitha P©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim: To aim of the current study was to evaluate the root canal morphology of lower lateral incisors in an Indian subpopulation
using Cone-Beam computed tomography
Material and Methods: The CBCT images of 256 patients were obtained from the Department of Oral Medicine and Radiology
of the University. Various parameters such as number of roots, number of root canal and canal configuration were evaluated and
recorded and then classified according to Vertucci’s classification of root canals.
Results: The most common root canal morphology is for Vertucci’s Type 1 which is 40.2%, and Type 2 being 33.6%. The other
types being Type 3(11.4%), Type 4(6.3%), Type 5(1.9%), Type 7(4.7%) and Type 8(1.9%).
Conclusion: From the assessed data it was seen the root canal morphology of lower lateral incisors exhibited a higher incidence
of Vertucci’s Type 1 and Type 2 andother configurations being Type 3, Type 4, Type 7, Type 5, Type 8. Type 6 was not to be seen
in the assessed sample. The variation in the root canal morphology was seen most commonly in the male population than in female
population.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.Refereces
Keywords
Lower Lateral Incisors; Root Canal Morphology; Cone Beam Computed Tomography; Vertucci’s Classification.
Introduction
Endodontic treatment is a complex process which requires the
practitioners to study the root canal morphology in tremendous
detail. Accurate diagnosis of the root canal morphology is of very
high significance since it can lead to a successful endodontic treatment
[1]. Root canal therapy involves shaping and cleaning of
root canal systemfollowed by filling with an inert restorative material.
Presence of untreated canal is said to be a major cause of
endodontic failure [2]. Different radiographic methods are used
for endodontic diagnosis of root canal morphology such as tooth
staining and colouring, conventional radiographs, digital medium
advanced radiographic techniques and the more recent computed
tomography techniques [3].
Cone beam computed tomography or CBCT is amethod introducedfor
diagnostic application in endodontic clinical practice. It
is used for different applications such as assessment of endodontic
trauma, diagnosis of radiographic signs of periapical lesions,
confirmation of nonodontogenic causes of pathosis, assessment
of complex root canal systems prior to endodontic management,
assessment of endodontic treatment complications or for management
of root resorption [4]. CBCT is said to be used initially
for angiography to assess the blood patterns and has paved its way
into various medical applications in different fields. Its mechanism
is said to be acquire individual image slices which are reconstructed
and made into a single image. CBCT is said to obtain a single
field of view (FOV) in an arc manner of planar image projection
[5]. The smaller the FOV the less the radiation exposure seen to
the patient. Another advantage of CBCT over conventional CT
is the decreased scan time ranging from 10-40 secs and in current advanced systems ranging from 5- 8 seconds [6].
Various retrospective studies [7-9] have been done which aims at
evaluating the different root canal morphology in different subpopulation
but none of the studies have been done to evaluate the
root canal variations of lower lateral incisors using Cone-beam
computed tomography in an Indian subpopulation. The current
study aims to evaluate the root canal morphology of lower lateral
incisors in an Indian subpopulation (Chennai) using cone beam
computed tomography data.
Materials and Methods
The CBCT images were obtainedfrom Dentsply Sirona 3D unit
(Orthophos XG 3D) with operating parameters(3-6 mA and 60-
90 kV, Exposure time - 5.1 seconds).The smallest possiblefield of
view (FOV) was used (8 × 8 cm) and isotropic voxel size was 0.16
mm.The effective dose was between 14 μsv-166 μsv. All CBCT
scans were performed with the minimum exposure necessary
for adequate image quality. The as low as reasonably achievable
(ALARA) protocol was strictlyfollowed. The patient was made to
position parallelto the emitter beam withhorizontal axis towards
the alveolar process, and the teethunder examination were placed
in thecentreof the volume.Vertucci’s classification (1-8) was used
as mode of classification to determine the number of canals [10].
A total CBCT data from the time frame April 2019 to September
2019 consisting of 256 patients were collected from the Department
of Radiology, out of the 256 patients CBCT data assessed
41 patients CBCT data was excluded. The acquisition process
was performed by an experienced radiologist. The data was taken
based on the inclusion/exclusion criteria:
• Permanent mandibular lateral incisors which were fully developed
• Absence of root canal treatment
• Absence of post and core restorations
• Absence of large metallic restorations which may interfere image analysis
• Absence of root resorption or periapical lesions
• No previous root amputation or hemi section
• Presence of high-quality CBCT images in which canal orifice and root canal configuration could be recognized.
• Distorted CBCT images
• Edentulous ridges
• Patients below the age of 18 years and above the age of 60 years
• Missing lower anterior
• Patients undergoing orthodontic treatment.
The data was collected interpreted digitally using Galaxis Galileo’s
Viewer 1.9 (Sirona Dental Systems, SICAT GmbH & Co. KG,
USA). The following information was recorded:
• The number of roots
• The root canal configuration the results were acquired, analysed and interpreted according to Vertucci’s Classification.
An experienced endodontist was made to assess the CBCT images
independently and could scroll through axial, coronal and
sagittal views of each tooth. In case of disagreement, the case
was made to discuss with another fellow endodontist until a consensus
was reached.
The statistical analysis was done using SPSS 21.0 (IBM Corp, Armonk,
USA). Descriptive Analysis was conducted following by
which a chi square analysis was conducted on the acquired data
among the same patient. A p value less than 0.05 was considered
to be statistically significant.
Results
From the analysed 214 samples, 125 samples belonged to the male
population and 90 samples belonged to the female population.
All the analysed images showed a single root configuration. The
incidence of canal variation was seen to be around 60% from the
total assessed samples. Table 1 denotes the frequency of canal
variation from the assessed samples. Vertucci’s Type 1 was seen to 35.5% in tooth 32 and 44.9% in tooth 42, Vertucci’s Type 2
was seen to be second highest in 32(40.7%) and 42(26.6%). A
total variation canal variation was seen of 33.6%. Vertucci’s Type
3 was seen to be the next most commonly seen with 32(8.9%) and
42(14.0%). Vertucci’s Type 4 was seen to be 6.3%, Vertucci’s Type
5 was seen to be 1.9%, Vertucci’s Type 7 was seen to 4.7% and
Vertucci’s Type 8 was seen to 1.9% respectively. A Chi-square test
between the analysed samples showed a significant correlation between
the assessed samples (p<0.05).
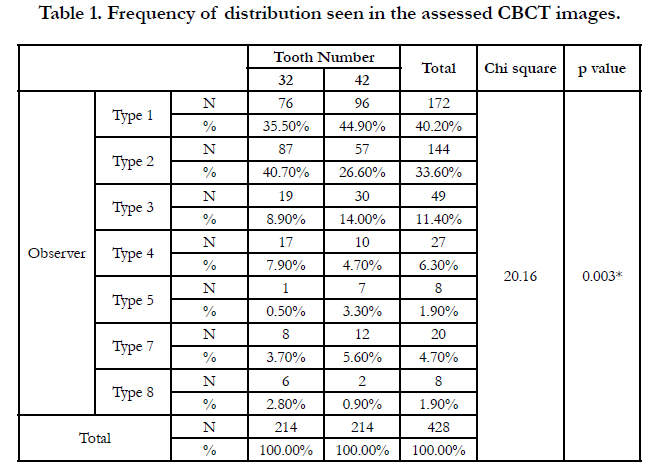

Table 1. Frequency of distribution seen in the assessed CBCT images.
Discussion
The current study aims to assess the diverse root canal morphology
in an Indian subpopulation. Mandibular lateral incisors are
one of the most common teeth present in the oral cavity shown
to have a high degree of root canal morphology variations and
has proven to clinically challenging for various practitioners. The
incidence of second canal is seen more than 40% with more than
1% having a separate foramen [5]. Numerous studies have shown
the presence of varied root canal morphology for lower anterior
[11, 12]. It is seen that root canal morphology variation is seen
among different racial population as well with the results varying
among different population. This could possibly be due to genetic
diversity playing a role in the variation of the canals. CBCT is an
effective tool which can be used for the endodontic practice for
locating additional canals or varied tooth morphology. Different
scenarios are seen in which the mandibular lateral incisor exhibit
varied root canal morphology. CBCT imaging is a non-invasive
technique that was reported to be as accurate as the modified canal
staining and clearing technique for evaluating root canal systems
[13]. Root canal variation is one of the factors seen with
studies showing the incidence of anatomical variation being more
common in males than in females [14]. The current study also
corelates with the existing literature of the canal variation being
more diverse in male population than in female population.
Several studies have used other different methods for the examination
of root canal morphology which are use of polyester resins,
creating transparent angles and use of 2D radiographs [15]. In
clinical practice the use of roentogram is said to have severe limitations
due to fact that it is 2-dimensional in nature which limits
the clinician’s ability to detect any additional canals. Currently with
the introduction of CBCT the clinician can visualize the tooth
in a 3-dimensional view which helps them to acquire the image.
In contrast to traditional radiography, CBCT scanning provides
3-dimensional images in axial, sagittal, and coronal sections that
could avoid geometric distortion and anatomic super imposition.
However, the cost of CBCT scanning compared with periapical
radiography hinder its clinical application in developing countries.
A case report published by Reeh et al, has seen the incidence of
fusion of the mandibular lateral incisor and seen varied apices
with some being more than one [16]. One of the main failures of
endodontic treatment is the missed root canal system this is seen
due to the anatomical variation in the root canal system [17]. A
study done by Boruah et al., [18] in which the incidence of type
1 root canal morphology is 63.5%, another study done by Wu et
al., [19] for the Taiwanese population had seen similar results with
Vertucci’s type 1 being 75% and type 3 being 23%. The present
study shows a slight variation in the results obtained in which
Vertucci’s Type 1 (40.2%), Type 2 (33.6%), Type 3(11.4%), Type
4(6.3%), Type 5(1.9%), Type 7(4.7%) and Type 8(1.9%). The incidence of a type 6 canal configuration was seen to nil from the
assessed samples.
Previously, various methods were advocated for the examination
of root canal morphology. The most primitive method used were
to sectionthe tooth, this was discontinued due to fact that it does
not allow a continuous view of the root canal system and also irreversibly
changing the morphology [20]. Another method given
by Robertson et al.which was used for a short amount of time
is the clearing technique in which India ink was used as for the
identification of the root canal system [21]. Ground sectioning
of the apices has also been done by various authors to study the
root canal morphology. In the recent timesscanning electron microscopy
or SEM is another method used to for the study of root
canal morphology but clinically impossible have not been able
to use [22]. With the advent of cone beam computed tomography,
the clinician can evaluate and plan the data with considerable
detail the mechanism of CBCT being a fan shaped beam which
is exposed to the target structure which is simulated to multiple
exposure in a single field of view and involving the sectioning of
the tooth in three planar directionthat is axial, coronal and sagittal
direction [23]. The mechanism of CBCT radiographs is very
much similar to conventional OPG but unlike the conventional
orthopanthograph which is taken in a 2-dimensional image CBCT
acquires the image in 3-dimensional in which a gantry is used to
acquire slices of images which are compiled together digitally to
produce a single image. Hundreds of planar projection images
are acquired in the field of view which ranges at 180 degree [24].
Multiple studies are performed among different ethnic population
to determine the root canal morphology. In Iranian population it
was seen that the population has Type 1 having 70.6% for permanent
lateral incisors compared to other types [13]. A study done
by Altunsoy et al., for the Turkish population had seen that Type
5 was one of the frequently observed root canal configurations
[25]. In the Chinese population a study conducted by Liu et al.,
had seen that males had 14.6% and females had 11.9% incidence
of second canal [26]. Micro CT is another method which can be
used for evaluation of the root canal morphology which is able to
provide much accurate information about root canal morphology
than the CBCT but its indicative purpose in clinical practice is not
applicable, but they can only be used on extracted teeth. In clinical
situations conventional radiography is the most commonly used
method to distinguish tooth anatomy.
One of the limitations of the present study, is to not use an advanced
diagnostic method such as micro CT for the evaluation of
root canal morphology. Though micro CT is shown to be much
effective in analysing root canal morphology the excessive cost
for analysis and its clinical application is seen to negligible the
usage of CBCT is still preferred for cone beam computed tomography
analysis.
Conclusion
Within the limitations of the present study, it can be concluded
that most of the tooth examined had Type 1 root canal morphology
of mandibular incisors. In tooth exhibiting more than single
canal, the Type II canal configuration was the most prevalent followed
by Type III, Type IV configuration based on the Vertucci’s
Classification. The least exhibited root canal morphology being additional type 6. Gender variation as also seen in a factor for the
variation in root canal morphology with the incidence of second
canal being more common in males than in female population.
References
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endodontic topics. 2005 Mar;10(1):3-29.
- Verma P, Love RM. A Micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int Endod J. 2011 Mar; 44(3):210-7. PMID: 20880136.
- Neelakantan P, Subbarao C, Subbarao CV. Comparative Evaluation of Modified Canal Staining and Clearing Technique, Cone-Beam Computed Tomography, Peripheral Quantitative Computed Tomography, Spiral Computed Tomography, and Plain and Contrast Medium–enhanced Digital Radiography in Studying Root Canal Morphology. Journal of Endodontics. 2010 Sep; 36(9): 1547–51. Pubmed PMID: 20728725.
- Patel S, Durack C, Abella F, Roig M, Shemesh H, Lambrechts P, et al. European Society of Endodontology position statement: The use of CBCT in Endodontics. International Endodontic Journal. 2014 Jun; 47(6): 502–4. Pubmed PMID: 24815882.
- Scarfe WC, Farman AG. What is Cone-Beam CT and How Does it Work? Dental Clinics of North America. 2008 Oct;52(4):707–30. Pubmed PMID: 18805225.
- Patel S. New dimensions in endodontic imaging: Part 2. Cone beam computed tomography. International Endodontic Journal. 2009 Jun; 42(6): 463–75. Pubmed PMID: 19298576.
- Lin Z, Hu Q, Wang T, Ge J, Liu S, Zhu M, et al. Use of CBCT to investigate the root canal morphology of mandibular incisors. Surg Radiol Anat. 2014 Nov;36(9):877–82. Pubmed PMID: 24515289.
- Han T, Ma Y, Yang L, Chen X, Zhang X, Wang Y. A Study of the Root Canal Morphology of Mandibular Anterior Teeth Using Cone-beam Computed Tomography in a Chinese Subpopulation. Journal of Endodontics. 2014 Sep;40(9):1309–14. Pubmed PMID: 25043332.
- Saati S, Shokri A, Foroozandeh M, Poorolajal J, Mosleh N, Saati S, et al. Root Morphology and Number of Canals in Mandibular Central and Lateral Incisors Using Cone Beam Computed Tomography. Brazilian Dental Journal. 2018 May;29(3):239–44. Pubmed PMID: 29972448.
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surgery, Oral Medicine, Oral Pathology. 1984 Nov;58(5):589–99. Pubmed PMID: 6595621.
- Kabak YS, Abbott PV. Endodontic treatment of mandibular incisors with two root canals: Report of two cases. Australian Endodontic Journal. 2007 Apr;33(1):27–31. Pubmed PMID: 17461838.
- Sert S, Aslanalp V, Tanalp J. Investigation of the root canal configurations of mandibular permanent teeth in the Turkish population. International Endodontic Journal. 2004 Jul;37(7):494–9. Pubmed PMID: 15189440.
- Aminsobhani M, Sadegh M, Meraji N, Razmi H, Kharazifard MJ. Evaluation of the Root and Canal Morphology of Mandibular Permanent Anterior Teeth in an Iranian Population by Cone-Beam Computed Tomography. J Dent (Tehran). 2013 Jul;10(4):358–66. Pubmed PMID: 24396355.
- Mauger MJ, Schindler WG, Walker WA. An evaluation of canal morphology at different levels of root resection in mandibular incisors. Journal of Endodontics. 1998 Sep;24(9):607–9. Pubmed PMID: 9922750.
- Kazemipoor M, Hajighasemi A, Hakimian R. Gender difference and root canal morphology in mandibular premolars: A cone-beam computed tomography study in an Iranian population. Contemp Clin Dent. 2015;6(3):401–4. Pubmed PMID: 26321843.
- Reeh ES, ElDeeb M. Root canal morphology of fused mandibular canine and lateral incisor. Journal of Endodontics. 1989 Jan;15(1):33–5. Pubmed PMID: 2607265.
- . Ghamari M, Farhad Mollashahi N, Salarpour M, Mousavi E, Kazemian K, Moudi E, et al. Evaluation of the relationship between crown size and root canal morphology of mandibular incisors by cone beam computed tomography (CBCT). Electron Physician. 2017 Aug 25; 9(8): 5001–7. Pubmed PMID: 28979734.
- Boruah LC, Bhuyan AC. Morphologic characteristics of root canal of mandibular incisors in North-East Indian population: An in vitro study. J Conserv Dent. 2011;14(4):346–50. Pubmed PMID: 22144800.
- Wu Y-C, Cheng W-C, Chung M-P, Su C-C, Weng P-W, Cathy Tsai Y-W, et al. Complicated Root Canal Morphology of Mandibular Lateral Incisors Is Associated with the Presence of Distolingual Root in Mandibular First Molars: A Cone-beam Computed Tomographic Study in a Taiwanese Population. Journal of Endodontics. 2018 Jan;44(1):73-79.e1. Pubmed PMID: 29079050.
- Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surgery, Oral Medicine, Oral Pathology. 1971 Aug;32(2):271– 5. Pubmed PMID: 5284110.
- Robertson D, Leeb IJ, McKee M, Brewer E. A clearing technique for the study of root canal systems. Journal of Endodontics. 1980 Jan;6(1):421–4. Pubmed PMID: 7005366.
- Hegde RS, Miller DA. Scanning Electron Microscopy for Studying Root Morphology and Anatomy in Alfalfa Autotoxicity. Agron.j. 1992 Jul;84(4):618–21.
- Mao T, Neelakantan P. Three-dimensional imaging modalities in endodontics. Imaging Sci Dent. 2014 Sep;44(3):177–83. Pubmed PMID: 25279337.
- Scarfe WC, Levin MD, Gane D, Farman AG. Use of cone beam computed tomography in endodontics. Int J Dent. 2009; 2009: 634567. PMID: 20379362.
- Altunsoy M, Ok E, Nur BG, Aglarci OS, Gungor E, Colak M. A cone-beam computed tomography study of the root canal morphology of anterior teeth in a Turkish population. Eur J Dent. 2014;8(3):302–6. Pubmed PMID: 25202207.
- Liu J, Luo J, Dou L, Yang D. CBCT study of root and canal morphology of permanent mandibular incisors in a Chinese population. Acta Odontologica Scandinavica. 2014 Jan 1;72(1):26–30. Pubmed PMID: 24255962.





