Prevalence and Severity of Periodontal and Oral Hygiene Status among 30-40 Years Old Adult Population Attending A Private Dental College- A Hospital Based Cross Sectional Study
Anupama Deepak1, Jayashri Prabakar2*, M. Jeevitha3
1 Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
2 Senior Lecturer, Department Of Public Health Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
3 Senior Lecturer, Department of Periodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
*Corresponding Author
Jayashri Prabakar,
Senior Lecturer, Department Of Public Health Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai,
600077, India.
Tel: +91 9841788803
E-mail: jayashri.sdc@saveetha.com
Received: November 10, 2020; Accepted: December 15, 2020; Published: December 18, 2020
Citation: Anupama Deepak, Jayashri Prabakar, M. Jeevitha. Prevalence and Severity of Periodontal and Oral Hygiene Status among 30-40 Years Old Adult Population Attending A Private Dental College- A Hospital Based Cross Sectional Study. Int J Dentistry Oral Sci. 2020;7(12):1242-1246. doi: dx.doi.org/10.19070/2377-8075-20000245
Copyright: Jayashri Prabakar©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Periodontitis or periodontal infection is a chronic inflammatory disease of the supporting tissues of teeth caused by specific microorganisms. They present clinical findings such as tooth mobility, periodontal pocket formation , gingival recession etc. They are associated with factors such as tobacco smoking, poor oral hygiene, plaque and calculus deposition. Generally, periodontal diseases are more common among the men diagnosed with oral habits. Tobacco smoking is one of the main reasons for poor periodontal status in men. The main aim of this study was to assess the prevalence and severity of periodontal status and oral hygiene status among the 30-40 years adult population attending a private dental college. This was a record based study with a sample size of 187, irrespective of their gender. This study was conducted in a university setting, Chennai. The data was then categorised according to their age groups, gender, Russels periodontal index values and OHIS index values. The coding was done in MS Excel Sheets. Results were then carried out using IBM SPSS Version 20.0 followed by tabulation and graphical illustration. Independent t-test was used to compare the mean Periodontal Index and OHI score with age and gender respectively. The results revealed that males (4.68± 2.46) were more prone for periodontal diseases than the females (2.26 ± 1.45) with high prevalence among the 35-40 years age group (4.09±3.59). In conclusion, periodontal diseases were highly prevalent among adults with poor oral hygiene.
2.Introduction
3.Material and Methods
4.Statistical Analysis
5.Results
6.Discussion
7.Conclusion
8.Refereces
Keywords
Oral Hygiene; OHIS Index; Periodontitis; Russell’s Periodontal Index.
Introduction
Periodontitis or periodontal infection is defined as an inflammatory
disease of the supporting tissues of teeth caused by specific
microorganisms resulting in destruction of the periodontal ligament
and alveolar bone with periodontal pocket formation [1].
This is a complex infectious disease due to bacterial interaction
with the host immunity responses. This infection is initiated by
specific invasive oral pathogens in the oral cavity. They colonise
and form dental plaque biofilms and calculus on the tooth’s surface.
The individual's host immune response plays a major role
in the disease pathogenesis. Dental plaque is an example of both
biofilm and microbial communities [2]. There are diversity ties
of bacterial species belonging to various periodontal flora of different
complexes [3]. The common organisms are the P. gingivalis,
A.actinomycetemcomitans, B.forsythus and Treponemas [4].
These species colonise in the oral cavity leading to destruction.
Oral hygiene maintenance is important to prevent diseases in the
oral cavity. Generally periodontal diseases are more commonly
seen in men, due to their oral habits like tobacco smoking and
other common reasons being stress and medications. The bacterial
infections when aggravated by habits like smoking can lead to
periodontitis. This is one of the most common diseases of the
oral cavity besides gingivitis [5]. Periodontal diseases are majorly
seen among the older age group due to the poor oral hygiene, diabetes,
medications, hereditary, lack of dental care and age related
diseases. Poor oral health associated with periodontal diseases can have an adverse effect on the individual’s systemic health like CVS
diseases, Diabetes, whereas in females, this is seen to be associated
with pregnancy related problems, whereas in children, it is seen in
the form of dental caries rather than periodontitis [6]. In children,
this can be prevented at an early age with the help of sealants that
form resin tags on the tooth and proper oral maintenance [7-10].
Dental caries are a widespread disease seen equally in men and
women. Treatment for prevention of dental caries in both adults
and children is the use of optimal fluoride containing toothpaste
[11, 12]. Tobacco in the form of smokeless form or smoking form
is the main reason for poor oral hygiene statuses seen in men.
Negative effects of smoking such as cigar, pipe etc can also have
effects on oral health [13, 14]. Studies have shown that smokers
are at 3 times greater risk than the non smokers [15]. Lack Of
proper tooth brushing can lead to plaque deposition [16]. Recent
advances such as the toothpastes containing Nova min, Bio min,
Remin Pro have been proven to reduce the caries progression
[17]. The usage of Poor oral hygiene is linked to periodontal diseases.
Nutrition plays a major role in maintaining the balance between
the body and oral health [18]. This leads to accumulation of
dental plaque and calculus [19]. Females are also equally affected.
Normally, the high prevalence in middle aged women is mostly
seen during their menstruation and at menopausal stages due to
high levels of progesterone levels [20]. Another reason being the
stress, which reduces the flow of salivary secretions leading to
dental plaque formation [21, 22]. This leads to the progression of
dental caries and adhesion of bacteria on the tooth surface [23].
There are various by which this can be treated. Individuals who
lack accessibility to dental care can maintain their oral hygiene at
home with the recent advances like green tea mouth rinse and
other herbal formulations that prevent plaque deposition [24, 25].
There were various complications of periodontal diseases associated
with poor oral hygiene. This can affect systemic health due to
various risk factors. Therefore, the aim of this study was to assess
the prevalence of periodontal disease status on oral hygiene status
among the adult population.
This present study was a descriptive, record based study conducted
in a university setting at Saveetha dental college, Chennai . Case
sheets of all the Patients of OP Department of Saveetha dental
college were reviewed for a period of two months [June 2019 and
April 2020]. Simple Random Sampling was carried out to select
a total of 187 patients. This retrospective study was approved by
the following ethical approval number of the university, SDC/
SIHEC/2020/DIASDATA/0619-0320. The sampling bias was
minimised by using a simple random technique of data collection.
The internal validity of the study was the random selection of
subjects and universally accepted Russell’s periodontal index and
OHI-S index.
Assessment of Periodontal disease was carried out using Russell’s
periodontal index by Russell AI for permanent dentition. The
tooth was scored according to the criterias into 0 (negative), 1
(mild gingivitis), 2 (gingivitis), 4 (used only when radiographs are
available), 6 (gingivitis with pocket formation) and 8 (advanced destruction with loss of masticatory function). The total of these
scores was then calculated and assigned Clinically normal suppurative
tissues (0-0.2), Simple gingivitis (0.3-0.9), Beginning destructive
periodontal disease (1-1.9), Established destructive periodontal
disease (2-4.9) and Terminal disease (5-8).
Assessment of Oral hygiene was carried out using an oral hygiene
index simplified (OHI-S) by Greene and Vermillion for permanent
dentition. The tooth was scored according to the presence
of debris and calculus present and given scoring of 0, if there
were no debris or stains present, 1 if there was soft debris or
calculus covering not more than one third of tooth’s surface, 2
if there was soft debris or calculus covering more than one third
of tooth’s surface, 3 if there was soft debris or calculus covering
more than two thirds of tooth’s surface. The total of these scores
was then calculated separately and assigned good (0-1.2), fair (1.3-
3) and poor (3.1-6).
The data was then entered in MS Excel Sheets and excel tabulation
was done. The data was then imported to SPSS. Graphical
and table illustration was done by variable definition process.
The statistical tests used were the descriptive and inferential statistics.
The software used was the IBM SPSS Version 20.0. The dependent
variables were the Periodontal Index and OHI-S whereas
the independent variables were the age and gender. Descriptive
statistics were expressed by means of frequency, percentage, mean
and standard deviation. Independent t-test was used to compare
the mean Periodontal Index and OHIS score with age and gender
respectively. Pearson correlation was used to find the relationship
between Periodontal Index and OHIS score.
Results And Discussion
In the present study, from Figure 1, 36% of subjects belonged
to the 30-34 years age group and 64% of subjects belonged to
the 35-40 years age group and from Figure 2, 39.8 % of subjects
were females and 60.2% of subjects were males. From Figure 3,
it is observed that among 30-34 years, the mean value was (2.3
±2.92) whereas in 35-40 years, the mean value was (4.5±3.59) respectively.
There was a statistically significant difference observed
on comparison of age with mean Russell’s periodontal index using
Independent t-test. From Figure 4, on comparison between
gender with mean Russell’s periodontal index, females (5.0±1.45)
were more prone for caries than males (2.9±2.46) with a p-value
less than 0.05 and were found to be statistically significant. From
Figure 5, On comparison between age and mean OHIS , it is observed
that among 30-34 years the mean is (2.16±0.87) whereas
in 35-40 years, the mean is (2.47±0.85) with a p-value of 0.99
having an insignificant association. From Figure 6, on comparison
between gender with mean OHIS, there was no much difference
among the females (2.12±0.90) and males (2.09±0.84) with a pvalue
of 0.00 and were found to be statistically significant.
Periodontitis is a constant potential source of infection in poor
oral hygiene. This disease has a greater risk in systemic health [26].
Chronic periodontitis/ localised periodontitis is an infectious inflammatory disease with potential risk factors and complications
[27]. Children, adolescents and adults can be equally affected with
this disease [28]. Fair to poor OHI-S scores shows persistent increase
in the periodontal index score. Higher scores were seen in
the beginning of periodontal destruction, which means that the
periodontal destruction is correlated with poor oral hygiene [29].
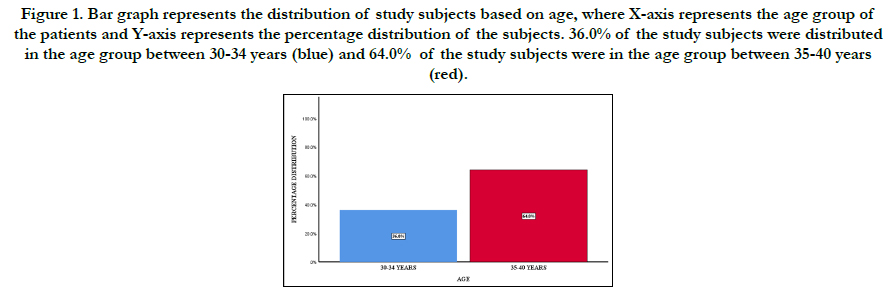
Figure 1. Bar graph represents the distribution of study subjects based on age, where X-axis represents the age group of the patients and Y-axis represents the percentage distribution of the subjects. 36.0% of the study subjects were distributed in the age group between 30-34 years (blue) and 64.0% of the study subjects were in the age group between 35-40 years (red).
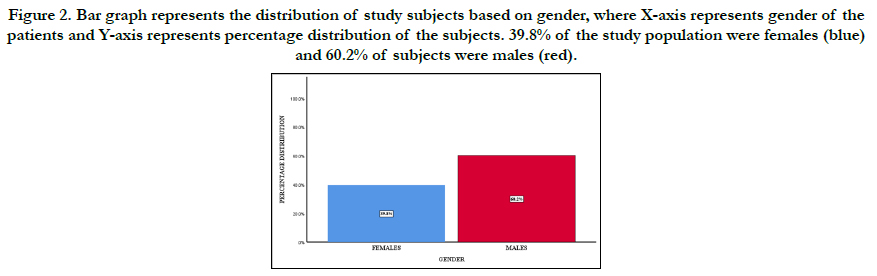
Figure 2. Bar graph represents the distribution of study subjects based on gender, where X-axis represents gender of the patients and Y-axis represents percentage distribution of the subjects. 39.8% of the study population were females (blue) and 60.2% of subjects were males (red).
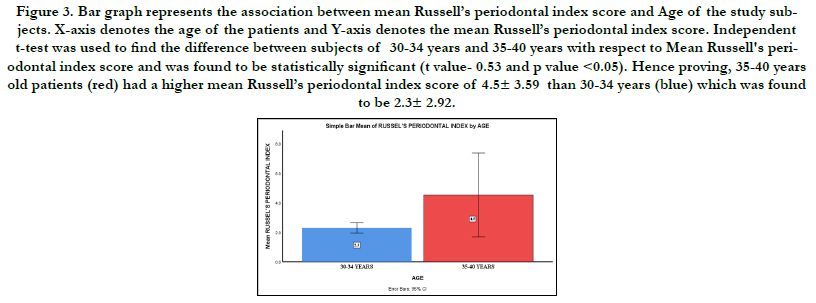
Figure 3. Bar graph represents the association between mean Russell’s periodontal index score and Age of the study subjects. X-axis denotes the age of the patients and Y-axis denotes the mean Russell’s periodontal index score. Independent t-test was used to find the difference between subjects of 30-34 years and 35-40 years with respect to Mean Russell's periodontal index score and was found to be statistically significant (t value- 0.53 and p value <0.05). Hence proving, 35-40 years old patients (red) had a higher mean Russell’s periodontal index score of 4.5± 3.59 than 30-34 years (blue) which was found to be 2.3± 2.92.
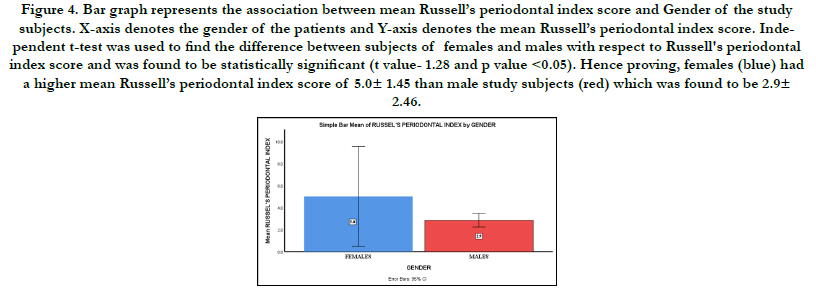
Figure 4. Bar graph represents the association between mean Russell’s periodontal index score and Gender of the study subjects. X-axis denotes the gender of the patients and Y-axis denotes the mean Russell’s periodontal index score. Independent t-test was used to find the difference between subjects of females and males with respect to Russell's periodontal index score and was found to be statistically significant (t value- 1.28 and p value <0.05). Hence proving, females (blue) had a higher mean Russell’s periodontal index score of 5.0± 1.45 than male study subjects (red) which was found to be 2.9± 2.46.
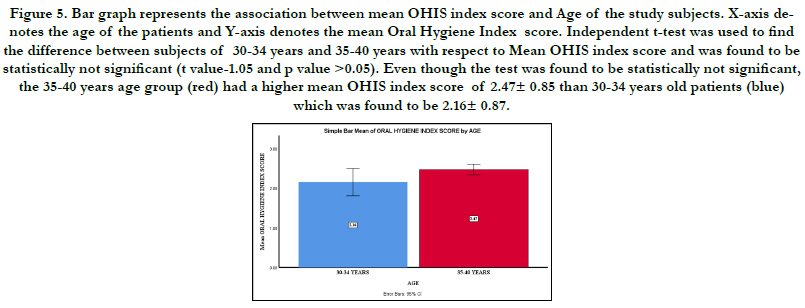
Figure 5. Bar graph represents the association between mean OHIS index score and Age of the study subjects. X-axis denotes the age of the patients and Y-axis denotes the mean Oral Hygiene Index score. Independent t-test was used to find the difference between subjects of 30-34 years and 35-40 years with respect to Mean OHIS index score and was found to be statistically not significant (t value-1.05 and p value >0.05). Even though the test was found to be statistically not significant, the 35-40 years age group (red) had a higher mean OHIS index score of 2.47± 0.85 than 30-34 years old patients (blue) which was found to be 2.16± 0.87.
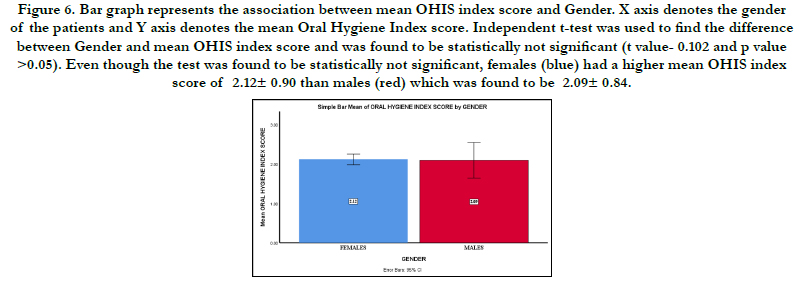
Figure 6. Bar graph represents the association between mean OHIS index score and Gender. X axis denotes the gender of the patients and Y axis denotes the mean Oral Hygiene Index score. Independent t-test was used to find the difference between Gender and mean OHIS index score and was found to be statistically not significant (t value- 0.102 and p value >0.05). Even though the test was found to be statistically not significant, females (blue) had a higher mean OHIS index score of 2.12± 0.90 than males (red) which was found to be 2.09± 0.84.
Good oral hygiene and oral care habits should be promoted in public health campaigns. Periodontal diseases can be prevented if one understands its complications [30]. Goal setting, self-planning is important. People should monitor their local hygiene [31]. Age is one of the most common risk factors. It is commonly seen in the older age group and increases with age [32]. Periodontal diseases are seen with increased bone loss, commonly due to accumulation of plaque and this eventually results in tooth mobility [33]. Sex also plays a major role , especially in males with oral habits than femals which predisposes to periodontal diseases [34]. Genetics play a role in the juvenile and aggressive periodontics with poor oral hygiene. This is significantly associated with adults [35]. Studies have been conducted by the United States showing 80% are prevalent in the older age group [36].
The OHI-S was assessed using both the soft and hard deposits and this study was similar to a study done with fair status showing high prevalence [37]. Public health services play a role in eliminating this disease and by creating awareness of the complications and management strategies [38]. There are various approaches for treating this disease. Main step in the prevention of this disease is by proper tooth brushing and flossing [39] followed by supragingival irrigation by scaling [40] and subgingival irrigation [41]. Periodontal scaling procedures are done to remove the calculus and plaque on the tooth. This is a mechanical type of irrigation. Root planing is also done alongside scaling [42]. This helps in pocket regression. Other various techniques are the host modulation [43] and antimicrobial therapy [44]. Public awareness must be created in order to reduce the mass disaster caused due to dental caries and poor oral hygiene [45]. The limitations of this study was the small sample size and geographic limitations. The future scope of this study is to create awareness on the effect of periodontal disease status on poor oral hygiene status among adults.
Conclusion
Therefore, in conclusion, periodontal diseases are highly prevalent
in the adult population, commonly in males (60.22%) among
the 38-40 years age group with poor oral hygiene.
Acknowledgement
The authors would like to acknowledge the support rendered by
The Department of Public Health Dentistry of Saveetha Dental
College and Hospitals and the management for their constant assistance
with the research.
References
- Newman MG, Takei H, Klokkevold PR, Carranza FA. Carranza's clinical 2]. Marsh PD. Dental plaque as a biofilm and a microbial community–implications for health and disease. In BMC Oral health. 2006 Jun; 6(1): 1-7.
- Socransky SS, Haffajee AD. The bacterial etiology of destructive periodontal disease: current concepts. J Periodontol. 1992 Apr; 63 (4 Suppl): 322-31. PMID: 1573546.
- Ezzo PJ, Cutler CW. Microorganisms as risk indicators for periodontal disease. Periodontol 2000. 2003; 32: 24-35. PMID: 12756031.
- Raitapuro-Murray T, Molleson TI, Hughes FJ. The prevalence of periodontal disease in a Romano-British population c. 200-400 AD. Br Dent J. 2014 Oct; 217(8): 459-66. PMID: 25342357.
- Prabakar J, John J, Srisakthi D. Prevalence of dental caries and treatment needs among school going children of Chandigarh. Indian J Dent Res. 2016 Sep-Oct; 27(5): 547-552. PMID: 27966516.
- Prabakar J, John J, Arumugham IM, Kumar RP, Sakthi DS. Comparative Evaluation of the Viscosity and Length of Resin Tags of Conventional and Hydrophilic Pit and Fissure Sealants on Permanent Molars: An In vitro Study. Contemp Clin Dent. 2018 Jul-Sep; 9(3): 388-394. PMID: 30166832.
- Prabakar J, John J, Arumugham IM, Kumar RP, Srisakthi D. Comparative Evaluation of Retention, Cariostatic Effect and Discoloration of Conventional and Hydrophilic Sealants - A Single Blinded Randomized Split Mouth Clinical Trial. Contemp Clin Dent. 2018 Sep; 9(Suppl 2): S233-S239. PMID: 30294150.
- Samuel SR, Acharya S, Rao JC. School Interventions-based Prevention of Early-Childhood Caries among 3-5-year-old children from very low socioeconomic status: Two-year randomized trial. J Public Health Dent. 2020 Jan; 80(1): 51-60. PMID: 31710096.
- Khatri SG, Madan KA, Srinivasan SR, Acharya S. Retention of moisturetolerant fluoride-releasing sealant and amorphous calcium phosphate-containing sealant in 6-9-year-old children: A randomized controlled trial. J Indian Soc Pedod Prev Dent. 2019 Jan-Mar; 37(1): 92-98. PMID: 30804314.
- Kumar RP, Vijayalakshmi B. Assessment of fluoride concentration in ground water in Madurai district, Tamil Nadu, India. Research Journal of Pharmacy and Technology. 2017; 10(1): 309-10.
- Kumar RP, Preethi R. Assessment of Water Quality and Pollution of Porur, Chembarambakkam and Puzhal Lake. Research Journal of Pharmacy and Technology. 2017; 10(7): 2157-9.
- Underner M, Maes I, Urban T, Meurice JC. Effects of smoking on periodontal disease. Revue des maladies respiratoires. 2009 Dec 1; 26(10): 1057-73.
- Leelavathi L. Nicotine Replacement Therapy for Smoking Cessation-An Overview. Indian Journal of Public Health Research & Development. 2019 Nov 1; 10(11).
- Johnson GK, Hill M. Cigarette smoking and the periodontal patient. J Periodontol. 2004 Feb;75(2):196-209. PMID: 15068107.
- de Oliveira C, Watt R, Hamer M. Toothbrushing, inflammation, and risk of cardiovascular disease: results from Scottish Health Survey. Bmj. 2010 May 27; 340.
- Mohapatra S, Kumar RP, Arumugham IM, Sakthi D, Jayashri P. Assessment of Microhardness of Enamel Carious Like Lesions After Treatment with Nova Min, Bio Min and Remin Pro Containing Toothpastes: An in Vitro Study. Indian Journal of Public Health Research & Development. 2019; 10(10): 375-80.
- Neralla M, Jayabalan J, George R, Rajan J, MP SK, Haque AE, et al. Role of nutrition in rehabilitation of patients following surgery for oral squamous cell carcinoma. International Journal of Research in Pharmaceutical Sciences. 2019 Oct 16; 10(4): 3197-203.
- Albandar JM, Rams TE. Global epidemiology of periodontal diseases: an overview. Periodontol 2000. 2002; 29: 7-10. PMID: 12102700.
- Markou E, Boura E, Tsalikis L, Deligianidis A, Konstantinidis A. The influence of sex hormones on proinflammatory cytokines in gingiva of periodontally healthy premenopausal women. J Periodontal Res. 2011 Oct; 46(5): 528-32. PMID: 21501171.
- Reners M, Brecx M. Stress and periodontal disease. International journal of dental hygiene. 2007 Nov; 5(4): 199-204.
- Pratha AA, Prabakar J. Comparing the effect of Carbonated and energy drinks on salivary pH-In Vivo Randomized Controlled Trial. Research Journal of Pharmacy and Technology. 2019; 12(10): 4699-702.
- Mathew MG, Samuel SR, Soni AJ, Roopa KB. Evaluation of adhesion of Streptococcus mutans, plaque accumulation on zirconia and stainless steel crowns, and surrounding gingival inflammation in primary molars: randomized controlled trial. Clin Oral Investig. 2020 Sep; 24(9): 3275-3280. PMID: 31955271.
- Pavithra RP, Jayashri P. Influence of Naturally Occurring Phytochemicals on Oral Health. Research Journal of Pharmacy and Technology. 2019; 12(8): 3979-83.
- Prabakar J, John J, Arumugham IM, Kumar RP, Sakthi DS. Comparing the Effectiveness of Probiotic, Green Tea, and Chlorhexidine- and Fluoride-containing Dentifrices on Oral Microbial Flora: A Double-blind, Randomized Clinical Trial. Contemp Clin Dent. 2018 Oct-Dec; 9(4): 560-569. PMID: 31772463.
- Ohyama H, Nakasho K, Yamanegi K, Noiri Y, Kuhara A, Kato-Kogoe N, et al. An unusual autopsy case of pyogenic liver abscess caused by periodontal bacteria. Jpn J Infect Dis. 2009 Sep;62(5):381-3. PMID: 19762989.
- Fowler EB, Breault LG, Cuenin MF. Periodontal disease and its association with systemic disease. Mil Med. 2001 Jan;166(1):85-9. PMID: 11197106.
- Armitage GC. Comparison of the microbiological features of chronic and aggressive periodontitis. Periodontol 2000. 2010 Jun;53:70-88. PMID: 20403106.
- . Bakdash B. Oral Hygiene and Compliance as Risk Factors in Periodontitis. J Periodontol. 1994 May; 65 Suppl 5S:539-544. PMID: 29539762.
- Tonetti MS, Eickholz P, Loos BG, Papapanou P, van der Velden U, Armitage G, et al. Principles in prevention of periodontal diseases: Consensus report of group 1 of the 11th European Workshop on Periodontology on effective prevention of periodontal and peri-implant diseases. J Clin Periodontol. 2015 Apr; 42 Suppl 16:S5-11. PMID: 25639948.
- Slot DE, Van der Weijden FA. Group A. Initiator paper. Plaque control: home remedies practiced in developing countries. Journal of the International Academy of Periodontology. 2015 Jan;17(1 Suppl):4.
- Den Grossi SG, Skrepcinski FB, DeCaro T, Zambon JJ, Cummins D, Genco RJ. Response to periodontal therapy in diabetics and smokers. J Periodontol. 1996 Oct;67(10 Suppl):1094-102. PMID: 8910828.
- Löe H, Anerud A, Boysen H, Morrison E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46 years of age. J Clin Periodontol. 1986 May; 13(5): 431-45. PMID: 3487557.
- Slade GD, Spencer AJ. Periodontal attachment loss among adults aged 60+ in South Australia. Community Dent Oral Epidemiol. 1995 Aug;23(4):237- 42. PMID: 7587146.
- Hart TC. Genetic considerations of risk in human periodontal disease. Curr Opin Periodontol. 1994:3-11. PMID: 8032464.
- Yellowitz JA. Geriatric health and functional issues. The ADA practical guide to patients with medical conditions. 2015 Oct 19:405-22.
- Parkar SM, Patel N, Patel N, Zinzuwadia H. Dental health status of visually impaired individuals attending special school for blind in Ahmedabad city, India. Indian J Oral Sci. 2014 May 1;5(2):73.
- Ryan ME. Nonsurgical approaches for the treatment of periodontal diseases. Dent Clin North Am. 2005 Jul;49(3):611-36. PMID: 15978244.
- Bader HI. Floss or die: implications for dental professionals. Dent Today. 1998 Jul;17(7):76-8, 80-2. PMID: 9796462.
- Newman MG, Cattabriga M, Etienne D, Flemmig T, Sanz M, Kornman KS, et al. Effectiveness of adjunctive irrigation in early periodontitis: multicenter evaluation. J Periodontol. 1994 Mar;65(3):224-9. PMID: 8164116.
- Boyd RL, Hollander BN, Eakle WS. Comparison of a subgingivally placed cannula oral irrigator tip with a supragingivally placed standard irrigator tip. J Clin Periodontol. 1992 May; 19(5): 340-4. PMID: 1517479.
- Cobb CM. Non-surgical pocket therapy: mechanical. Ann Periodontol. 1996 Nov;1(1):443-90. PMID: 9118268.
- Oringer RJ. Research, science, and therapy committee of the American 3. Academy of Periodontology. Modulation of the host response in periodontal therapy. J Periodontol. 2002 Apr;73(4):460-70.
- Slots J, Rams TE. Antibiotics in periodontal therapy: advantages and disadvantages. J Clin Periodontol. 1990 Aug; 17(7 ( Pt 2)): 479-93. PMID: 2202744.
- KANNAN SS, KUMAR VS, RATHINAVELU PK, INDIRAN MA. AWARENESS AND ATTITUDE TOWARDS MASS DISASTER AND ITS MANAGEMENT AMONG HOUSE SURGEONS IN A DENTAL COLLEGE AND HOSPITAL IN CHENNAI, INDIA. WIT Transactions on The Built Environment. 2017 Sep 7; 173: 121-9.





