The Effect of Grape Seed Extract Mouth Rinse on the Caries Activity, Dental plaque and Gingivitis
Wahdan MA Elkwatehy1*, Rabab I. Salama1
1 Assistant Professors of Paediatric, Dental Public Health and Preventive Dentistry, Faculty of Dentistry, Mansoura University, Egypt.
*Corresponding Author
Wahdan M.A. Elkwatehy,
Assistant professors of Paediatric, Dental Public Health and Preventive Dentistry, Faculty of Dentistry, Mansoura University, Egypt.
Tel: 00966582396965
E-mail: elkwatehywahdan@gmail.com
Received: October 20, 2020; Accepted: November 25, 2020; Published: December 07, 2020
Citation:Wahdan MA Elkwatehy, Rabab I. Salama. The Effect of Grape Seed Extract Mouthrinse on the Caries Activity, Dental plaque and Gingivitis. Int J Dentistry Oral Sci. 2020;7(12):1148-1152. doi: dx.doi.org/10.19070/2377-8075-20000228
Copyright: Wahdan M.A. Elkwatehy©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objectives: This study aimed to evaluate the effect of mouth rinse containing grape seed extract (GSE)on caries activity, plaque
accumulation and gingivitis.
Material and Methods: A total of ninety-five healthy children participate in a clinical trial, they divided into two groups, group
1: grape seed extract mouth rinse (prepared for this study) (test group) and group 2: chlorhexidine mouth rinse (positive control
group). The evaluation of caries activity, dental plaque accumulation and gingivitis were done prior to and on weekly basis for 3
weeks. The effect of mouth rinses was evaluated using one-way ANOVA test to compare baseline scores with different follow up
scores. Multiple comparisons within each group were done using Post-hoc test. Comparison between the two groups was done
using Un-paired t test. p values less than 0.05 were considered statistically significant.
Results: The efficacy of GSE mouth rinse was comparable to that of chlorhexidine in reducing the dental caries activity, dental
plaque accumulation and gingivitis.
Conclusion: GSE mouth rinse may be used as a self-applied preventive measure to maintain healthy oral and dental tissues in
the future.
2.Introduction
3.Materials and Methods
4.Results and Discussion
5.Limitations
6.Acknowledgement and Declarations
7.Refereces
Keywords
Caries Activity; Grape Seed Extract; Oratest; Dental Plaque; Gingivitis.
Introduction
Prevention of oral diseases is very important to maintain good
oral health condition; children usually neglect oral hygiene measures
leading to active and uncontrolled dental diseases which
subsequently affecting their general health [1]. Dental decay and
gingivitis are the most prevalent dental disease in children, oral
micro-organisms and bacterial plaque attached to tooth surface
are responsible for initiation and progression of these diseases
[2, 3].
The dental diseases are preventable not curable diseases, so dental
healthcare workers should focus on preventive dentistry. Various
preventable agents developed for self-care at home [4]. Mouth
rinses containing antimicrobial agents used as supplements to
daily homecare for prevention of bacterial plaque. Synthetic antimicrobial
agents usually had several side effects while natural
products have been used for thousands of years in medicine. All
this directing toward using natural therapeutic agents for prevention
of oral diseases such as dental caries [5, 6].
Grape seed extract (GSE) contains high concentration of proanthocyanidin,
it represents a variety of polymers of flavanol such
as monomeric catechin and epicatechin, gallic acid and polyphenols
[7, 8]. Proanthocyanidin (condensed tannin) has several clinical
uses and has been used as dietary supplements, it strengthens
collagen-based tissues by collagen synthesis and accelerates the
conversion of soluble collagen to insoluble collagen [6, 9, 10].
GSE act as antioxidant, antimicrobial and free radical scavenger
[11, 12]. It has a remineralizing potential on artificial carious lesions
of enamel, inhibits the proliferation of cariogenic bacteria and
reduce the synthesis of dental plaque [13, 14]. Also, it has
anti-inflammatory action and immune response enhancement,
thus, might be used as natural antimicrobial agent in preventive
dentistry [15].
Oratest is diagnostic test used to determine microbial load in saliva. It is used to assess periodontal disease as there is high correlation
between the plaque and gingival indices and Oratest scores
[16]. It is simple, inexpensive and rapid caries activity test helps
in identification of high caries risk individuals [17]. The Oratest
make the management of dental disease easier by determine and
customize the most suitable therapeutic preventive measures, it
used as an index to check the effectiveness of treatment instilled
[18].
The literature indicated that, GSE is effective against streptococcus
mutans in vitro but limited information is available regarding
its effect in vivo. The comparative effect of these active agents
on caries activity, dental plaque and gingivitis using Oratest is not
studied yet. So, this trial was designed to evaluate their efficacy in
vivo.
This trial designed to:-
1- Evaluate the efficacy of GSE mouth rinse on the caries activity, dental plaque and gingivitis.
2- Compare the efficacy of GSE with that of commercially available chlorhexidine mouth rinse.
The study design is clinical trial which carried out at the dental
clinic of Pediatric, Dental Public Health and Preventive Dentistry
Department, Faculty of Dentistry, Mansoura University, Egypt. after obtaining the ethical approval
from institutional ethical committee. Written informed
consents were obtained from the children's parents after understanding
the aim of the study.
The target population was children aged from 9-12 years old. By
calculating the sample size with confidence interval 95% and marginal
error of 5 % and expected percentages of caries activity
of 50%. The calculated sample size was (90 subjects) which was
increased to 95 subjects.
- Children with an age range from 9 - 12 years.
- Children with high caries risk detected by dental caries scores
(DMFT + dft≥ 3).
- Children not brushing their teeth or brushing once before the
bedtime and had fair to poor plaque accumulation according to
Silness and LÖe Index.
- Moderate to severe gingivitis according to LÖe and Silness Index.
- Children with systemic disorders.
- Children taken antibiotic within one month before the study.
- Baseline Oratest score more than 25 minutes.
107 participants meeting inclusion criteria were selected from
children seeking treatment in Pediatric Dentistry Department.
101 subjects from the selected 107 who their parents signed the
informed consents were included in this study. Later, 6 participants
have baseline Oratest score more than 25 minutes were excluded
and the remaining 95 children formed the study sample.
- Chlorhexidine (Hexitol, The Arab Drug Company, Cairo,
Egypt) (Group I = Positive control). Commercially available chlorhexidine
mouthwash contains 0.12% chlorhexidine gluconate.
- Grape Seed Extract (GSE) mouthwash (Group II = Test
group). It was prepared for this study and contains 2 % Grape
Seed Extract and other ingredients like that found in chlorhexidine
mouthrinse.
- Oratest armamentarium:-
1. Sterile beakers & Screw cap test tubes.
2. Sterilized milk & 0.1% Methylene blue solution.
3. 10ml disposable syringes & sterile pipettes.
4. Mirror & test tube stand.
The study sample was stratified into three groups according to
dental caries scores, from (3-5), (6-10) and (11 or more). Each
stratum subsequently divided according to the gender into males
and females substrata, from the final substrata the two study
groups were allocated randomly, group I [47(25 female + 22
male)] children and group II [48(25 female + 23 male)] children.
Both participants and researcher who carried out caries activity
test, plaque and gingivitis scoring were blind to the study materials
used. The collected data was also analysed by an external statician.
This trial was carried out by two researchers. One of them perform
randomization and the other one performs clinical examination
and Oratest procedure all over the study. To ensure the
consistency of the measurements during the study period, intra
examiner consistency was obtained by training and calibration before
starting the study and during it. The intra examiner consistency
was tested by Kappa test and weighted kappa test was 90 %.
Demographic characters, frequency of tooth brushing/day,
Number of dental visits/years, dental plaque and gingival indexes
scores, dental caries experience and caries activity (Oratest scores)
were recorded as baseline data.
0.1% methylene blue was prepared by mixing 100 mg of methylene blue in 100 ml of distilled water. Every child was instructed
to rinse his mouth thoroughly with 10 ml of sterilized milk for 30
seconds then expectorate in a sterile beaker. 3 ml of expectorate
was added to a screw cap test tube containing 0.12 ml of 0.1%
methylene blue. Then content of the tube mixed thoroughly, and
a mirror was used to detect any color change (blue to white) at the
bottom of the tube every 5 minutes, the time taken for the initiation
of color change was recorded [19].
The children in both groups were instructed to rinse their mouths
with (5 ml) of mouth rinse for five minutes in the morning before
school time and at evening before the bedtime (daily for one
week). To ensure the children compliance, a bottle contains 100ml
of mouth washes enough for one-week use was supplied to each
childand the extra return mouth rinses were calculated. Parents
were instructed to supervise their children during the rinsing procedures
and fill the supplied checklist.
Plaque Index and Gingival Index scoring and Oratest procedure
were carried out at the end of 1st, 2nd, and 3rd weeks from the
beginning of the mouth washes usage to evaluate and compare
their effect.
Data was collected and analyzed using SPSS version 21(IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp).
Independent t test was used to compare between the two groups
at baseline and different follow up intervals. One-way ANOVA
and post Hoc Tukey tests were used to evaluate the effect of each
mouth wash and compare among the scores of the different follow
up intervals in the same group. The p values less than 0.05
were considered statistically significant.
Results
At baseline; there were no significant differences between the
2 groups as regards age (p=0.138), brushing frequency/day
(p=0.339), number of dental visits/year (p=0.080) and DMFT +
dft scores (p=0.068) (Table 1), Oratest scores (p=0.451), dental
plaque (p=0.302) and gingivitis (p=0.984)(Table 2).
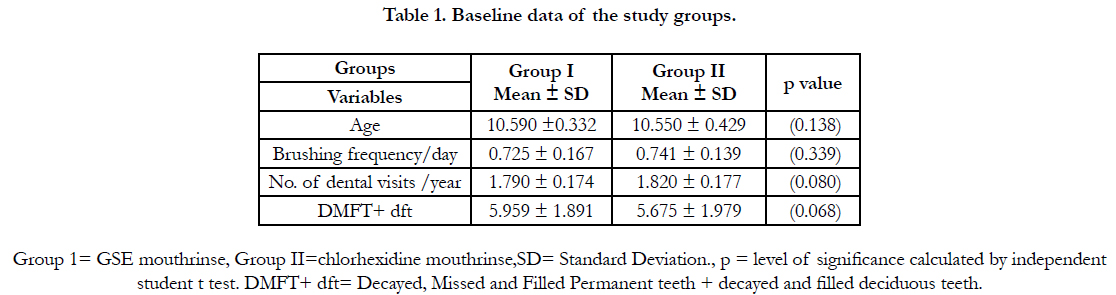

Table 1. Baseline data of the study groups.
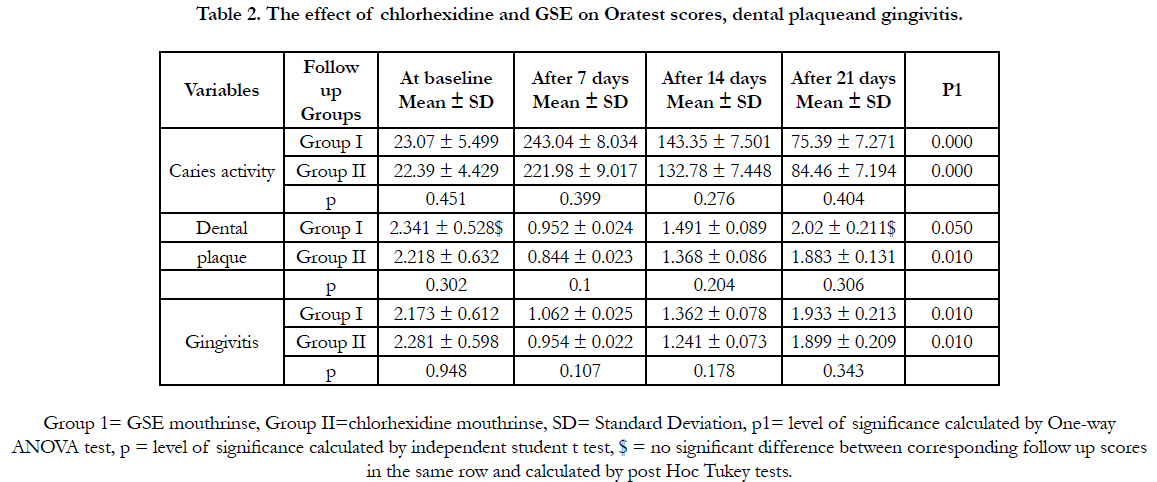
Table 2. The effect of chlorhexidine and GSE on Oratest scores, dental plaqueand gingivitis.
Both chlorhexidine and GSE mouthrinses produce statistically significant reduction in; caries activity (increased time required for colour change by Oratest) (p= 0.000 for both), dental plaque scores (p=0.050 and p=0.010 respectively) and gingivitis scores (p= 0.010 for both) (Table 2).
Post hoc test revealed that, both chlorhexidine and GSE mouthrinses exhibited statistically significant effect on caries activity, dental plaque and gingivitis at all time intervals compared to each other or compared to baseline scores except dental plaque score for week three in group I compared to baseline. Student's t test revealed that, there were no significant differences between the two groups at all time intervals (Table 2, graph 1, 2 and 3).
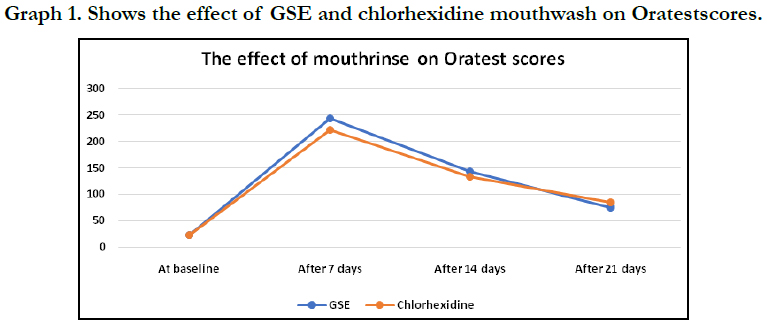
Graph 1. Shows the effect of GSE and chlorhexidine mouthwash on Oratestscores.
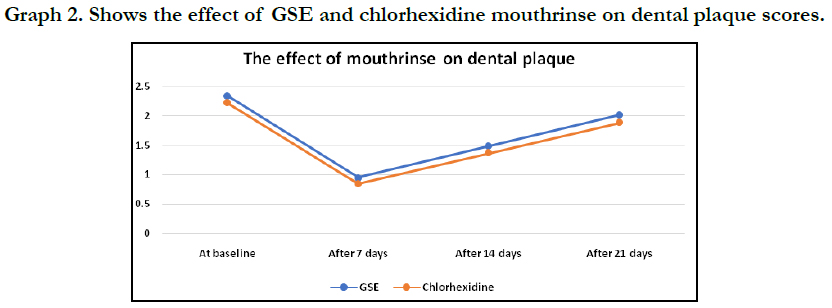
Graph 2. Shows the effect of GSE and chlorhexidine mouthrinse on dental plaque scores.
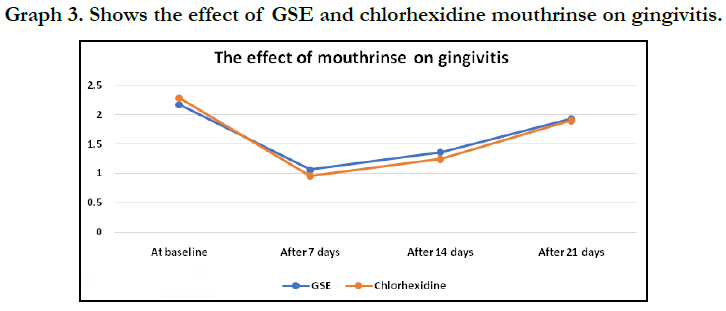
Graph 3. Shows the effect of GSE and chlorhexidine mouthrinse on gingivitis.
Discussion
The prevalence of dental diseases was increased among children
and to prevent the initiation of such diseases and overcome its
sequelae advocated the use of natural product with antimicrobial
potential. This study was carried out to evaluate the effect of GSE
mouthrinse on the caries activity, plaque accumulation and gingival
inflammation in comparison with chlorhexidine mouth rinse.
Chlorhexidine was used as positive control because several studies
proved its antimicrobial activity and use it as gold standard for
evaluating the antimicrobial efficacy of other antimicrobial agents
[20-22].
Oratest was used in present trial to evaluate the efficacy of GSE
compared to chlorhexidine because it is simple non-invasive
test,needs minimal armamentarium, acceptable for children assuring
greater patient compliance [23]. Oratest is effective and
reliable in assessment of caries activity and gingivitis, there were
inverse relation between salivary bacterial load and time taken for
the change in the color of methylene blue and vice versa [24, 28,
16].
The significant increase in time of colour change in the present
study (Oratest scores) may be due to the antimicrobial effect of
GSE and chlorhexidine which reduce the bacterial load in saliva
and subsequently reduced rate of oxygen depletion [25].
Ourresults indicated a significant reducing effect of both mouth
rinses on caries activity, plaque and gingival indexes when comparing
the scores at baseline with the scores at different time intervals
(Table 2). The effect of GSE and chlorhexidine mouth
rinses was comparable to each other where there were no significant
differences between them as regards caries activity, gingival
and plaque indexes scores at different follow up intervals (Table
2, graph I, 2 and 3). The reduction in caries activity was in accordance
with previous studies concluded that, GSE inhibits enamel
caries in vitro due to its ability to suppress growth of cariogenic
bacteria and plaque formation as well as promoting dental remineralization
[13, 26].
The reduction in dental plaque and gingivitis scores were in accordance
with the other studies used GSE mouth rinse and produced
significant reduction in the gingivitis score, the improved
gingival condition may be due to antimicrobial effect of GSE (reduction
in dental plaque biofilm) [22], anti-inflammatory properties
of bioactive antioxidants in GSE (polyphenols, catechin, and
flavanol) [27-29] and increases collagen synthesis and accelerates
the conversion of soluble collagen to insoluble collagen as GSE
is a rich source of proanthocyanidin [6].
The present findings support results of another study evaluate the
antimicrobial, anti-gingivitis, and anti-caries effect of GSE and
suggested the future possibility of its utilization in preventive and
restorative materials to preserve the dental health [30].
Conclusion
We can conclude that,GSE mouthrinse have anti-caries, antiplaque
and anti-gingivitis effect like that of 0.12% chlorhexidine
gluconate mouthrinse. GSE can be used as safe mouth rinse for
short term maintenance therapy with an advantage of having no
side effects as it was used as dietary supplement and antioxidant.
Recommendation
Further research is recommended to test the efficacy of GSE
mouth rinse on larger population as the present study is the first
one evaluating the GSE as a mouth rinse to prove anti-caries, antigingival
and anti-plaque effects.
References
- Mc Donalds RE, Avery DR, Dean JA. Dentistry for child and Adolescent. 7th edn. St Louis: CV Mosby; 2000;415-24.
- Shafer WG, Hine MK. A textbook of oral pathology. 5th edn 1993; 567-68.
- Marsh PD. Dental Plaque as Microbial Biofilm. J Caries Res. 2004; 38: 204- 11.
- Harris NO, Godoy G. Primary Preventive Dentistry .6thedn. Julie Levin Alexander .2004; 1-22.
- Xie Q, Bedran-Russo AK, Wu CD. In vitro remineralization effects of grape seed extract on artificial root caries. Journal of dentistry. 2008 Nov 1;36(11):900-6.
- Wu CD. Grape products and oral health. J Nutr. 2009 Sep;139(9):1818S- 23S. Pubmed PMID: 19640974.
- Monagas M, Gómez-Cordovés C, Bartolomé B, Laureano O, Ricardo da Silva JM. Monomeric, oligomeric, and polymeric flavan-3-ol composition of wines and grapes from Vitis vinifera L. Cv. Graciano, Tempranillo, and Cabernet Sauvignon. J Agric Food Chem. 2003 Oct 22;51(22):6475-81. Pubmed PMID: 14558765.
- Nakamura Y, Tsuji S, Tonogai Y. Analysis of proanthocyanidinsin grape seed extracts, health foods and grape seed oils. Journal of Health Science. 2003;49:45-54.
- Yamakoshi J, Saito M, Kataoka S, Kikuchi M. Safety evaluation of proanthocyanidin rich extract from grape seeds. Food Chem Toxicol. 2002;40:599- 07.Pubmed PMID: 11955665.
- Ray S, Bagchi D, Lim PM, Bagchi M, Gross SM, Kothari SC, et al. Acute and long-term safety evaluation of a novel IH636 grape seed proanthocyanidin extract. Res Commun Mol Pathol Pharmacol. 2001 Mar- Apr;109(3-4):165-97.Pubmed PMID: 11758648.
- Furiga A, Lonvaud-Funel A, Badet C. In vitro study of antioxidantcapacity and antibacterial activity on oral anaerobes of a grape seed extract Food Chemistry.2009;113:1037-40.
- Kao TT, Tu HC, Chang WN, Chen BH, Shi YY, Chang TC, et al. Grape seed extract inhibits the growth and pathogenicity of Staphylococcus aureus by interfering with dihydrofolate reductase activity and folate-mediated one-carbon metabolism. Int J Food Microbiol. 2010 Jun 30;141(1-2):17-27. Pubmed PMID: 20483185.
- Zhao W, Xie Q, Bedran-Russo AK, Pan S, Ling J, Wu CD. The preventive effect of grape seed extract on artificial enamel caries progression in a microbial biofilm-induced caries model. J Dent. 2014 Aug;42(8):1010-8. Pubmed PMID: 24863939.
- . Rubel M, Prashant GM, NAVEEN KP, Sushanth VH, MOHAMED IMRANULLA IP, MALLICK S. Effect of grape seed extract on remineralization of artificial caries: An in-vitro study. Asian J Pharm Clin Res. 2016;9(5):174- 6.
- Alkedaide AQ. The Anti-inflammatory effect of grape seed extract in rats exposed to Cadmium Chloride toxicity.Inter J Advanced Res. 2015, 3(7): 298-05.
- Joshi M, Jayakumar, Joshi N. Comparative evaluation for assessing Oratest as a diagnostic tool for evaluation of plaque levels and gingivitis.Journal of Dental and Allied Sciences. 2012 Jul 1;1(2):52.
- Sundaram M, Nayak UA, Ramalingam K, Reddy V, Rao AP, Mathian M. A comparative evaluation of Oratest with the microbiological method of assessing caries activity in children. J Pharm Bioallied Sci. 2013 Jun;5(Suppl 1):S5-9. Pubmed PMID: 23946577.
- Chandak S, Kesri R, Bhardwaj A. Milk, a simple tool to detect caries activity: Oratest. Int J Prev Clin Dent Res. 2016; 3(2): 98-101.?
- Rosenberg M, Barki M, Portnoy SA. A simple method for estimating oral microbial level. J Microbial Methods. 1989;9:253‑7.
- Nadkerny PV, Ravishankar PL, Pramod V, Agarwal LA, Bhandari S.A comparative evaluation of the efficacy of probiotic and chlorhexidine mouthrinses on clinical inflammatory parameters of gingivitis: A randomized controlled clinical study. J Indian Soc Periodontol. 2015; 19(6): 633–9.
- Eshwar S, Rekha K, JainV, et al. Comparison of Dill Seed Oil Mouth Rinse and Chlorhexidine Mouth Rinse on Plaque Levels and Gingivitis - A Double Blind Randomized Clinical Trial. Open Dent J. 2016 May 11;10:207-13. Pubmed PMID: 27386006.
- Jain I, Jain P. Comparative evaluation of antimicrobial efficacy of three different formulations of mouth rinses with multi herbal mouth rinse. J Indian Soc Pedod Prev Dent. 2016;34:315-23.PubmedPMID: 27681394.
- Jauhari D, Srivastava N, Rana V, Chandna P. Comparative Evaluation of the Effects of Fluoride Mouthrinse, Herbal Mouthrinse and Oil Pulling on the Caries Activity and Streptococcus mutans Count using Oratest and Dentocult SM Strip Mutans Kit. Int J Clin Pediatr Dent. 2015;8(2):114-8.Pubmed PMID: 26379378.
- Desai VB, Chiranjeevi, Thakur L. A clinic pathological study: Evaluation of gingival inflammation using Oratest. J Ind Soc Periodontol.1997;21:68‑70.
- Bhasin S, Sudha P, Anegundi RT. Chair side simple caries activitytest: Oral test. J Ind Soc Pedod Prev Dent. 2006;24(2): 76-9.PubmedPMID: 16823231.
- Delimont NM, Carlson BN. Prevention of dental caries by grape seed extract supplementation: A systematic review. Nutrition and Health.2019; 26(1):43-52.Pubmed PMID: 31760860.
- Fernández-Larrea J, Pujadas G, Salvadó J, Arola L, Blay M. Modulatory effect of grape-seed procyanidins on local and systemic inflammation in diet-induced obesity rats. J Nutr Biochem. 2011 Apr;22(4):380-7. Pubmed PMID: 20655715.
- Ahmad SF, Zoheir KM, Abdel-Hamied HE, Attia SM, Bakheet SA, Ashour AE, et al. Grape seed proanthocyanidin extract protects against carrageenaninduced lung inflammation in mice through reduction of pro-inflammatory markers and chemokine expressions. Inflammation. 2014 Apr;37(2):500-11. Pubmed PMID: 24162779.
- Yang G, Wang H, Kang Y, Zhu MJ. Grape seed extract improves epithelial structure and suppresses inflammation in ileum of IL-10-deficient mice. Food Funct. 2014 Oct;5(10):2558-63. Pubmed PMID: 25137131.
- Benjamin S, Sharma R, Thomas SS, Nainan MT. Grape seed extract as a potential remineralizing agent: a comparative in vitro study. J Contemp Dent Pract. 2012 Jul 1;13(4):425-30. Pubmed PMID: 23151686.





