Association Of Irreversible Pulpitis And Single Visit Root Canal Treatment
S.S. Shivanni1, Anjaneyulu K2*, Balakrishna R.N3
1 Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
2 Reader, Department of Conservative Dentistry and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
3 Senior Lecturer, Department of Oral and Maxillofacial Surgery, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
*Corresponding Author
Anjaneyulu K,
Reader, Department of Conservative Dentistry and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University,
Chennai, 600077, India.
E-mail: kanjaneyulu.sdc@saveetha.com
Received: October 07, 2020; Accepted: November 22, 2020; Published: November 27, 2020
Citation: S.S. Shivanni, Anjaneyulu K, Balakrishna R.N. Association Of Irreversible Pulpitis And Single Visit Root Canal Treatment. Int J Dentistry Oral Sci. 2020;7(11):1127-1131. doi: dx.doi.org/10.19070/2377-8075-20000223
Copyright: Anjaneyulu K© 2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Root canal treatment in a common procedure in dentistry. The main indications for RCT are irreversible pulpitis and necrosis of
dental pulp due to caries or dental trauma.The aim of this study was to assess the number of single visit RCT done in irreversible
pulpitis cases. The study includes patients visiting the OP of Saveetha Dental College diagnosed with irreversible pulpitis who have
undergone Single - visit RCT. The results were statistically analysed and graphs were tabulated. Single visit RCT was less prevalent
among the population (43.40%) than multi visit RCT (56.60%). Male predominance was found to be higher with a percentage of
(50.75%). The association of gender and number of visits for RCT shows that single visit RCT was more prevalent among females
(22.01%) than males (21.38%) and chi square test shows a positive significance (p value = 0.000). The incidence of single-visit RCT
was lower than multi-visit RCT. The type of RCT to be done depends on the amount of inflammation and extent of the lesion. It
can also be based on the patient’s preference, as patients might want the treatment to be done in a single visit.
2.Introduction
3.Materials and Methods
4.Results and Discussion
5.Conclusion
6.Acknowledgements
7.References
Keywords
Irreversible Pulpitis; Single-Visit RCT; Multi Visit RCT; Male Predominance.
Introduction
Irreversible pulpitis, is characterised by acute and intense pain
and is one of the most frequent reasons for patients to attend
emergency dental care. Apart from extraction, the customary way
of relieving the pain of irreversible pulpitis is by removing the
inflamed pulp and cleaning the root canal [1].
The symptoms usually include a history of spontaneous pain
which may also involve an exaggerated response to hot or cold
that lingers after the stimulus is removed [2]. Any tooth may be affected
by irreversible pulpitis. It is not restricted to any particular
age group and it usually occurs as a direct result of dental caries,
cracked teeth or trauma and thus tends to occur more frequently
in older patients. The involved tooth is usually not sensitive
to percussion, and palpation tests do not produce any reaction.
The characteristics of irreversible pulpitis are a vital pulp which
responds to cold and electric pulp testing. Cold may actually alleviate
the pain of irreversible pulpitis and thus, can be used as
a diagnostic test [3]. A number of variations of irreversible pulpitis
have been recognised. These include acute, subacute, chronic,
partial or total, infected or sterile, however it is not possible to
clearly differentiate these clinically and can be differentiated only
by histopathological methods [4].
Pulp vitality plays an important role in routine dental practice [5].
Pulp vitality tests are the valuable diagnostic tool which aids the
clinician towards the accurate diagnosis and appropriate treatment
planning. Diagnosing the exact pulpal status by direct examination
is uncertain due to the fact that the pulp is enclosed within
a hard tissue. In order to identify the actual pulp status surrogate
test must be performed [6]. Disease of the pulp can be infectious
or inflammatory. In such conditions, the healthy pulp attempts to
counteract the inflammatory response as a defence mechanism in
order to restore the integrity of the pulp [7]. Therefore, the presence
of blood flow within the pulp is a reliable indicator as it can
reflect the degree of pulpal disease. The tests which record the
blood flow within the pulp are termed as pulp vascularity tests as it is the only true indicator in assessing the actual pulp status [8].
Root canal therapy (RCT) and tooth extraction have been conventional
treatment options for management of human mature teeth
with irreversible pulpitis [9]. Root canal treatment in a common
procedure in dentistry. The main indications for RCT are irreversible
pulpitis and necrosis of dental pulp due to caries or dental
trauma [10].
Single visit treatment is an approach when in access opening,
cleaning and shaping with irrigation and obturation is done in a
single setting. Whereas multi visits but they are carried out in 3
to 4 appointments help to reduce chances of error and infection
[11]. Intracanal medicaments have been used to disinfect root canals
between appointments and reduce the interappointment pain
[12]. After root canal treatment, teeth can experience short/long
term complications. Short term complication includes postoperative
inflammation of periapical tissue leading to mild pain and
flare up, pain and swelling associated with instrumentation and
irrigation transporting medium [13]. Long term outcome includes
persisting inflammation and infection, resulting in abscess,since
track formation, periapical bone resorption [14].
Previously our team had conducted numerous clinical trials [15-
17], in vitro studies [18-21] and surveys [12, 22] and reviewed [10,
23-27]. Various aspects of endodontics and conservative dentistry
over the past five years. Now we are focusing on retrospective
studies, the idea for which has stemmed from the current interest
in our community. The aim of this study was to find out the
association of irreversible pulpitis and single visit root canal treatment.
A retrospective study was carried out in patients who visited University
in Chennai with irreversible pulpitis and underwent single
visit root canal treatment. The data were collected from patients
records between June 2019-March 2020. The data contains details
of patients, intraoral photographs and treatment being done.
● Patients with irreversible pulpitis
● Patients undergoing root canal treatment
● Above 17 years
● Patient with reversible pulpitis
● Patients with periradicular disease
● Pulp necrosis
Sample size [N=2329] is the total number of patients who visit
University in Chennai with irreversible pulpitis and underwent
single visit root canal treatment. Their distribution according to
age,gender, teeth number were recorded.
Ethical clearance was obtained from the Institutional Ethical
Committee and Scientific Review Board [SRB] of University in
Chennai.
The data collected were entered in an Excel sheet and subjected
to statistical analysis using SPSS software. Descriptive statistics
was done i.e frequency and cross tabulation. A chi square test was
done between age and teeth number, gender and teeth number.
Mean and standard deviation was done for age and gender. Independent
variables are age and gender while dependent variables
are teeth number. The level of significance was p<0.05.
Results And Discussion
A total of 5366 patients were diagnosed with irreversible pulpitis,
among which 2329 patients underwent single visit RCT (43.40%)
and 3037 patients had undergone multi visit RCT (56.60%) [Figure
1]. Among 2329 patients 1182 were females (50.73%) and
1147 were males (49.27%) [Figure 2]. Females (22.03%) mostly
underwent single visit root canal treatment when compared to
males [21.38%] and Male (30.62%) patients mostly underwent
multiple visit root canal treatment when compared to female
patients (25.98%) which was found to be statistically significant
[Figure 3, Table 1]. Most number of single visit RCT (19.47%)
and multi visit RCT (34.87%) are seen in the age group of 18-38
years and were found to be statistically significant [Figure 4 Table
2]. Single visit RCT was higher in maxillary first molar followed
by maxillary central incisors while multi visit RCT was higher in
mandibular first molars followed by maxillary first molars which
was found to be statistically significant [Figure 5, Table 3].
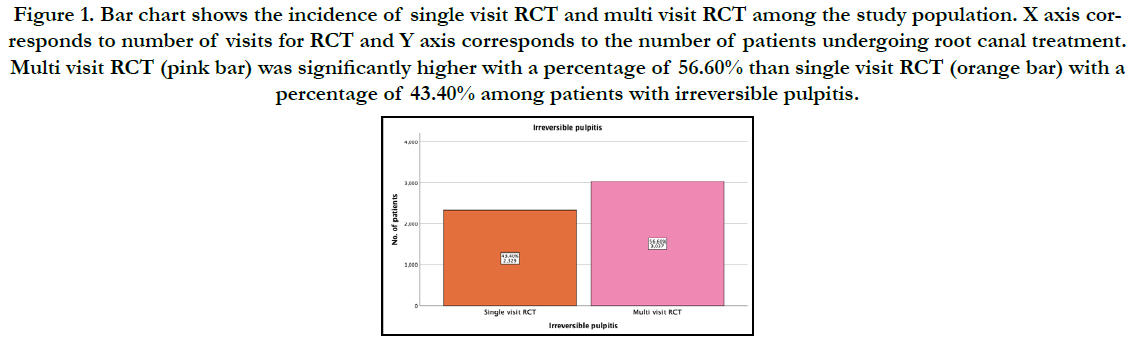
Figure 1. Bar chart shows the incidence of single visit RCT and multi visit RCT among the study population. X axis corresponds to number of visits for RCT and Y axis corresponds to the number of patients undergoing root canal treatment. Multi visit RCT (pink bar) was significantly higher with a percentage of 56.60% than single visit RCT (orange bar) with a percentage of 43.40% among patients with irreversible pulpitis.
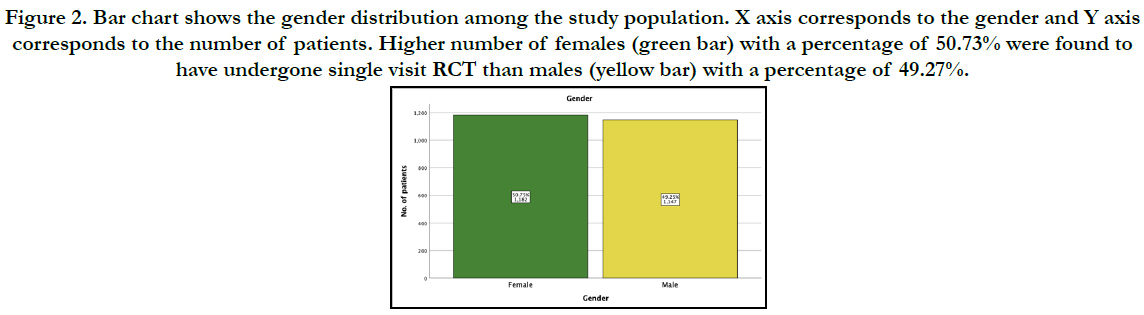
Figure 2. Bar chart shows the gender distribution among the study population. X axis corresponds to the gender and Y axis corresponds to the number of patients. Higher number of females (green bar) with a percentage of 50.73% were found to have undergone single visit RCT than males (yellow bar) with a percentage of 49.27%.
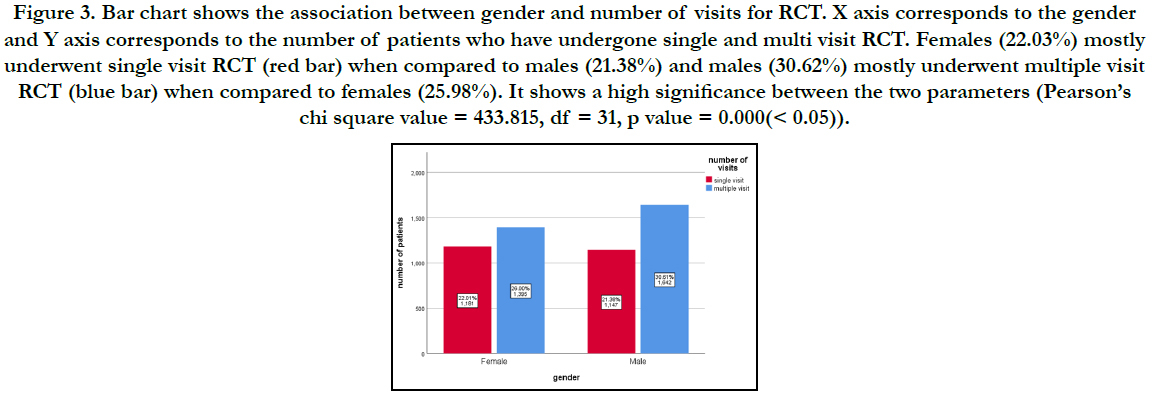
Figure 3. Bar chart shows the association between gender and number of visits for RCT. X axis corresponds to the gender and Y axis corresponds to the number of patients who have undergone single and multi visit RCT. Females (22.03%) mostly underwent single visit RCT (red bar) when compared to males (21.38%) and males (30.62%) mostly underwent multiple visit RCT (blue bar) when compared to females (25.98%). It shows a high significance between the two parameters (Pearson’s chi square value = 433.815, df = 31, p value = 0.000(< 0.05)).
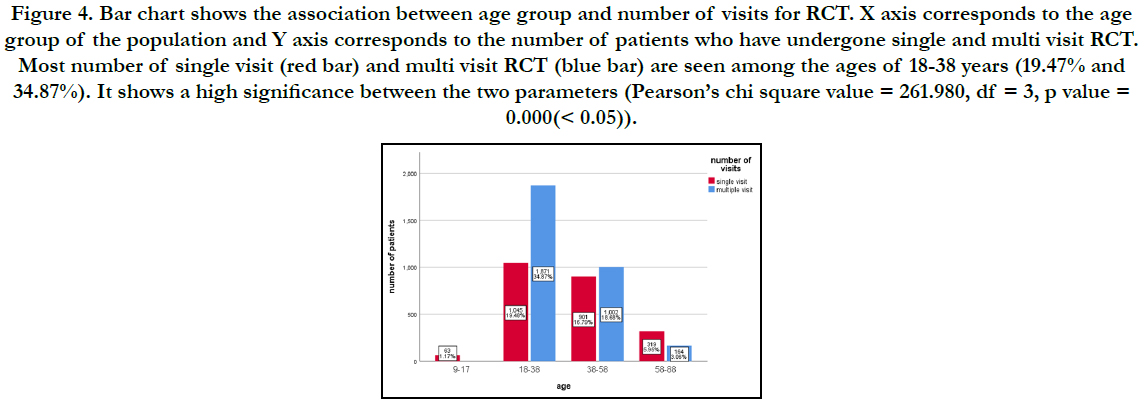
Figure 4. Bar chart shows the association between age group and number of visits for RCT. X axis corresponds to the age group of the population and Y axis corresponds to the number of patients who have undergone single and multi visit RCT. Most number of single visit (red bar) and multi visit RCT (blue bar) are seen among the ages of 18-38 years (19.47% and 34.87%). It shows a high significance between the two parameters (Pearson’s chi square value = 261.980, df = 3, p value = 0.000(< 0.05)).
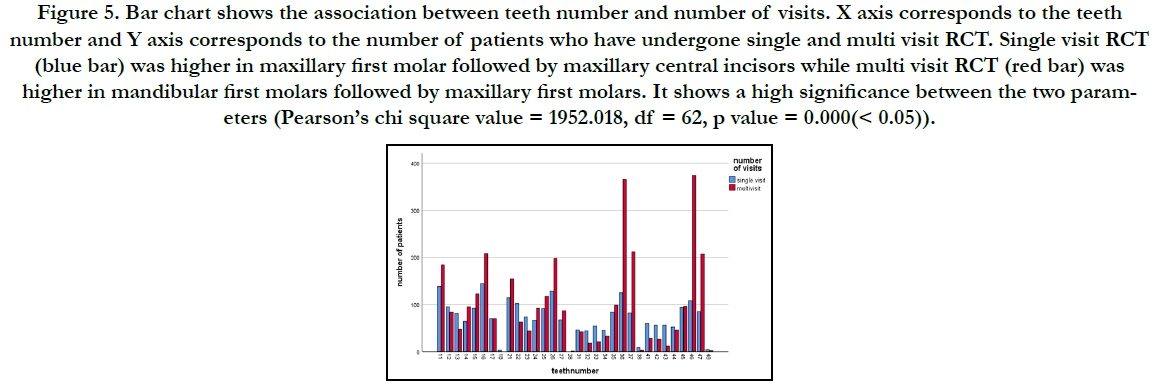
Figure 5. Bar chart shows the association between teeth number and number of visits. X axis corresponds to the teeth number and Y axis corresponds to the number of patients who have undergone single and multi visit RCT. Single visit RCT (blue bar) was higher in maxillary first molar followed by maxillary central incisors while multi visit RCT (red bar) was higher in mandibular first molars followed by maxillary first molars. It shows a high significance between the two parameters (Pearson’s chi square value = 1952.018, df = 62, p value = 0.000(< 0.05)).
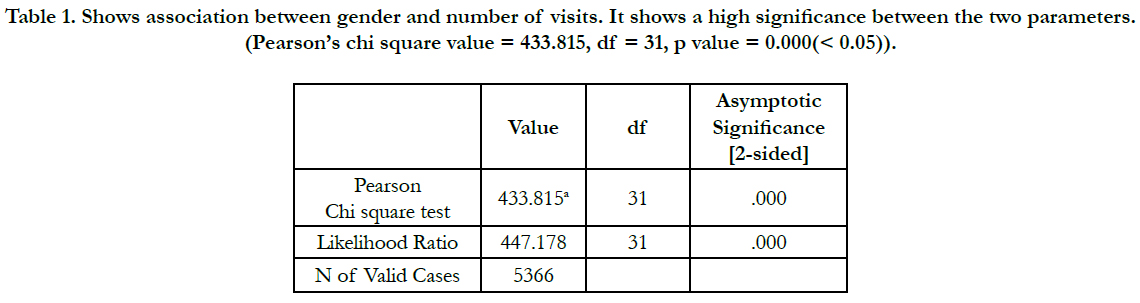

Table 1. Shows association between gender and number of visits. It shows a high significance between the two parameters. (Pearson’s chi square value = 433.815, df = 31, p value = 0.000(< 0.05)).
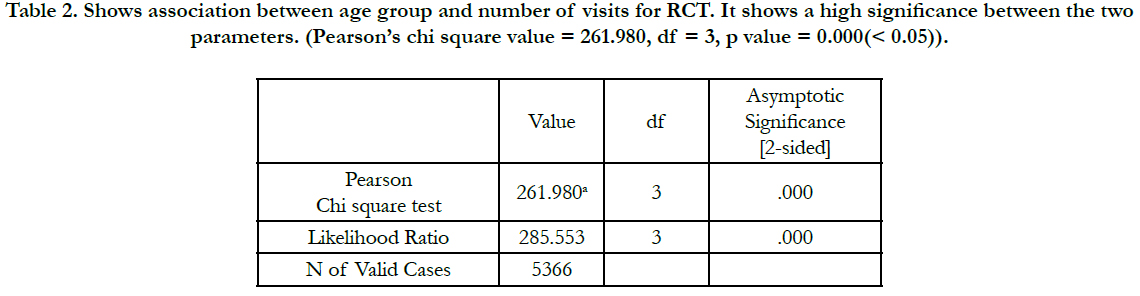
Table 2. Shows association between age group and number of visits for RCT. It shows a high significance between the two parameters. (Pearson’s chi square value = 261.980, df = 3, p value = 0.000(< 0.05)).
Table 3. Shows association between teeth number and number of visits for RCT. It shows a high significance between the two parameters. (Pearson’s chi square value = 1952.018, df = 62, p value = 0.000(< 0.05)).
The current study shows that the incidence of single visit RCT was among 43.40% of the population. There was no previous literature showing the incidence of single and multi visit RCT but did show the postoperative complication of both [28].
A study by R.B Pekruhn et al,shows that failure rates in single visit RCT was 5.2% [29]. Another study by Lara figini et al states that patients undergoing single visit RCT showed higher rates of swelling [30]. According to Wai-lee yong et al, the success rate of single and multi visit endodontic treatments had no significance difference [31]. This was also supported by Wong A W et al,who stated that postoperative complications of single visit and multiple visit RCT were similar [32]. A study done by Alomaym et al concludes that less incidence of pain in multi visit root canal treatment than single visit group,which is statistically significant [33]. A study done by Adbel Hameed et al., concludes that no significant difference exists in post operative pain after single visit or multi visit root canal treatment [34]. The limitation of this study is that it was confined to a specific population and geographic location. The future scope of this study is to compare the prognosis and failure rates of single visit and multi visit RCT and to conduct the study among a larger population.
Conclusion
Within the limitation of this study, it can be concluded that female
patients were highly diagnosed with irreversible pulpitis and
underwent single visit root canal treatment. More number of single
visit root canal treatments were seen in the 18-38 age group.
Maxillary first molar and maxillary central incisors are frequently
affected with irreversible pulpitis underwent single visit RCT. Female
patients underwent more number of single visit root canal
treatments when compared to male patients. Although multi visit
RCT is considered the conventional technique, single visit takes
less time, is cost effective, prevents RC contamination bacterial
regrowth, less stressful to patients regarding anesthesia and instrumentation
related to treatment; and studies have shown that
success rates are similar in both techniques.
Author Contributions
All authors have equal contributions in bringing out this research
work.
Acknowledgement
This study was supported by Saveetha Dental College and Hospitals,
Chennai.
References
- Agnihotry A, Thompson W, Fedorowicz Z, van Zuuren EJ, Sprakel J. Antibiotic use for irreversible pulpitis. Cochrane Database Syst Rev. 2019 May 30; 5(5): CD004969. PMID: 31145805.
- Soames JV, Southam JC. Oral Pathology (3rd Edtn). Oxford: Oxford University Press. 1998; 51-70.
- Cecic PA, Hartwell GR, Bellizzi R. Cold as a diagnostic aid in cases of irreversible pulpitis. Report of two cases. Oral Surg Oral Med Oral Pathol. 1983 Dec; 56(6): 647-50. PMID: 6581463.
- Cohen S, Burns RC, Walton R, Torabenijad M. Pathways of the Pulp (1). Learning. 1998; 30: 10.
- Gopi Krishna V, Kandaswamy D, Gupta T. Assessment of the efficacy of an indigeniously developed pulse oximeter dental sensor holder for pulp vitality testing. Indian J Dent Res. 2006 Jul-Sep;17(3):111-3. PMID: 17176825.
- Levin LG. Pulp and periradicular testing. J Endod. 2013 Mar; 39(3 Suppl):S13-9. PMID: 23439039.
- Baumgardner KR, Walton RE, Osborne JW, Born JL. Induced hypoxia in rat pulp and periapex demonstrated by 3H-misonidazole retention. J Dent Res. 1996 Oct;75(10):1753-60. PMID: 8955670.
- Calil E, Caldeira CL, Gavini G, Lemos EM. Determination of pulp vitality in vivo with pulse oximetry. Int Endod J. 2008 Sep;41(9):741-6. PMID: 18554185.
- Asgary S, Eghbal MJ, Ghoddusi J, Yazdani S. One-year results of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter, randomized, non-inferiority clinical trial. Clin Oral Investig. 2013 Mar;17(2):431-9. PMID: 22431145.
- Rajakeerthi R, Ms N. Natural Product as the Storage medium for an avulsed tooth–A Systematic Review. Cumhuriyet Dental Journal. 2019; 22(2):249- 56.
- Peters LB, Wesselink PR. Periapical healing of endodontically treated teeth in one and two visits obturated in the presence or absence of detectable microorganisms. Int Endod J. 2002 Aug;35(8):660-7. PMID: 12196219.
- Manohar MP, Sharma S. A survey of the knowledge, attitude, and awareness about the principal choice of intracanal medicaments among the general dental practitioners and nonendodontic specialists. Indian J Dent Res. 2018 Nov-Dec; 29(6):716-720. PMID: 30588997.
- Glennon JP, Ng YL, Setchell DJ, Gulabivala K. Prevalence of and factors affecting postpreparation pain in patients undergoing two-visit root canal treatment. Int Endod J. 2004 Jan;37(1):29-37. PMID: 14718054.
- Manfredi M, Figini L, Gagliani M, Lodi G. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev. 2016 Dec 1;12(12):CD005296. PMID: 27905673.
- Janani K, Palanivelu A, Sandhya R. Diagnostic accuracy of dental pulse oximeter with customized sensor holder, thermal test and electric pulp test for the evaluation of pulp vitality: an in vivo study. Brazilian Dental Science. 2020 Jan 31;23(1):8-p.
- Ramamoorthi S, Nivedhitha MS, Divyanand MJ. Comparative evaluation of postoperative pain after using endodontic needle and EndoActivator during root canal irrigation: A randomised controlled trial. Aust Endod J. 2015 Aug;41(2):78-87. PMID: 25195661.
- Hussainy SN, Nasim I, Thomas T, Ranjan M. Clinical performance of resinmodified glass ionomer cement, flowable composite, and polyacid-modified resin composite in noncarious cervical lesions: One-year follow-up. J Conserv Dent. 2018 Sep-Oct;21(5):510-515. PMID: 30294112.
- Nandakumar M, Nasim I. Comparative evaluation of grape seed and cranberry extracts in preventing enamel erosion: An optical emission spectrometric analysis. J Conserv Dent. 2018 Sep-Oct;21(5):516-520. PMID: 30294113.
- Ramanathan S, Solete P. Cone-beam Computed Tomography Evaluation of Root Canal Preparation using Various Rotary Instruments: An in vitro Study. J Contemp Dent Pract. 2015 Nov 1;16(11):869-72. PMID: 26718293.
- Teja KV, Ramesh S, Priya V. Regulation of matrix metalloproteinase-3 gene expression in inflammation: A molecular study. J Conserv Dent. 2018 Nov- Dec;21(6):592-596. PMID: 30546201.
- Manoharan V, Kumar RK, Sivanraj AK, Arumugam SB. Comparative Evaluation of Remineralization Potential of Casein Phosphopeptide- Amorphous Calcium Fluoride Phosphate and Novamin on Artificially Demineralized Human Enamel: An In vitro Study. Contemp Clin Dent. 2018 Jun; 9(Suppl 1): S58-S63. PMID: 29962765.
- Jose J, Subbaiyan H. Different Treatment Modalities followed by Dental Practitioners for Ellis Class 2 Fracture–A Questionnaire-based Survey. The Open Dentistry Journal. 2020 Feb 18;14(1).
- Shenoy A, Bolla N; Sayish, Sarath RK, Ram CH; Sumlatha. Assessment of precipitate formation on interaction of irrigants used in different combinations: an in vitro study. Indian J Dent Res. 2013 Jul-Aug;24(4):451-5. PMID: 24047837.
- Teja KV, Ramesh S. Shape optimal and clean more. Saudi Endodontic Journal. 2019 Sep 1;9(3):235.
- Kumar D, Antony S. Calcified Canal and Negotiation-A Review. Research Journal of Pharmacy and Technology. 2018;11(8):3727-30.
- Noor S. Chlorhexidine: Its properties and effects. Research Journal of Pharmacy and Technology. 2016;9(10):1755-60.
- Ravinthar K. Recent advancements in laminates and veneers in dentistry. Research Journal of Pharmacy and Technology. 2018;11(2):785-7.
- Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature -- Part 2. Influence of clinical factors. Int Endod J. 2008 Jan;41(1):6-31. PMID: 17931388.
- Singh S, Garg A. Incidence of post-operative pain after single visit and multiple visit root canal treatment: A randomized controlled trial. J Conserv Dent. 2012 Oct;15(4):323-7. PMID: 23112477.
- Sathorn C, Parashos P, Messer H. Australian endodontists' perceptions of single and multiple visit root canal treatment. Int Endod J. 2009 Sep;42(9):811-8. PMID: 19619228.
- Pekruhn RB. The incidence of failure following single-visit endodontic therapy. J Endod. 1986 Feb;12(2):68-72. PMID: 3457093.
- Manfredi M, Figini L, Gagliani M, Lodi G. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev. 2016 Dec 1;12(12):CD005296. PMID: 27905673.
- Alomaym MAA, Aldohan MFM, Alharbi MJ, Alharbi NA. Single versus Multiple Sitting Endodontic Treatment: Incidence of Postoperative Pain - A Randomized Controlled Trial. J Int Soc Prev Community Dent. 2019 Mar- Apr;9(2):172-177. PMID: 31058068.
- El Mubarak AH, Abu-bakr NH, Ibrahim YE. Postoperative pain in multiplevisit and single-visit root canal treatment. J Endod. 2010 Jan;36(1):36-9. PMID: 20003932.





