Comparison of Infrazygomatic Crest Mini-Implant and Inter-Radicular Mini-Implant as Skeletal Anchorage when used for En Masse Anterior Retraction and En Masse Distalization - A Fem Study
Swapna Sreenivasagan1, Aravind Kumar Subramanian2*, Jong-Moon Chae3, Stephen Mark Chadwick4
1 Resident, Department of Orthodontics, Saveetha Dental College, Saveetha Institute of Medical and Technical Science, Saveetha University, Chennai,
India.
2 Professor and Head of the Department, Department of Orthodontics, Saveetha Dental College, Saveetha Institute of Medical and Technical Science,
Saveetha University, Chennai, India.
3 Professor, Department of Orthodontics, School of Dentistry, University of Wonkwang, Wonkwang Dental Research Institute, Iksan, Korea; Visiting
Scholar, Postgraduate Orthodontic Program, Arizona School of Dentistry and Oral Health, A.T. Still University, Mesa, Ariz.
4 Professor and Consultant orthodontist, NHS Royal College of Physicians and Surgeons of Glasgow,London , United Kingdom.
*Corresponding Author
Dr. Aravind Kumar Subramanian,
Professor and Head of the Department, Department of Orthodontics, Saveetha Dental College, Saveetha Institute of Medical and Technical Science, Saveetha University, Chennai,
India.
Tel: 9841299939
E-mail: aravindkumar@saveetha.com
Received: November 01, 2020; Accepted: December 03, 2020; Published: December 04, 2020
Citation:Swapna Sreenivasagan, Aravind Kumar Subramanian, Jong-Moon Chae, Stephen Mark Chadwick. Comparison of Infrazygomatic Crest Mini-Implant and Inter-Radicular Mini-Implant as Skeletal Anchorage when used for En Masse Anterior Retraction and En Masse Distalization - A Fem Study. Int J Dentistry Oral Sci. 2020;7(12):1176-1181. doi: dx.doi.org/10.19070/2377-8075-20000233
Copyright: Aravind Kumar Subramanian©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: This paper describes a finite element model study comparing infrazygomatic crest mini-implants with inter-radicular
mini-implants for both En Masse retraction of anterior teeth and En masse distalization of the upper dentition.
Aim: The main objectives of this study were to examine the forces on the bone generated by the alternative biomechanic systems
of anterior retraction or en masse distalization.
Design: Finite element analysis.
Setting: Department of orthodontics.
Material and Methods: Finite element models of maxillary anterior teeth and surrounding bone were constructed from CT scans
Main outcome methods: FEM model was used to simulate the force levels and direction using the two alternative mini-implant
systems under investigation.
Results: There was no significant difference between the force levels used in infrazygomatic crest mini-implants compared to
inter-radicular mini-implants. Maximum distalization was achieved when the infrazygomatic crest mini-implants were placed at 70
degrees. The infrazygomatic crest mini-implants were more effective in en masse distalization of the maxillary dentition. If both
intrusion and retraction are indicated infrazygomatic mini-implants are a better choice than inter-radicular mini-implants.
Conclusions: The infrazygomatic crest mini-implants were more effective in en masse distalization of the maxillary dentition.
If both intrusion and retraction are indicated infrazygomatic mini-implants are a better choice than inter-radicular mini-implants.
2.Introduction
3.Methodology
4.Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.Refereces
Keywords
Finite Element Analysis; Intrusion; Retraction; Infrazygomatic Crest Mini-Implant; Inter-Radicular Mini-Implant.
Introduction
Anchorage has been described as the resistance to unwanted
tooth movement. As many of our patients present with proclined
upper anterior teeth and an increased overjet it is desirable for
these teeth to be retroclined and retracted. The reaction to this
desirable tooth movement is the undesirable mesial movement
of the upper posterior molars. As a consequence anchorage has
often involved headgear, palatal arches or temporary anchorage
devices in maxilla in order to resist this undesirable mesial movement
of the upper molar teeth. Our paper goes further than preventing
the upper molar teeth moving mesially as a reaction to
the retraction of the upper incisors and looks at the En Masse
distalization of the whole of the maxillary dentition. This is a new
development for our speciality as this type of En Masse movement
of the whole dentition was previously only possible using
orthognathic surgery.
Stable molar anchorage is a pre-requisite for orthodontic treatment
with fixed appliances [1]. Skeletal anchorage with mini-implants
has been reported as an adjunct to orthodontic treatment
that is less dependent on patient compliance [2]. In split mouth
studies comparing conventional anchorage and mini-implants retraction
can be achieved with no loss of anchorage on the implant
side whilst on on the non implant side there will be a small loss
of anchorage [3]. Mini-implants can be an efficient alternative to
the conventional molar anchorage especially in maximum anchorage
situations [1]. Not only have these screws proved to be useful
for anchorage in extraction cases, they have also been used cases
where it is desirable to distallize the entire arch [4].
The finite element method is a widely used mathematical model
for solving problems in engineering. It has been used in structural
analysis, heat transfer, mass transport and electromagnetic potential.
Finite element analysis is a way of mathematically modelling
the stresses on an engineering design. Finite element analysis has
found increasing use in the field of orthodontics due to its ability
to deliver detailed yet precise information regarding stress on
load application [5]. Finite element method (FEM) studies can
be useful for us to understand the various factors that we can’t
clinically assess.
The variability of material characteristics, the loads applied to the
orthodontic appliance and the dentition, the stress patterns and
their geometric evaluation [6]. Using the finite element method
complex structures like the maxilla are divided into smaller units
called finite elements which helps in formulating a solution for
each element rather than for the whole arch [7]. Computational
techniques have helped our understanding of biomechanics.
Finite element method has been helpful in orthodontics as it is
impractical to use randomized clinical trials to compare every
modification to biomechanics or to appliance design. Finite element
method have been used to simulate the addition of miniimplants,
the addition of power arms to brackets, the intrusion
and extrusion of teeth and variations in the arch wire dimensions
[7-10].
Infrazygomatic crest mini-implants are usually made of either
stainless steel or titanium and placed in the region of infrazygomatic
crest distal to the first permanentmolar. They are used
mostly in en masse distalization and in orthodontic correction
of malocclusions without surgery or extractions [11]. The distal
movement of anterior teeth in conventional mechanics is usually
inefficient and slow. Where as mini-screws offers the practitioner
the opportunity to translate the entire anterior quadrant. Thereby
reducing the treatment time, eliminating any loss of anchorage
and also reducing patient discomfort [12] Miniscrews have been
used in non-extraction cases and maintained throughout treatment
in order to provide anchorage for the retraction of the
whole dentition [13].
The main objective of this paper is to evaluate the en masse retraction
of the anterior teeth and the en masse distalization of
the maxillary dentition. Using infrazygomatic crest mini-implants
or interradicular mini-implants. The outcome measures are bone
stress, the amount of retraction and the amount of intrusion of
maxillary teeth.
Methodology
CT scans of human skulls were obtained in DICOM format.
These images were then changed to STL images using MIMICS
8.11 software. The design of mini-implant used in this model was
obtained from Favanchor company, the inter-radicular mini-implant
was of 1.6*10 mm in size and infrazygomatic mini-implant
of size 2*12 mm. Using these geometric models of lines and surfaces
were made and surface model of a finite element model tool
was using HYPERMESH software version 10.0. ABAQUS software
was used for material design. The hinge portion of maxilla
was fixed in all degrees of freedom.
Once the maxilla model was generated the upper teeth were set
up with metal brackets of MBT system and all tooth aligned, with
wire of 19*25 dimension stainless steel (Figure 1). For the model
to be used for en masse anterior retraction , the first premolar
was removed from both the sides. (Figure 2) En masse distalization
setup was done and brackets placed till the second molars
(Figure 3).
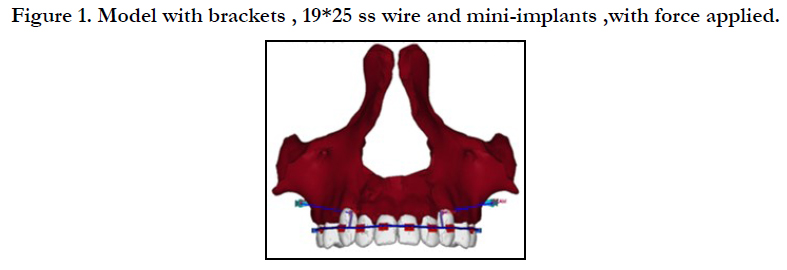
Figure 1. Model with brackets , 19*25 ss wire and mini-implants ,with force applied.
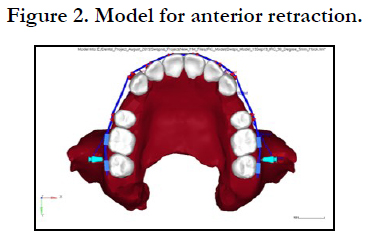

Figure 2. Model for anterior retraction.
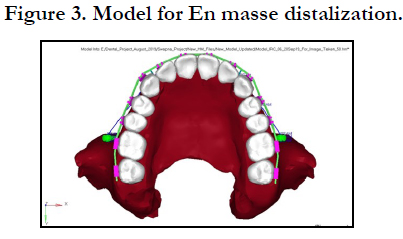
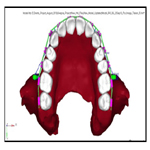
Figure 3. Model for En masse distalization.
The infra-zygomatic crest mini-implant were placed between the 1st and 2nd molar 13mm above the CEJ at 5 different angulation of 50, 60, 70, 80 and 90° from the level of the occlusal plane. The orientation perpendicular to the buccal bone was taken as 90° and reduction of 10 degrees [11].
The interradicular mini-implant was placed between the tooth roots of 2nd premolar and 1st molar at 7mm above the CEJ at 3 different angulations of 30, 40 and 50° from the level of the occlusal plane. The miniscrews placed in maxilla are usually placed at 30-40° to the long axis of the posterior teeth and whereas in mandible 10-20 degrees of angulation in the mandible.
Anteriorly retraction hooks of 8mm length were placed between the lateral incisor and canine. For the en masse anterior retraction model the force applied on either side was fixed at 200 gms per side and en masse distalization model 300 gms per side using niti coil springs. This model of maxilla was fixed in all directions and discretized in X, Y and Z axis.
Results
The properties of the materials used in this FEM set-up has been
depicted in young’s modulus and as poisson’s ratio in Table 1 and
they were assumed to be isotropic and homogenous.
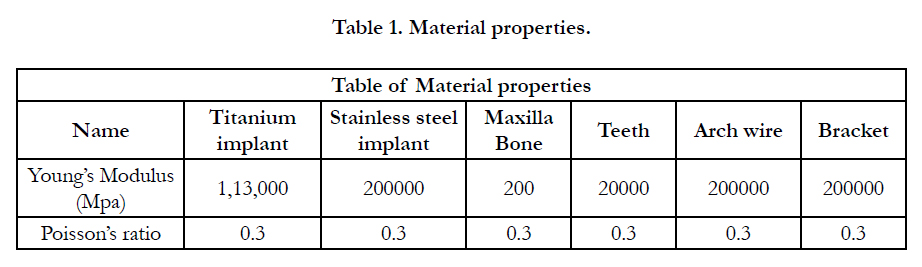

Table 1. Material properties.
Table 2 depicts the results of Von mises test , the bone stress patterns when infrazygomatic crest mini-implants and interradicular mini-implants when used for en masse distalization and en masse retraction. Maximum bone stress is noted when the angulation was reduced in IZC mini-implants. There was no significant difference in the stress levels when mini-implants were tried with different angulations. Figure 4 is a depiction of von mises test.
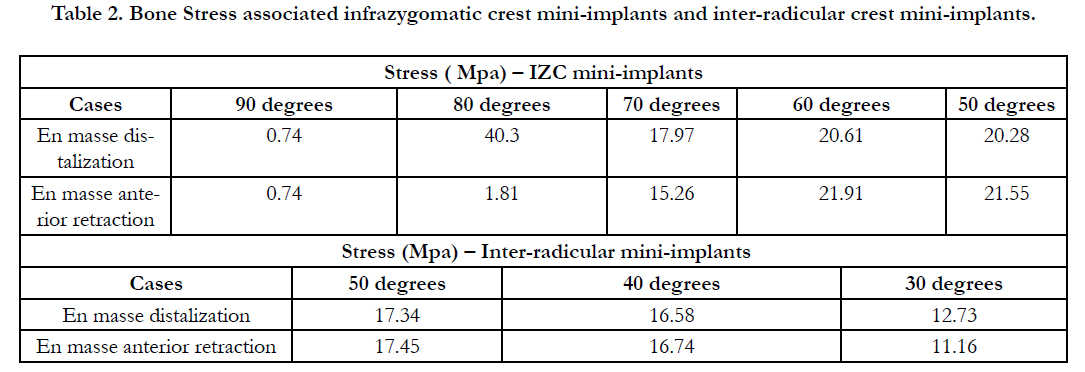
Table 2. Bone Stress associated infrazygomatic crest mini-implants and inter-radicular crest mini-implants.
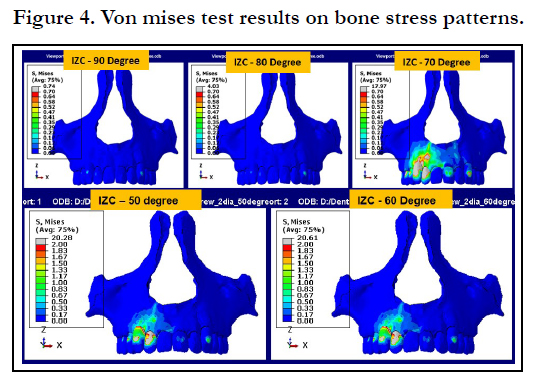
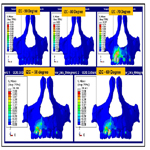
Figure 4. Von mises test results on bone stress patterns.
The magnitude of backward movement or the retraction of anterior teeth is shown in Table 3, the infrazygomatic crest miniimplant at 70 degrees brought about maximum movement when used for both the en masse distalization model ad en masse anterior retraction model whereas there is no significant difference in the movement between the various angles tried for inter-radicular mini-implants. IZC mini-implants brought about more distalization when compared to inter-radicular mini-screws. Figure 5 is a depiction of the the results of the distal movements in magnitude. Table 4 is used to explain the movement in magnitude in the z direction or the intrusive movement . Maximum intrusive movement was noted when force was applied with IZC, the intrusive movement is almost negligible when seen with inter-radicular implants. Figure 6 explains the studies that revealed in displacement in intrusive movements.
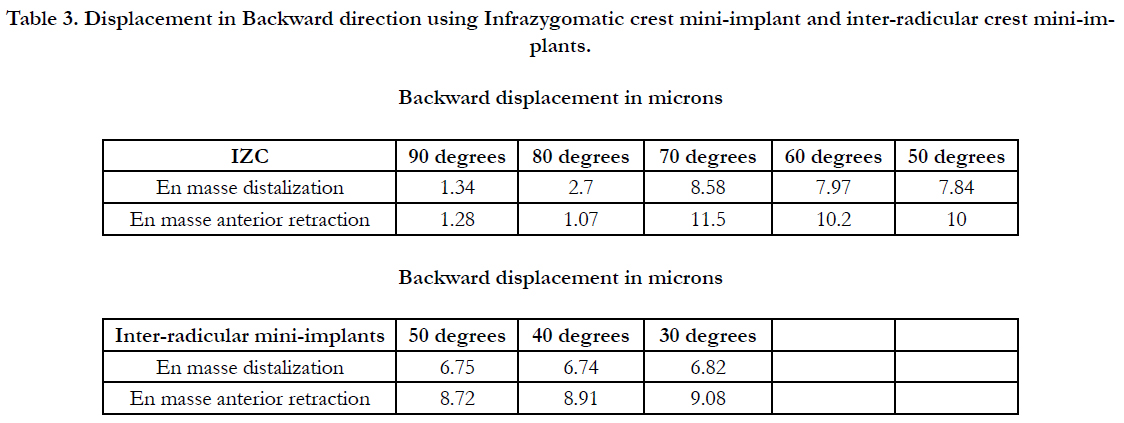
Table 3. Displacement in Backward direction using Infrazygomatic crest mini-implant and inter-radicular crest mini-implants.
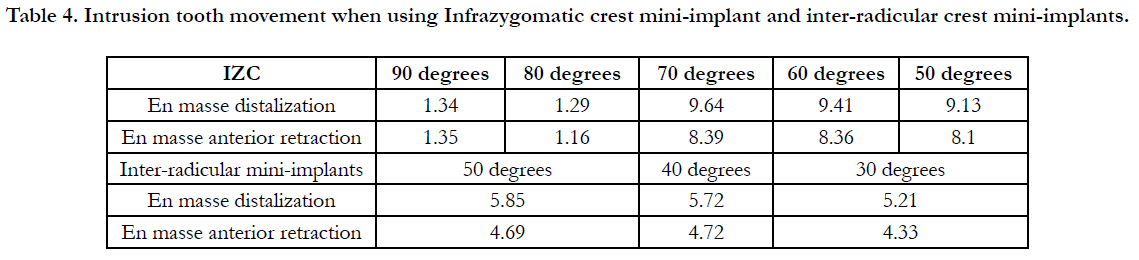
Table 4. Intrusion tooth movement when using Infrazygomatic crest mini-implant and inter-radicular crest mini-implants.
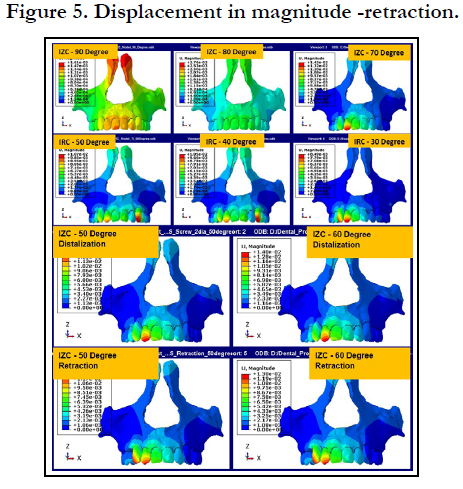
Figure 5. Displacement in magnitude -retraction.
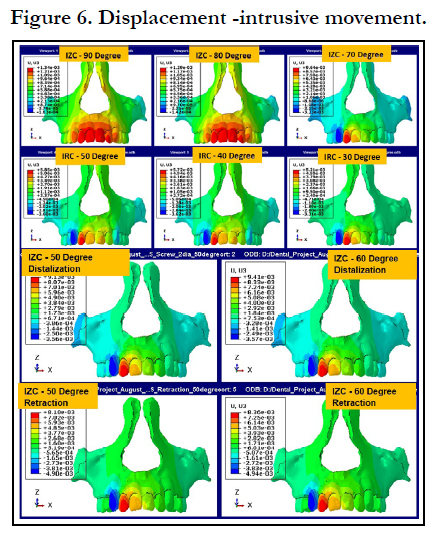
Figure 6. Displacement -intrusive movement.
Discussion
[14] One of the perceived complications of the retraction of upper
anterior teeth using sliding mechanics is the extrusion of the
upper anterior teeth during the retraction process. This would
be a particular risk for patients presenting with a high smile line
or vertical maxillary excess [14]. The use of mini-implants can
reduce this side effect.Miniscrews in posterior maxilla are used
to bring about various tooth movement mainly the retraction of
anterior teeth and the distalization of all the teeth [15]. The orthodontic mini implants can be useful not only as a skeletal anchorage,
but also for torque control during retraction [16]. The
true retraction will take place when the force passes through the
centre of resistance of the anterior teeth.When mini-screws are
placed between the second premolar and the first molar there is
increase in rotation of anterior teeth and the vertical movement
is reduced. For en masse distalization infrazygomatic crest miniimplants
are mostly indicated however it has been proposed that
interradicular implants can be used for the same effect [5].
There are various studies both in-vitro and in FEM models where
mini-implants have been widely researched in order to evaluate
the results on retraction of anterior teeth and for en masse anterior
retraction. This study is the first of its kind to evaluate and
compare the infrazygomatic crest mini-implants and the interradicular
mini-implants and to gain an understanding of the bone
stress patterns This study also aimed at establishing which miniimplant
was better for the purpose of en masse retraction of the
anterior teeth and for the en masse distalization of all the teeth of
the maxilla. The main change due to the orthodontic treatment
is due to tissue reaction either through bone or within the bone,
hence it is essential to study the stress patterns [15].
From the results of our study there is greater bone stress when
infra zygomatic crest mini-implants are placed at 70 degrees and
when interradicular mini-implants are placed at 40 and 50 degrees.
There is no significant difference between Infrazygomatic implant
and interradicular mini-implant in bringing about anterior
en masse anterior retraction. However, infra zygomatic crest mini-
implants is better for en masse distalization of the maxillary
dentition.
Using Interradicular mini-implant there is no significant intrusion.
The mini-implants placed at an increase in the acute angulation
has a potential to engage more cortical bone thickness, there is
also a disadvantage that too acute an angulation will cause slippage
during placement [16] Liou has established that insertion
angle of 30 to 70 degrees from the occlusal plane is sufficient to
allow adequate cortical bone engagement and more success of the mini-implants which is in accordance with the results of our
study [17].
In a previous study conducted there was no significant level of
difference in stress and magnitude when comparing the titanium
and stainless steel mini-screws. In the present study we have used
titanium mini-screw in both the regions in order to eliminate bias
that can arise from different material properties.
FEM is only an approximation technique and are highly dependent
on the models generated. There is an inability to predict long
term effects and movement and stress distribution after force application.
Time dependant reactions are unpredictable and needs
clinical evidence.
Conclusion
For En masse distalization infrazygomatic crest mini-implants are
more efficient than inter-radicular mini-implants.
There is no significant difference between these two alternatives
for en masse retraction of the upper anterior teeth.
Infrazygomatic crest mini-implants are indicated when both retraction
and intrusion of the teeth is desirable.
Acknowledgements
The researchers didn’t receive any funding from external sources
for this project. We sincerely thank engineer Mr Ramkumar. M for
helping in the finite element model setup and analysis.
References
- Yamaguchi M, Inami T, Ito K, Kasai K, Tanimoto Y. Mini-Implants in the Anchorage Armamentarium: New Paradigms in the Orthodontics. International Journal of Biomaterials. 2012; 2012: 394121. Pubmed PMID: 22719763.
- Costa A, Pasta G, Bergamaschi G. Intraoral hard and soft tissue depths for temporary anchorage devices. Seminars in Orthodontics. 2005 Mar 1; 11(1): 10–5.
- Thiruvenkatachari B, Pavithranand A, Rajasigamani K, Kyung HM. Comparison and measurement of the amount of anchorage loss of the molars with and without the use of implant anchorage during canine retraction. American Journal of Orthodontics and Dentofacial Orthopedics. 2006 Apr 1;129(4):551–4. Pubmed PMID: 16627183.
- Chung KR, Choo H, Kim SH, Ngan P. Timely relocation of mini-implants for uninterrupted full-arch distalization. American journal of orthodontics and dentofacial orthopedics. 2010; 138(6): 839-849. Pubmed PMID: 21130344.
- Marya A. Finite Element Analysis and its Role in Orthodontics. Advances in Dentistry & Oral Health. 2016 Jul 28; 2: 5-6.
- CicciùM, BramantiE, CecchettiF, ScappaticciL, GuglielminoE, RisitanoG. Fem and Von Mises analyses of different dental implant shapes for masticatory loading distribution. Oral Implantol (Rome). 2014 Dec 27; 7(1): 1–10. Pubmed PMID: 25694795.
- Sung SJ, Jang GW, Chun YS, Moon YS. Effective en-masse retraction design with orthodontic mini-implant anchorage: A finite element analysis. American Journal of Orthodontics and Dentofacial Orthopedics. 2010 May 1; 137(5): 648–57. Pubmed PMID: 20451784.
- Hedayati Z, Hashemi SM, Zamiri B, Fattahi HR. Anchorage value of surgical titanium screws in orthodontic tooth movement. International Journal of Oral and Maxillofacial Surgery. 2007 Jul 1; 36(7): 588–92. Pubmed PMID: 17524619.
- Kim T, Suh J, Kim N, Lee M. Optimum conditions for parallel translation of maxillary anterior teeth under retraction force determined with the finite element method. American Journal of Orthodontics and Dentofacial Orthopedics. 2010 May 1;137(5):639–47. Pubmed PMID: 20451783.
- Ahuja S, Gupta S, Bhambri E, Ahuja V, Jaura BS. Comparison of conventional methods of simultaneous intrusion and retraction of maxillary anterior: a finite element analysis. Journal of Orthodontics. 2018 Oct 2; 45(4): 243–9. Pubmed PMID: 302806645.
- Chang C, Liu SSY, Roberts WE. Primary failure rate for 1680 extra-alveolar mandibular buccal shelf mini-screws placed in movable mucosa or attached gingiva. The Angle Orthodontist. 2015 Jan 20; 85(6): 905–10. Pubmed PMID: 25603272.
- Park HS, Jeong SH, Kwon OW. Factors affecting the clinical success of screw implants used as orthodontic anchorage. American Journal of Orthodontics and Dentofacial Orthopedics. 2006 Jul 1; 130(1): 18–25. Pubmed PMID: 16849067.
- Park HS, Kwon TG, Sung JH. Nonextraction Treatment with Microscrew Implants. The Angle Orthodontist. 2004 Aug 1;74(4): 539–49. Pubmed PMID: 15387034.
- Jeong GM, Sung SJ, Lee KJ, Chun YS, Mo SS. Finite-element investigation of the center of resistance of the maxillary dentition. Korean Journal of Orthodontics. 2009 Apr 1; 39(2): 83–94.
- Melsen B. Biological reaction of alveolar bone to orthodontic tooth movement. The Angle Orthodontist. 1999 Apr 1; 69(2): 151–8. Pubmed PMID: 10227556.
- Kravitz ND, Kusnoto B. Risks and complications of orthodontic miniscrews. American Journal of Orthodontics and Dentofacial Orthopedics. 2007 Apr 1; 131(4, Supplement): S43–51. Pubmed PMID: 17448385.
- Liou EJW, Pai BCJ, Lin JCY. Do miniscrews remain stationary under orthodontic forces?. American Journal of Orthodontics and Dentofacial Orthopedics. 2004 Jul 1; 126(1): 42–7. Pubmed PMID: 15224057.





