Common Reasons for Premolar Extractions In Children Of Age Between 12 To 18 Years - A Retrospective Study
P. Kuzhalvaimozhi1, Vignesh Ravindran2*, Subhashini.V.C3
1 Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
2 Senior Lecturer, Department of Pediatric and Preventive Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
3 Tutor, Department of Public Health Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
*Corresponding Author
Vignesh Ravindran,
Senior Lecturer, Department of Pediatric and Preventive Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University,
Chennai, 600077, India.
E-mail: vigneshr.sdc@saveetha.com
Received: October 07, 2020; Accepted: November 22, 2020; Published: November 27, 2020
Citation: P. Kuzhalvaimozhi, Vignesh Ravindran, Subhashini.V.C. Common Reasons for Premolar Extractions In Children Of Age Between 12 To 18 Years - A Retrospective Study. Int J Dentistry Oral Sci. 2020;7(11):1136-1139. doi: dx.doi.org/10.19070/2377-8075-20000225
Copyright: Vignesh Ravindran© 2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Planned extraction of permanent teeth for orthodontic purposes is a challenging factor for the stability of the treatment, and for
successful esthetic and functional results. Dental extractions can also be due to caries, traumatic injuries and other periodontal
conditions. The most common reasons for extracting permanent premolars needs further analysis. Hence a study was conducted
to assess the common reasons for extraction of premolars among children between 12 to 18 years of age. A total of 86000 dental
records were analysed from the records of patients attending the dental institute and based on inclusion and exclusion criteria the
final study sample consisted of 100 patients who underwent premolar tooth extractions. Patient details, tooth extracted and the
reasons for extraction of premolars were noted. Data was tabulated and subjected to Chi-square test in SPSS software. The most
common reason for extraction of premolars among children between 12-18 years of age was orthodontic treatment. This was
noticed predominantly in children who were females due to esthetic concerns.
2.Introduction
3.Materials and Methods
4.Results and Discussion
5.Conclusion
6.Acknowledgements
7.References
Keywords
Extraction; Dental Caries; Malocclusion; Premolars.
Introduction
The main goal of the orthodontic treatment is to achieve the normal
relationship of the teeth with facial structures. Angle stated
that preservation of all dental structures was required to achieve
facial balance. However, there can be little soft tissue constraints
which limit the amount of alteration that can be corrected orthodontically,
which needs extraction [1-3]. According to Little
et al [4], in severe crowding cases which are greater than 9mm
may require extensive orthodontic therapy with tooth extractions.
There are many factors which require extraction of teeth for orthodontic
therapy- Increased tooth size arch length discrepancy
(crowding), open bite cases, impacted cases, supernumerary teeth,
malformed teeth, cleft lip and palate cases. The decision to extract
premolar teeth totally depends on cases, patient's medical history,
attitude to treatment, oral hygiene status, and caries rate of the
patients [5].
Extraction of permanent teeth at a younger age would be a complete
loss forever. The lost tooth wouldn't be replaced by a succeeding
tooth as in primary teeth [6]. The reasons for extraction
vary from dental caries, unrestorable teeth, periodontal problems,
traumatic dental injuries, root stumps, furcal involvement and also
for orthodontic purposes. Absence of a permanent tooth would
lead to space loss, supra eruptions, mesial migrations and also
pose a threat to adjacent teeth. This would affect the functionality
of the teeth, disruption in speech and also has an impact on
mastication [7-9]. Extraction of permanent molars and incisors
are commonly studied. There are minimal studies on the reasons
for extraction of premolars. So the aim of the study was to assess
the common reasons for extraction of premolars among children
between 12 to 18 years of age.
Materials And Methods
This retrospective study was carried out in a hospital based university setting. This study was evaluated and ethically approved by
an institutional ethical review committee (ethical approval number:
SDC/SIHEC/2020/DIASDATA/0619-0320).Retrospective
data collected from 9,000 case records from June 2019 to March
2020. Informed consent was obtained from the parents or guardian
before starting the treatment. Inclusion criteria were patients
aged from 12 to 18 years and patients who underwent permanent
tooth extractions, extraction of premolars, complete records of
the patient with fully filled case sheets and photographic evidence
of extraction done. Exclusion criteria were patients aged above 18
years, incomplete data records, absence of photographic evidence
of extraction and censored records.
Total cases acquired for this study were 100 which include patients
who underwent premolar extractions. Selected cases were
examined by two people: one researcher and one guide. Patient's
case sheets were reviewed thoroughly. Cross checking of data including
digital entry, removal of data records of the same patient
involved in multiple extractions and intraoral photographs was
done by an additional reviewer, and as a measure to minimise
sampling bias, samples for the group were picked by the simple
random sampling method. Digital entry of clinical examination
and intraoral photographs were assessed. Reasons for premolar
extraction were noted by a researcher, entered into Microsoft excel
(MS Excel) and then transferred into Statistical Package for the
Social Sciences (SPSS) Software for statistical analysis. A correlation
test (Chi-square test) was done between gender and reason
for premolar extraction. The difference was statistically significant
when the p-value was less than 0.05.
Results And Discussion
The final sample size consisted of 100 patients which includes
62 females and 38 males (Graph -1). This shows that most of the
study participants were females who underwent premolar extractions.
The main reason for premolar extractions in children aged
between 12 to 18 for orthodontic treatment (90%) and premolar
tooth extracted due to dental caries (10%). (Graph-2). Association
between the reasons for premolar extraction and gender shows
that 5% of female study participants extracted premolar due to
dental caries, 5% of male study participants extracted premolar
due to dental caries, 57% of female study participants extracted
premolar for orthodontic treatment and 33% of male study participants
extracted premolar for orthodontic treatment. Higher
number of children who were females (57) extracted premolars
for orthodontic reasons when compared to children who were
males (33), which was statistically significant. (p = 0.00).
Results of the present study suggests the most common reason
for extraction of premolars was orthodontic treatment which is
more predominant in females. Though there are no studies for
comparison, the reason for such a difference between the genders
was because the adolescents who were females were more concerned
on their esthetic appearances when compared to males.
Extraction for orthodontic reasons will be governed by three
factors such as condition of the teeth, positioning of crowding and position of teeth. High grossly decayed teeth, fractured teeth,
root canal treated teeth and teeth with large restorations are preferred
for extraction over healthy teeth. Main consideration is the
long term prognosis for the tooth rather than the appearance of
the tooth. Crowding in one part of the arch is more readily corrected
if extraction was done in that part than adjacent areas of
arch. In case of incisor crowding, premolars were extracted as it is
esthetic and occlusal balance is also maintained. First premolar is
positioned in the centre of each quadrant, is usually near the area
of crowding whether in the anterior or buccal segment. Hence,
premolars are most commonly extracted for orthodontic treatment.
Malaligned teeth which are difficult to align may often be
the teeth of choice for extraction. The position of the apex of the
tooth must be considered as it is difficult to move the apex than
crown [7, 10].
Another interesting pattern was noticed during initial stages of
data collection. Multiple premolar extractions were noticed in the
same patient records. The data finalised for the study did not consider
multiple extraction data of the same patient so as to eliminate
bias. Extraction of all [4] premolars, either first or second,
was the most common pattern noticed. This was due to the fact
that balanced extractions could preserve the concept of facial
symmetry. Certain sound healthy teeth may be extracted to facilitate
proper alignment of other teeth in cases of severe arch length
tooth material discrepancy. Such extraction of sound teeth for the
purpose of orthodontic treatment is called therapeutic extraction.
Wilkinson advocated extraction of entire 1s molars between the
age of 8.5 years and 9.5 years as this prevents impaction of 3rd
molars, relieves crowding in the arch, and helps in decreasing the
incidence and occurrence of dental caries [7].
However we could not find any data on premolar extraction prior
to 12 years of age. The concept of serial extraction was not
noticed in the present sample population however this method
would minimise the future orthodontic treatment duration. It
could also be due to the fact that parents were reluctant for extraction
of permanent teeth due to reasons other than pain or
decay. Serial extraction is the planned and sequential extraction
of certain deciduous teeth followed by removal of specific permanent
teeth in order to engage the spontaneous correction of irregularities [11-13].
Parents and children should work together to maintain good oral
hygiene. Good attitude of parents reflects as a good oral health in
children and vice versa [14-16]. Preservation of primary teeth in
the dental arch is important to guide the eruption of the permanent
teeth in the optimal position [17-19]. Grossly decayed primary
teeth which are extracted before exfoliation causes space in the
dental arch which causes malocclusion if space maintainer was
not given [20, 21]. Bacteria play a vital role in the initiation and
progression of pulpal and periodontal disease [22]. Untreated
dental caries eventually lead to pulpitis and periapical periodontitis
which is treated by means of root canal procedure or extracted
leading to space loss and malalignment which would require orthodontic
management [23, 24]. However maintenance of proper
oral hygiene would minimise such complications and preserve the
primary dentition minimising the orthodontic needs [25-28].
The strength of the study was that this was one of the few studies
that assess the common reasons for extraction of premolars. Although
this study has a high internal validity, the limitations of reduced
sample size, geographic and ethinic limitations of the study
sample would reduce the overall external validity of the study.
However the future scope would be to perform the study with
larger sample size and varied ethnicities to get a broader perspective
on understanding.
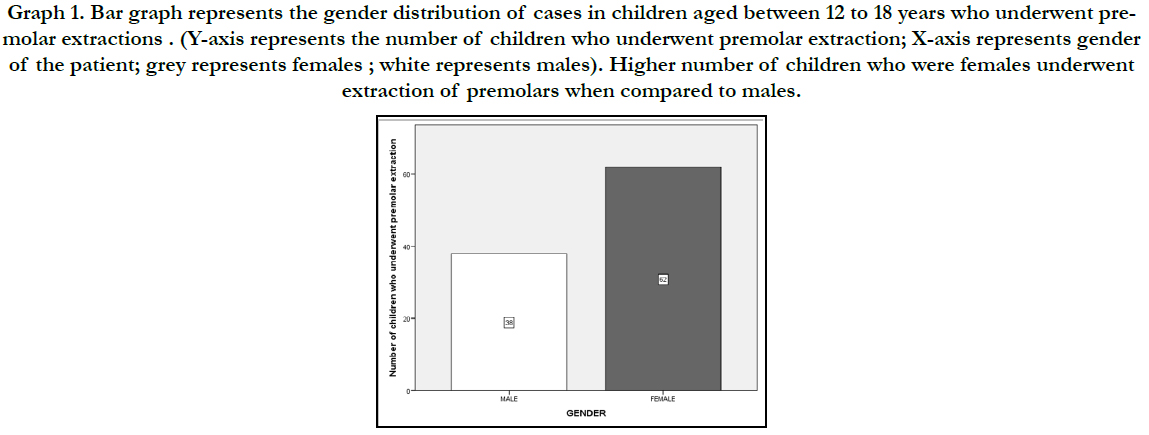
Figure 1. Pie chart represents the gender wise distribution of study population ,(dark blue)males and (pink) females. This graph shows that 42.3% of the study population were females and 57.6% of them were males.
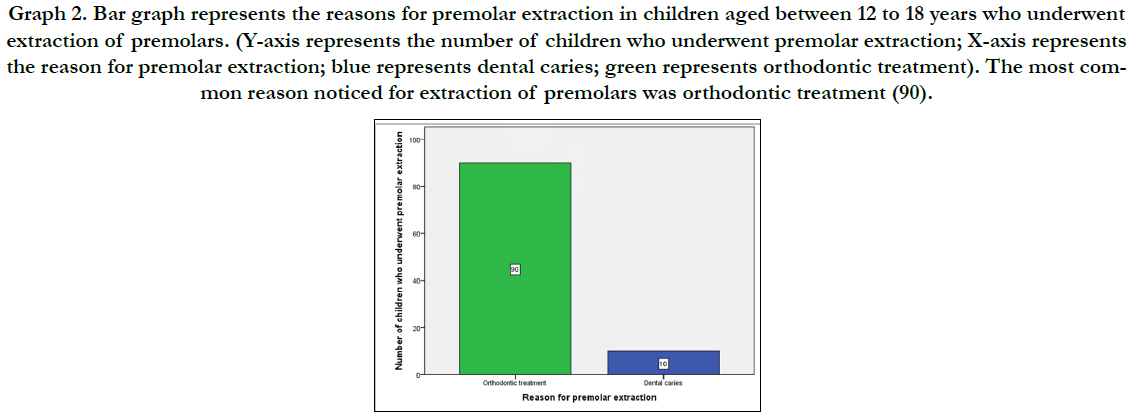
Figure 2. Pie chart represents the age wise distribution of study population . It also shows that 18.6% of the population belonged to the age group 20-30 years (maroon) , 10.1% of the population belonged to the age group 30-40 years (grey) , 20.3% of the population belonged to the age group 40-50 years (green) ,5.08% of the population belonged to the age group 50-60 years(orange) and 45.% of the population belonged to the age group 60-70 years (brown). From this we can infer that the age group of 60-70 years was high in population in this study.
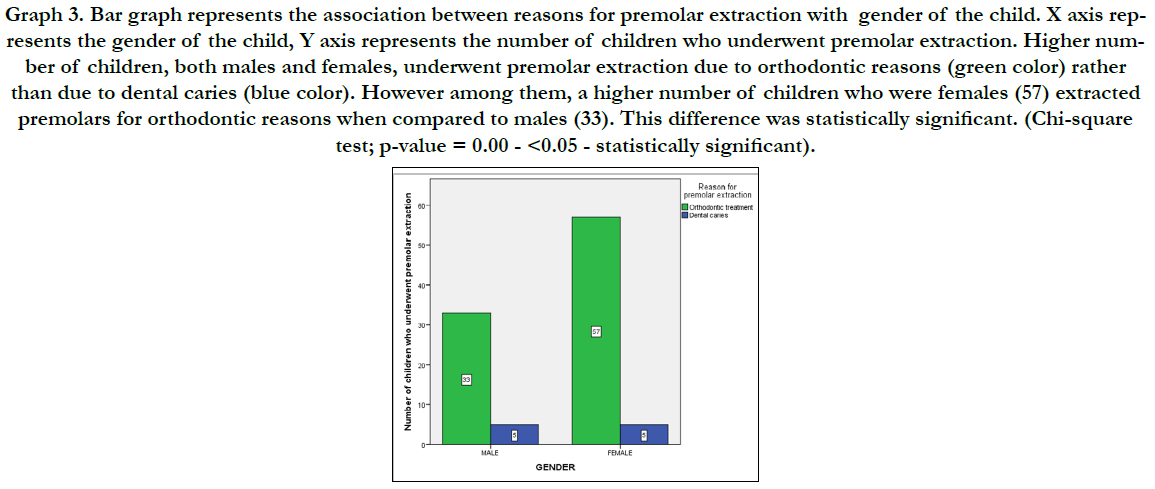
Figure 3. The clustered bar represents the distribution of study population based on age and suturing , X axis represents the age of the population and Y axis represents the percentage of study population. 32.0% of the patients belonging to the age group of 60-70 years did not have suture followed by 13.5% patients having suture belonging to the same age group.From this we can infer that , patients did not have suture for most of extractions. ( Chi square = 0.196 ;Df =4 ;P= 0.999 > P=0.05, statistically not significant)Association of suturing based on age was statistically not significant.
Conclusion
Within the limitations of the present study, the most common
reason for extraction of premolars among children between 12-
18 years of age was orthodontic treatment. This was noticed predominantly
in children who were females due to esthetic concerns.
Acknowledgment
The authors of this manuscript would like to acknowledge the
University for providing us access to patients’ data that was useful
to complete this retrospective study.
References
- Angle EH. Treatment of Malocculsion of the Teeth and Fractures of the Maxillæ. SS White dental manufacturing Company; 1900.
- Hulsey CM. An esthetic evaluation of lip-teeth relationships present in the smile. Am J Orthod. 1970 Feb;57(2):132-44. PMID: 5263359.
- Ackerman JL, Proffit WR. Soft tissue limitations in orthodontics: treatment planning guidelines. Angle Orthod. 1997;67(5):327-36. PMID: 9347106.
- Little RM. The irregularity index: a quantitative score of mandibular anterior alignment. Am J Orthod. 1975 Nov;68(5):554-63. PMID: 1059332.
- Travess H, Roberts-Harry D, Sandy J. Orthodontics. Part 8: Extractions in orthodontics. Br Dent J. 2004 Feb 28;196(4):195-203. PMID: 15039723.
- Williams R, Hosila FJ. The effect of different extraction sites upon incisor retraction. Am J Orthod. 1976 Apr;69(4):388-410. PMID: 1062936.
- Phulari BS. Orthodontics: principles and practice. JP Medical Ltd; 2011 May 30.
- Case CS. The question of extraction in orthodontia. American journal of orthodontics. 1964 Sep 1;50(9):660-91.
- Tweed CH. Clinical Orthodontics, Vol. 1. Mosby; 1966.
- . Millett D, Day P. Clinical Problem Solving in Orthodontics and Paediatric Dentistry E-Book. Elsevier Health Sciences; 2016 Oct 18.
- Finn SB. Clinical Pedodontics. 4 [sup] th ed. Philadephia: WB Saunders Company. 1991:454-74.
- Proffit WR, Fields Jr HW, Sarver DM. Contemporary orthodontics. Elsevier Health Sciences; 2006 Dec 8.
- Enlow DH, Hans MG. Essentials of facial growth. WB Saunders Company. 1996; 303.
- Gurunathan D, Shanmugaavel AK. Dental neglect among children in Chennai. J Indian Soc Pedod Prev Dent. 2016 Oct-Dec;34(4):364-9. PMID: 27681401.
- Somasundaram S, Ravi K, Rajapandian K, Gurunathan D. Fluoride Content of Bottled Drinking Water in Chennai, Tamilnadu. J Clin Diagn Res. 2015 Oct;9(10):ZC32-4. PMID: 26557612.
- Subramanyam D, Gurunathan D, Gaayathri R, Vishnu Priya V. Comparative evaluation of salivary malondialdehyde levels as a marker of lipid peroxidation in early childhood caries. Eur J Dent. 2018 Jan-Mar;12(1):67-70. PMID: 29657527.
- Packiri S, Gurunathan D, Selvarasu K. Management of Paediatric Oral Ranula: A Systematic Review. J Clin Diagn Res. 2017 Sep;11(9):ZE06-ZE09. PMID: 29207849.
- Christabel SL, Gurunathan D. Prevalence of type of frenal attachment and morphology of frenum in children, Chennai, Tamil Nadu. World J Dent. 2015 Oct; 6(4): 203-7.
- Govindaraju L, Gurunathan D. Effectiveness of Chewable Tooth Brush in Children-A Prospective Clinical Study. J Clin Diagn Res. 2017 Mar;11(3):ZC31-ZC34. PMID: 28511505.
- Ravikumar D, Jeevanandan G, Subramanian EMG. Evaluation of knowledge among general dentists in treatment of traumatic injuries in primary teeth: A cross-sectional questionnaire study. Eur J Dent. 2017 Apr- Jun;11(2):232-237. PMID: 28729799.
- Panchal V, Jeevanandan G, Subramanian E. Comparison of instrumentation time and obturation quality between hand K-file, H-files, and rotary Kedo-S in root canal treatment of primary teeth: A randomized controlled trial. J Indian Soc Pedod Prev Dent. 2019 Jan-Mar;37(1):75-79. PMID: 30804311.
- Jeevanandan G. Kedo-S Paediatric Rotary Files for Root Canal Preparation in Primary Teeth - Case Report. J Clin Diagn Res. 2017 Mar;11(3):ZR03- ZR05. PMID: 28511532.
- Govindaraju L, Jeevanandan G, Subramanian EMG. Comparison of quality of obturation and instrumentation time using hand files and two rotary file systems in primary molars: A single-blinded randomized controlled trial. Eur J Dent. 2017 Jul-Sep; 11(3): 376-379. PMID: 28932150.
- Jeevanandan G, Govindaraju L. Clinical comparison of Kedo-S paediatric rotary files vs manual instrumentation for root canal preparation in primary molars: a double blinded randomised clinical trial. Eur Arch Paediatr Dent. 2018 Aug;19(4):273-278. PMID: 30003514.
- Govindaraju L, Jeevanandan G, Subramanian E. Clinical Evaluation of Quality of Obturation and Instrumentation Time using Two Modified Rotary File Systems with Manual Instrumentation in Primary Teeth. J Clin Diagn Res. 2017 Sep;11(9):ZC55-ZC58. PMID: 29207834.
- Lakshmanan L, Mani G, Jeevanandan G, Ravindran V, Ganapathi SE. Assessing the quality of root canal filling and instrumentation time using kedo-s files, reciprocating files and k-files. Brazilian Dental Science. 2020 Jan 31;23(1):7.
- Ramakrishnan M, Bhurki M. Fluoride, Fluoridated Toothpaste Efficacy And Its Safety In Children-Review. International Journal of Pharmaceutical Research. 2018 Oct 1;10(04):109-14.
- Govindaraju L, Jeevanandan G, Subramanian EM. Knowledge and practice of rotary instrumentation in primary teeth among Indian dentists: a questionnaire survey. Journal of International Oral Health. 2017 Mar 1;9(2):45.





