Association of Handedness and Maximum Voluntary Bite Force on Respective Side of Oral Cavity
Danish Altaf1*, Muhammad Sohaib Nawaz2, Muhammad Hassan3, Arooj ul Hassan4, Muhammad Haseeb5, Aqil Malik6
1 Post graduate resident, Department of Prosthodontics, University college of Medicine and Dentistry, University of Lahore, Pakistan.
2,6 Assistant Professor, Department of Prosthodontics, University college of Medicine and Dentistry, University of Lahore, Pakistan.
3 Assistant Professor, Department of Dental Materials, University college of Medicine and Dentistry, University of Lahore, Pakistan.
4 Assistant Professor, Department of Community and Preventive Dentistry, University college of Medicine and Dentistry, University of Lahore, Pakistan.
5, Assistant Professor, Department of Periodontology, University college of Medicine and Dentistry, University of Lahore, Pakistan.
*Corresponding Author
Danish Altaf,
Postgraduate Resident, Department of Prosthodontics, University college of Medicine and Dentistry, University of Lahore, Pakistan.
Tel: +923214488555
E-mail: danishaltaf91@gmail.com
Received: September 21, 2020; Accepted: October 02, 2020; Published: November 08, 2020
Citation:Danish Altaf, Muhammad Sohaib Nawaz, Muhammad Hassan, Arooj ul Hassan, Muhammad Haseeb, Aqil Malik. Association of Handedness and Maximum Voluntary Bite Force on Respective Side of Oral Cavity. Int J Dentistry Oral Sci. 2020;7(11):972-975. doi: dx.doi.org/10.19070/2377-8075-20000193
Copyright: Danish Altaf©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: The aim of the study was to explore the difference between handedness and bite force among general population.
Method: Bite force was recorded with an Occlusal Bite force meter (GM-10 Nagano Keiki Japan). A mean of three left sided and
a mean of three right sided maximum voluntary bite forces were calculated and a final mean of the two were taken to find out the
Mean Maximum Voluntary Bite force. The data was entered and analyzed in SPSS version 25.0. As descriptive statistics, percentage
of gender distribution was calculated. Later on, Paired sample t test and independent sample t test was used to explore the bite
force difference among right and left handed participants.
Results: Paired sample t test used to calculate between group difference of Bite Force which was found to be significant (t= 2.895,
P=.005). The results of independent sample t test revealed a significant difference between the handedness and the average force
bite from left side of mouth (t (2, 68) = -3.08, P=.003). The results for the comparison of average bite force from right side of
mouth and handedness was also found significant (t (2, 68) = 2.36, P=.02).
Conclusion: The study explored the difference of handedness with the bite force which was found to be significant. The results
explained that right handed people have higher bite force at right side of mouth on chewing whereas left handed people apply
more force while biting with left side of mouth as compared to right side. This was the new finding explored by performing this
study.
2.Material and Methods
3.Results
4.Discussion
5.Conclusion
6.Refereces
Introduction
For language, the major imperative behavioral irregularity is handedness
because of its close relationship with the brain specialization.
Handedness can be seen in 3 levels, i-e., right handedness,
left handedness and both right and left handedness (mixed). The
primary minority group categorized around the globe is the group
of Left-handers and at several times they face disadvantaged situations
due to left handedness paralleled to right handers. Numerous
studies demonstrated association between left-handedness
and different health problems ranging from learning disorders to
breast cancer and decreased longevity. This paper is based on the
concept that there might be some difference between the handedness
and bite force.
Dissemination of handedness in a populace possess structures of
directional irregularity in which non-racemic combination of two
kinds of laterality is present [1]. In human around the globe, there
is a Harmonious inclination for preferring the right hand as the
prevalence of left handed people is around 10% of population in
most of the cultures [1-4]. It is suggested from this fact that the
change to the right has been determined on general preconception
towards right hand as compared to unintentional inclination
towards left hand [1, 2]. Numerous authors proposed that the
evolution of right-handedness is based on convenience of using
right hand for various activities as carrying and soothing of a baby
or for eating food [5, 6].
Occlusal Bite force is the interocclusal force that is produced
when the jaw is closed under the effect of jaw muscles as a result
of the coordination between different components of the
masticatory system i.e. muscles, bones and teeth [1]. Occlusal bite
force is frequently used to evaluate masticatory function because
it reflects the maximum voluntary contraction of the masticatory
muscles [2]. Masticatory muscles more importantly Masseter,
Temporalis and Medial Pterygoid plays an important role in the closure of the jaw. Maximum voluntary bite force (MVBF) is the
capacity of the mandibular elevator muscles to perform a maximum
strain of mandibular teeth against the maxillary teeth1-3.
MVBF magnitude is influenced by age, gender, face form, occlusion,
periodontal and gingival problems, missing teeth, pulp related
problem, jaw muscle cross-sectional area, craniofacial morphology
and temporomandibular disorders [1, 4-6].
At its peak level, Maximum Bite Force was recorded in first molar
region [7]. Among healthy adults with natural teeth, the unilateral
MVBF measurements in the molar region averages between 300N
to 600N [8]. The average bite force in males from 13 to 40 years
is 374. ± 30.75 N and average bite force in females of age 13 to
40 years is 257 ± 31 N [8]. The mean bite force at this age is 315.5
± 30.87N [8]. The average increase in the rate of bite force on
the permanent molars in children has been reported to be 23 N
per year from 7 years to early twenties. All correlations between
MVBF and age reduces between 26 and 41 year and then forces
decrease after the age of 45 years [8]. Generally there has been a
gradual decrease in average bite force with the time. Discrepancies
in relation to the maximum bite force were found on regional
bases, that white western population have less average bite force
than Eastern population which in turn have less average bite force
than Black African [8]. The rural area people generally have higher
average bite force than urban area [7]. Food choice is one of the
major known cause of these differences at regional levels. Soft
food consumption resulting in lesser average bite force [7]. There
are numerous study available on average bite force, but no literature
was cited related to the relationship between the left, or right
handedness with the side of molar region with higher average
force bite. The aim of the study was to explore the difference
between handedness and bite force among general population.
Material and Methods
This quantitative study was of crossectional in nature. The research
was approved by the Ethics Committee of the Fatima
Memorial College of Medicine and Dentistry Lahore. Sample size
was estimated as 72 subjects. Both genders were included in the
study. The subjects signed an informed consent to participate in
the study before data collection.
The subjects had a neutral occlusion (Class I molar relationship)
with balanced facial profiles, a symmetric appearance in the frontal
view, harmoniously shaped competent lips, and absence of
previous orthodontic treatment. They had normal healthy teeth
(intraoral examination reveal no caries, mobility, periodontitis
or any pulp related pathology) and a full natural complement of
teeth from 2nd molar to 2nd molar both in maxilla and mandible.
None of the subjects had craniofacial anomalies or systemic muscle
or joint disorders. Morphological examination verified the
neutral occlusal relationship (both canines and molars were Angle
Class I), the presence of all permanent teeth, except third molars,
and the absence of any dental malocclusion, even minor rotations.
The evaluation of inclusion criteria for each subject was
conducted by a Prosthodontist using a mouth mirror and artificial
lighting.
The instrument used for measuring bite force in a portable occlusal
force gauge (GM10; Nagano Keiki, Tokyo, Japan). The
instrument consisted of a hydraulic pressure gauge and a biting
element (17 mm in width and 5.4 mm in height) made of a vinyl
material encased in a disposable plastic tube (Figure 1, 2).
Each tube was used for one person after whom the device was
cleaned with a cloth moistened with alcohol. The measuring range
of the instrument was from 0 to 1000 N with an accuracy of ±1
N. Bite force was displayed digitally. All measurements were made
with the subjects seated with back unsupported, looking forward
and head in unsupported natural position (Figure 3).
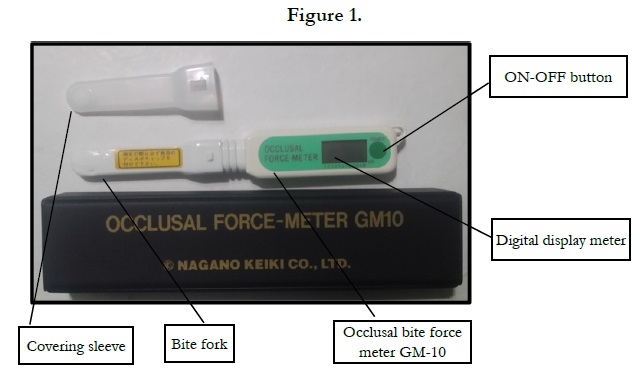
Figure 1.
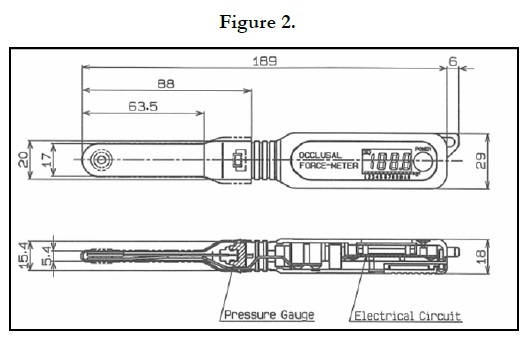
Figure 2.
Figure 3.
Measurements of MVBF were undertaken during a single session for each subject, using the instrument. It was measured unilaterally on both the left and right sides of the jaw in the 2nd pre molar and first molar region. The maximum bite force was measured three times on each side with an interval of minimum 3 minutes. Mean of each side was recorded separately and later an average of both the means were taken to record MVBF. None of the subjects experienced any discomfort or pain during biting on the instrument.Data was entered in SPSS version 25.0 and independent sample t test was used to analyze the effect of handedness on the average force bite.
Results
Gender was taken as demographic variable. Males were 47.2%
whereas females were 52.8% of the entire sample. Paired sample
t test used to calculate between group difference of Bite Force
which was found to be significant (t = 2.895, P=.005). The mean
score of Bite force from right side of the mouth was 593.569 ± 136.587 whereas Bite force from right side of the mouth mean
score was 518.416 ± 161.475.
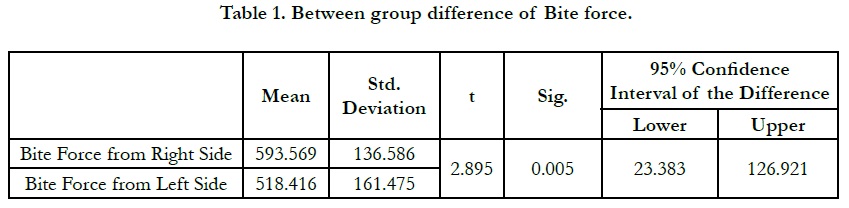

Table 1. Between group difference of Bite force.
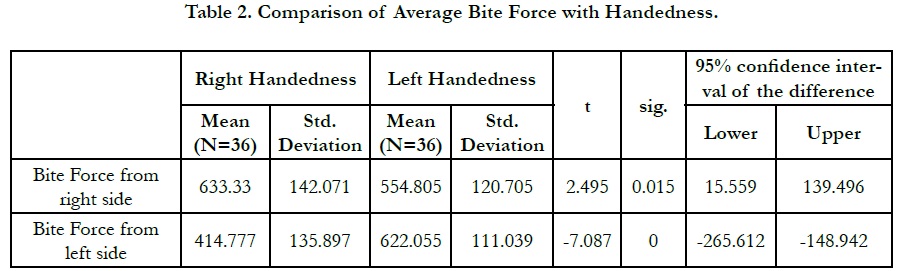
Table 2. Comparison of Average Bite Force with Handedness.
The results of independent sample t test revealed a significant difference between the handedness and the average force bite from left side of mouth (t (2, 68) = -3.08, P =.003). The mean value of average bite force of left side of mouth for right handed participants was 498.25 ± 171.90 which was found to be less as compared to the mean value of average bite force of left side of mouth for left handed participants 614.49 ± 143.54.
Moreover, the results for the comparison of average bite force from right side of mouth and handedness was also found significant (t (2, 68) = 2.36, P = .02). The mean value of average bite force of right side of mouth for right handed participants was 601.57 ± 171.09 which was found to be greater than the mean value of average bite force of right side of mouth for left handed participants 503.28 ± 179.03.
Discussion
This study aimed to determine mean maximum bite force in a
healthy population with normal occlusion. The study explored the
difference of handedness with the bite force which was found
to be significant. The results explained that right handed people
have higher bite force at right side of mouth on chewing whereas left handed people apply more force while biting with left side of
mouth as compared to right side.
Bite force is a complex outcome of multiple factors [1-4, 13, 18, 19]
therefore bite force is a unique feature of every human which
varies from person to person and age to age. NO two studies
till date have reported exactly same bite force values. The disparity
between different studies is from 189 ± 78 N by Sasaki et al
2019, 89 to 720 N by Gibbs et al in 1981. Gibbs et al [21] in 1986
discovered one individual who had a biting force of 4340 N (443
kg). This disparity in the bite force in this study and all the previous
studies can be due to various intra human and inter human
reasons one of them may the global variation of food preference,
food availability, human races environmental factors and human
development environment.
The bite force calculated in this study is lower than Sathyanarayana
H P, Sridhar Premkumar S 22 with Adults (17-25years) who
had a mean MVBF of 601.83 N with males having a value of
650.67 N and females it was 543 N. Similarly, with the results of
the study done by Bonakdarchian M, Askari N Askari M 4 on a
sample of 40 subjects with normal dentition with age range from
19 - 27 years the Mean MVBF is 631.12 N ± 235 N.
The main reason of MVBF calculated in this study being less
than that of few other studies may be attributed to the age group
taken. In this study the age range is 13 - 40 while in above mentioned
other studies the age range is smaller. Relatively younger
age group is taken which have been proven to have higher average
bite force values than older adults [1, 2, 8-13].
The MVBF calculated in this study is greater thanPalinkasM et
al2 , according to this study average MVBF in age 13-20 years
MVBF is 341.5 N ± 27, from age 21-30 years MVBF is 288.5 N ±
24.5, from age 31-40 years MVBF is 264 N ± 21.5. According to,
Al- Saadi D K and , Al - Mulla A A 9, in Iraqi people the MVBF
is 392.81 N ± 54.7. The studies [2, 13] with lesser bite force than
this study are based on the Brazilian, Iraqi respectively and the
studies [4, 12] with higher bite force than this study are in based on
Irani and Indian population. The results are more comparable to
studies [4,12] the reason may be the regional variation as per HallakRegalo
S C et al 7 the type of food being consumed in one
particular region [1, 2, 7].
Conclusion
The study explored the difference of handedness with the bite
force which was found to be significant. The results explained
that right handed people have higher bite force at right side of
mouth on chewing whereas left handed people apply more force
while biting with left side of mouth as compared to right side.
This was the new finding explored by performing this study.
References
- Ikebe K, Matsuda K, Kagawa R, Enoki K, Yoshida M, Maeda Y, et al. Association of masticatory performance with age, gender, number of teeth, occlusal force and salivary flow in Japanese older adults: is ageing a risk factor for masticatory dysfunction? Arch Oral Biol. 2011 Oct;56(10):991-6. Pubmed PMID: 21529776.
- PalinkasM,Nassar MSP, Cecı´lio FA, Sie´ssere S, SempriniM,c, Machadode- Sousa JP, et al. Age and gender influence on maximal bite force and masticatory muscles thickness, Arch Oral Biol2010;55:797-802. Pubmed PMID: 20667521.
- Bakke M. Bite force and occlusion. InSeminars in orthodontics.WB Saunders.. 2006;12:120-6.
- Bonakdarchian M, Askari N, Askari M. Effect of face form on maximal molar bite force with natural dentition. Arch Oral Biol. 2009 Mar;54(3):201-4. Pubmed PMID: 19131047.
- Al-Drees AM. Oral and perioral physiological changes with ageing. Pakistan oral & dental journal. 2010 Jun 1;30(1).
- Bokhari SA, Khan AA, Ansari JA, Alam R. Tooth loss in institutionalized coronary heart disease patients of Punjab Institute of Cardiology, Lahore, Pakistan. J Epidemiol Glob Health. 2012 Mar;2(1):51-6. Pubmed PMID: 23856398.
- Regalo SCH, Santos CM, Vitti M, Regalo CA, Vasconcelos PB, MestrinerJr W, et al. Evaluation of molar and incisor bite force in indigenous compared with white population in Brazil. arch oral biol 2008;53:282-6.Pubmed PMID:18031710.
- Varga S, Spalj S, Varga ML, Milosevic SA, Mestrovic S, Slaj M. Maximum voluntary molar bite force in subjects with normal occlusion. Eur J Orthod 2011; 33:427-433.Pubmed PMID:21062965.
- Al-Saadi D K and , Al – Mulla A A. Digitalized measurement of maximum bite force in Iraqi adult sample aged 18 – 25 years with different malocclusion groups.J BaghColl Dentistry 2011; 23(sp. issue):146-150.
- Sakaguchi M, Ono N, Turuta H, Yoshiike J, Ohhashi T. Development of new handy type occlusal force gauge. Japanese journal of medical electronics and biological engineering 1996; 34: 53-5.
- Paphangkorakit J, Osborn JW. Effect on human maximum occlusal force of biting on a softer or harder object. Arch Oral Biol 1998;43:833–9.Pubmed PMID: 9821506.
- Van Der Bilt A, Tekamp FA, Van Der Glas HW, Abbink JH. Bite force and electromyograpy during maximum unilateral and bilateral clenching. Eur J Oral Sci. 2008;116:217-222. Pubmed PMID:18471239.
- Koc D, Dogan A, Bek B. Bite Force and Influential Factors on Bite Force Measurements: A Literature Review. Eur J Dent. 2010;4:223-232.Pubmed PMID:20396457.
- Manns A, Miralles R, Palazzi C. EMG, occlusal force and elongation of the masseter muscle under isometric voluntary contractions and variations of vertical dimension. J Prosthet Dent 1979;42:674–82. Pubmed PMID: 292779.
- Paphangkorakit J, Osborn JW. Effect of jaw opening on the direction and magnitude of human incisal occlusal forces. JDent Res 1997;76:561–7. Pubmed PMID:9042078.
- Nawaz MS, Yazdanie N, Faheemuddin M. Rehabilitation of a cystic mixed dentition mandible following marsupialization with a multipurpose acrylic splint acting as a space maintainer and an obturator. J Ayub Med Coll 2011;23(2):177-179.Pubmed PMID: 24800375.
- Ming Su C Yang Y, Hsieh T. Relationship between oral status and maximum bite force in preschool children. J Dent Sci 2009;4(1):32−39.
- Gonçalves TM, de Vasconcelos LM, da Silva WJ, Del Bel Cury AA, Garcia RC. Influence of female hormonal fluctuation on maximum occlusal force. Braz Dent J. 2011;22(6):497-501.Pubmed PMID: 22189646.
- Pereira LJ, Gavião MB, Bonjardim LR, Castelo PM, van der Bilt A. Muscle thickness, bite force, and craniofacial dimensions in adolescents with signs and symptoms of temporomandibular dysfunction. Eur J Orthod. 2007 Feb;29(1):72-8. Pubmed PMID: 17290018.
- Sasaki K, Hannam A G, Wood WW. Relationships between the size, position, and angulation of human jaw muscles and unilateral first molar bite force. J Den Research. 1989 Mar;68(3):499-503. Pubmed PMID: 2921394.
- Gibbs CH, Mahan PE, Mauderli A, Lundeen HC, Walsh EK.Limits of human bite strength. J Prosthet Dent.1986;56:226- 229. Pubmed PMID: 3463748.
- Sathyanarayana HP, Premkumar S. Assessment of maximum voluntary bite force in children and adults with normal occlusion. International Journal of Pharmacutical Science and Health Care. 2012;2:64-70.





