An Assessment of Occupational Stress, Job Satisfaction and Coping Strategies among Dentists in Damascus, Syria
Fatima KAlmasri*, Ali Al-sheikh Haidar
Oral Medicine Department, Faculty of Dental Medicine, Damascus, Syria.
*Corresponding Author
Fatima KAlmasria,
Oral Medicine Department, Faculty of Dental Medicine, Damascus, Syria.
Tel: +963969960118
E-mail: fatema.almasri92@gmail.com
Received: October 07, 2020; Accepted: November 06, 2020; Published: November 13, 2020
Citation:Fatima KAlmasri, Ali Al-sheikh Haidar. An Assessment of Occupational Stress, Job Satisfaction and Coping Strategies among Dentists in Damascus, Syria. Int J Dentistry Oral Sci. 2020;7(11):1017-1026. doi: dx.doi.org/10.19070/2377-8075-20000202
Copyright: Fatima KAlmasri©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Dentistry is understood to be a stressful profession.
Aims: (1) To distinguish grounds of stress can help preventing associated adverse effects. (2) To assess the association of various
personal and work related factors with general stress. (3) To evaluate the level of job satisfaction among dentists. (4) To explore
how job satisfaction among dentists is associated with various personal and work related factors. (5) To determine coping strategies
among Syrian dentists.
Methods: Non-randomized and cross-sectional survey had been accomplished between October 2018 to March 2019. The questionnaire
included modified version of the Occupational Stress, developed version of the dentist satisfaction survey. Besides, the
coping strategies were administered for 409 dentists.
Results: With response rate (82.8 %), 61.86% was reported being stressed. The most common cause of stress has maintained
high levels of concentration. Least frequent stressor wasTreatment of patient with maladaptive response to nervous functions.
The mean score of total careers of the respondents was 122.3. There is a medium-strong inverse correlation between scales of Job
stressors and Job satisfaction. Most common coping strategy was referred to the interactions with people.
Conclusions: Dentists are encouraged to implement extensively active coping strategies and participate in stress management
courses helping them in job satisfaction improvement.
2.Introduction
3.Material and Methods
4.Results
5.Discussion
6.Conclusions
7.Refereces
Keywords
Occupational Stress; Job Satisfaction; Coping Strategy; Dentist; Syria.
Introduction
Stress nowadays is a natural and unavoidable part of everyday
lifeand all people need a certain amount of stress, otherwise their
lives would be dull. Stress is responsible each year for the loss of
some 100 million working days; perhaps this is why the topic of
stressful work has attracted the attentions of many researchers
[1]. Seley [2] characterized stress as "the spice of life", although
too much stress may be damaging to body, some stress may be a
source of motivation if put under proper control. The long-term
exposure to stress can be a triggered for many psychosomatic
disorders [3], poor job performance, poor job satisfaction, poor
family, peer and coworker relations, as well as decreased life satisfaction
and general well‑being [4].
In recent years, Occupational stress has become an increasingly
serious problem around the world [5]. It is common within health
care professionals in the developed countries, although less is
known about its prevalence inMiddle Eastern countries [6]. Over
the years, studies have shown that experiencing stress in the work
setting leads to undesirable consequences on the well‑being and
safety of an individual and invariably for the organization [7].
Although dentists occupy an important position in the society,
dentistry has been considered one of the most stressful of all
healthcare professions [3]. The image of dentistry as being stressful
is part of the dental culture and tends to override the personal
experience due to the nature and working conditions as in the
dental surgery [8]. Job-related factors are almost explaining half
of the overall stress in a dentist’s life [9]. Levels of burnout (exhaustion)
are increasing [7], which appears to be related to deficits
in executive functioning or cognitive control [10]. Cross-sectional
studies had indicated that 10% of dentists experience high levels
of burnout [11].
Researchers from the BDA (Business Development Agreement) found high levels of stress and burnout amongst a survey of
more than 2,000 UK dentists where 17.6% admitted that they had
seriously thought about committing suicide [8].
Career satisfaction is a one central indicator of subjective career
success [12]. An American study used the dentist satisfaction survey
(DSS) [13], has investigated external or environmental factors
contributing to a job satisfaction, nonetheless, research involving
individual-level factors is relatively scarce. By focusing on intrapersonal
factors, we can be able to better explain why individuals in
similar work environments experience differing levels of satisfaction.
Cope is the constantly changing cognitive and behavioral efforts
to manage specific external and/or internal demands that
are appraised as taxing or exceeding the resources of the person
[14]. Coping strategies come under two broad classifications:
1- Adaptive: problem‑focused coping, long‑term, as past experience
- talking it out with others, are seen as constructive ways of
dealing with stress, and 2- Maladaptive: emotion‑focused coping
and short‑term as eating, sleeping, smoking, are reducing tension
temporarily, but do not deal directly with the stressful situation
[15]. Coping has been acknowledged as a mediator between encountered
stress and life adjustment outcomes [16].
Only meager number of surveys has been undertaken to assess
stress, satisfaction and cope behaviors of dentists. Thereon, the
current subject aimed to investigate sources of occupationalstress,
job satisfaction and coping strategies among them and then
tracking their relationship with the demographic characteristics
of dentists.
For this purpose, the following test tools were considered with
their reliability, validity and objectivity mentioned in their respective
manuals. The first section of the questionnaire collated-demographic
information, including gender, age, and social status,
specialty, years of experience, working hours per week, income
and number of patients treated per day. The second section consisted
of the modified version of the Occupational StressIndicator
(OSI) questionnaire devised by Cooper et al., [17] was used to
obtain information about job stressors. It consisted of 33 items
within the following seven scales: time pressures, financial stressors, patient-related stressors, staff problems, profession-related
stressors, and the nature of work and Fears from future.The response
options were as follows: ‘never’, ‘seldom’, ‘sometimes’,
‘often’ and ‘all the time’. Similar versions of this questionnaire
have been used widely in dental research [18]. The third section
comprised the DSS [19] instrument with minor modifications
made to reflect cultural uniqueness (i.e. spacing medical insurance
regimens, tradition, convention, education, illiteracy prevalence),
more appropriate for Syrian dentists. It consisted of 37 items:
Seven items to measure the factor of overall professional satisfaction
(OPS) and 30 items related to 10 work environment factors.
The supplementary material (SM) reproduces the DSS. Note
that negatively phrased items were incorporated into the survey
and are underlined in the SM. The work environment factors included:
Perception of staff, Income, Professional relations, Time
management, Stress, Patient relations, Personal time, Prudent
strategies, Respect, and Delivery of care. All items were measured
by a 5-point Likert scale: 1=Strongly Disagree, 2=Disagree,
3=Neither Agree nor Disagree, 4=Agree, and 5=Strongly Agree.
The last section consisted 10 strategies, was used for coping with
stress; Fig.S1
The paper has not investigated the correlations between the naturally-
occurring biological diseases (incl. oral) and the occupational
stress.
Inclusion criteria: This cross-sectional study took place between
October 2018 and March 2019 among dentists working in Damascus,
Syria, who had more than two years of work experience.
Exclusion criteria: A participant, who did not graduate from
Syrian university or complete the questionnaire.
Sample size: The sample was non-randomly selected (not randomized),
the questionnaire was posted with a covering letter
explaining the study’s purpose. 409 of dentists were invited to
participate in the study.
The sample size was estimated using G * Power (ver. 3.1.9.2, Universität
Kiel, Kiel, Germany), and the minimum sample size was
calculated for analysis using a chi-squared test. To obtain a 95%
confidence, and at least 5 percent-plus or minus-precision, this
gave Z values of 1.96, per the normal tables. Considering the internal
consistencies, the minimum required sample size for the objective of the study was calculated using the Cochran’s formula
for cross-sectional surveys, as follows:
n = t2P(1-P)/d2 = (1.96)2 × 0.70 × 0.30/(0.05)2 = 322
d: is the desired level of precision (i.e. the margin of error),
P: is the (estimated) proportion of the population which has the attribute in question, and
t: is the effect size that is given in the normal distribution table (z-table).
Therefore, the minimum sample size of surveys was 322 and the
final sample was 339, which fulfilled this statistical requirement.
The survey responses were entered into an electronic database
then the entry errors and outlier values were reviewed. Descriptive
statisticswere expressed as mean )μ), Standard deviation (SD)
andfrequency (ʋ). Further data screening was made to check all
variables for missing data, skewness and kurtosis. A student’s ttest
was used to compare the effects of variables. Associations between
categorical variables were tested for statistical significance
using the Chi-square test (χ2) [20]. P values were determined for
the continuous and categorical variables using the Mann-Whitney
U test and χ2 test, respectively. Cronbach Alpha coefficients of
the factors extracted in the analysis were identified to test the reliability
of the dimensions. The score of items for each factor were averaged to determine the degree of satisfaction. The average
scores of each factor were classified into three categories based
on the mean score in line with previous research [22]: dissatisfied
(1.0–2.5), neutral (>2.5–<3.5), and satisfied (3.5–5.0). (Table S1)
Total career score (TCS) was defined as a total score of all items.
All statistical analyses conducted using SPSS version 24 Independent
t-tests and analysis of variance (ANOVA), were implemented
to compare variables of demographic and practice characteristics.
Stepwise multiple regression analysis was used to identify predictors
or TCS and its related personal and professional characteristics,
p-values <0.05 were considered as having statistically significant
differences. The fallouts from the logistic regression were
expressed as 95% confidence intervals (CIs).
Results
Of the 409 dentists invited to participate in the study, 371 responded
(Males are the majority; Age distribution bands in decrement
sequence: ≤29, 30-39, 40-49, ≥50; Unmarried dentists and
General dentists were 124.4% that of Married and Specialists,
respectively; Years of expertise distribution bands in decrement
sequence: <10, 2–5, 6–10; Working (hr./wk.) bands in decrement
sequence: 21–40, <20, >40; Silent majority of Syrian dentists
monthly-pensions is ranged between $100-400; Preponderance
of treated patients: ʋ (<12); Total response rate (TRR): 82.8%;
Table 1) while 32 participants were excluded.
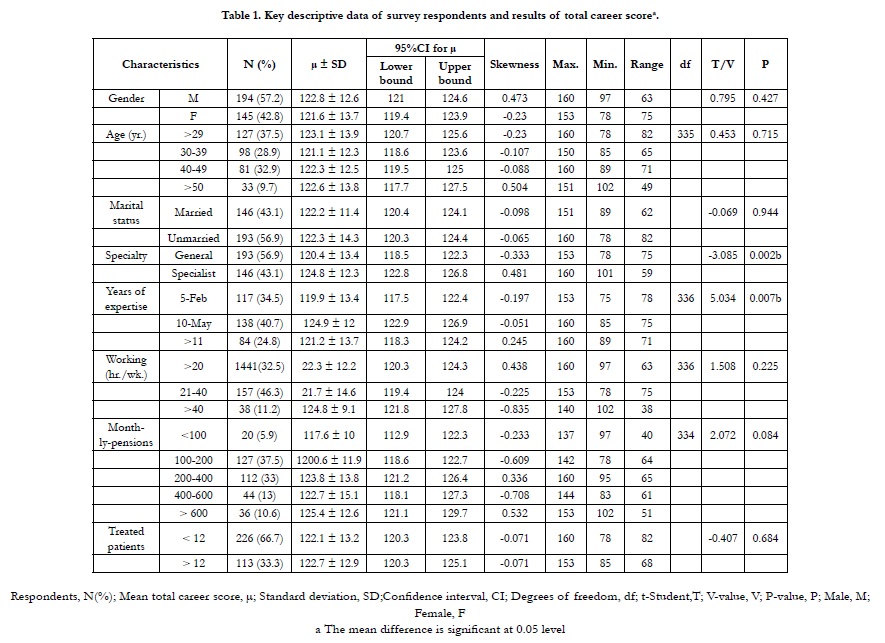

Table 1. Key descriptive data of survey respondents and results of total career scorea.
There was a considerable variation in the number of stressors that dentists experienced frequently or all thetime, with the number per dentistranging from 1 to 28. The frequency with which the various stressors were reported as occurring ‘very often’ or all the time (Table S2).
An Exploratory Factor Analysis method was used to determine the degree of correlation of the stressors in each section, 33 Stressors are summarized into seven sections using the Principal Component method, and variables branched were redistributed to the sections using the method of varimax, and these sections together contributed to explaining 61.05% of the total variance. (Table S3)
The quality of the factor analysis was significant .Also, using Bartlett's Test, this test is significant (χ 2 = 5974.2, p.value = 0.000 < 0.05) (Table S4). The most commonly reported stressors under the control management standard were Maintaining high levels of concentration, Time pressure (considering work schedule, time of work, and breaking time) and Repetitive nature of work. Work stress caused general stress response syndrome.
The least frequent stressors were Treatment of patient with maladaptive response to nervous functions, Feeling of devaluation from patient, and Packet of staff-based problems. 61.86% reported often being stressed (Table 2 and Table S5).
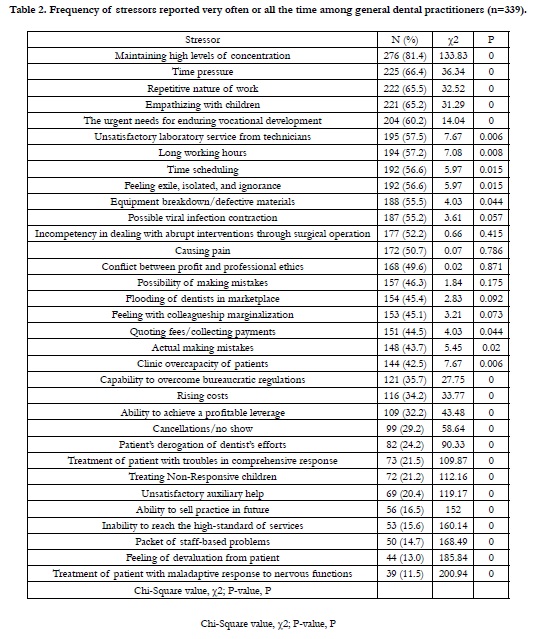
Table 2. Frequency of stressors reported very often or all the time among general dental practitioners (n=339).
Cronbach Alpha of Vocational stressor, Pressure stressor, Nature of work stressor, Financial stressor, OSI,Future stressor,Patientrelated stressor, Staff stressor are 0.935, 0.887, 0.858, 0.849, 0.712, 0.699, 0.673, 0.649, respectively andinternal consistency reliabilityof OSI (P-value: 0.000; All values were significant for α=0.05).(table S6)
The demographic characteristics of the participants and relationships with general stress are presented in Table 3. There was no significant relationship between general stress scores and gender (men have presented slightly higher job stress which was not significant with females), age, social status,years of experience, working hours per week, income, and number of patients treated per day. However, general stress showed a significant correlation with Specialty (P = 0.000). T-test showed that general dentists exhibited higher stress than specialist dentists, the mean difference was statistically significant (P = 0.00).
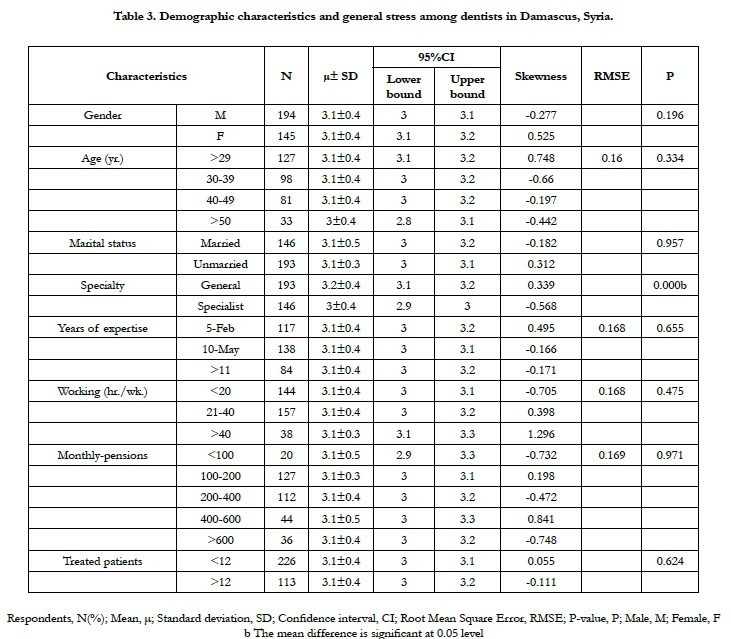
Table 3. Demographic characteristics and general stress among dentists in Damascus, Syria.
Cronbach’s alpha reliability coefficients for DSS is 0.805 and Internal consistency reliability for OPS is 0.8. (Table S7)
Table S8 depicts the average TCS. The top three highest mean score factors were Delivery of care, Respect, and Patient relations while the three lowest factors were Stress, Prudent strategies, and Personal time. Nearly half of the dentists were generally satisfied. The majority of dentists and staff were satisfied mainly with professional relations but with fair contentment about the income and time assigned for clinic management. The positive engagement in work was accompanied with the improvement in Clinical productivity (No significant association was detected between productivity (Job performance) and job burnout) and so on the dentist’s expenditure. (Table S8. Fig.1)
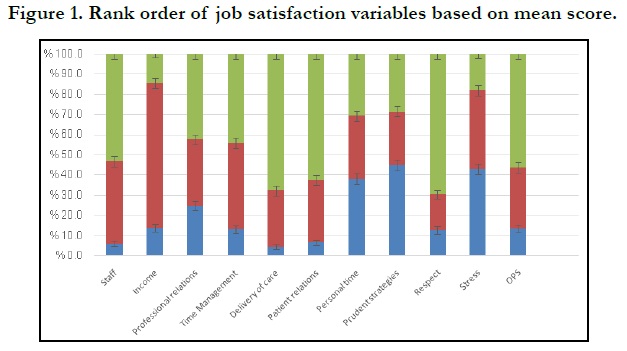
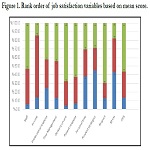
Figure 1. Rank order of job satisfaction variables based on mean score.
The effect of demographic and practice characteristics on TCS was evaluated by a stepwise-regression analysis (Table 4). Results showed that Specialty and Years of experience were significant predictors of TCS.
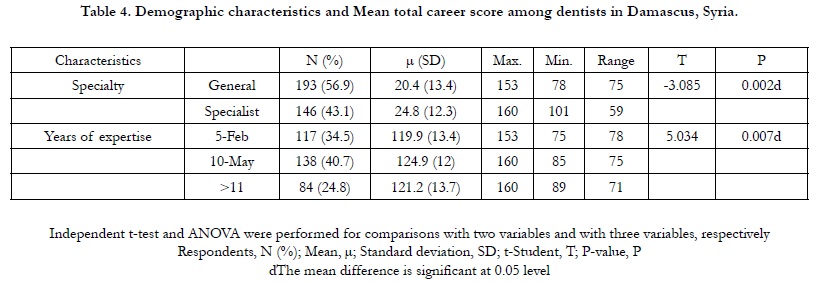
Table 4. Demographic characteristics and Mean total career score among dentists in Damascus, Syria.
As revealed in Table 5, the ANOVA table shows that the F-statistic was 21.5 and a significance level (Sig.) of 0.000. Therefore, the null hypothesis is rejected and the alternative hypothesis is accepted, proving that there is an impact of job stressors on overall Job satisfaction. In addition, there is a weak inverse correlation between scales of Job stressors and Job satisfaction (Table 5), representing the relative contribution of scales of job stressors (nature of work, patient-related stressors, time pressures, Fears from future, and profession-related stressor) in explaining the variance in the Job satisfaction.( Table S9 shows model summary – testing of hypothesis research).
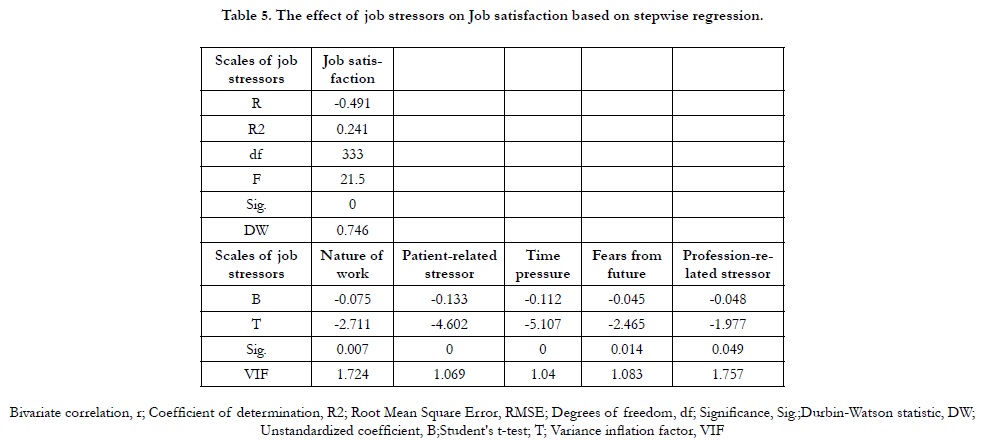
Table 5. The effect of job stressors on Job satisfaction based on stepwise regression.
Most common coping strategies used were interactions with people and spending money. The least common strategies were prescribed drugs and consumption of alcohol (Figure 2).
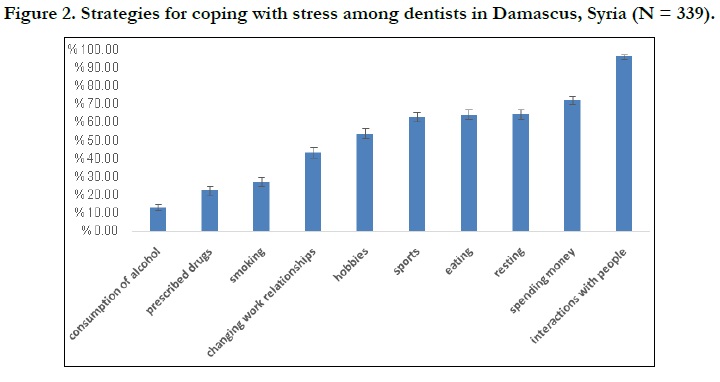
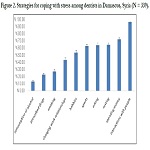
Figure 2. Strategies for coping with stress among dentists in Damascus, Syria (N = 339).
A higher proportion of males and specialists respondents reported using prescribed drugs, playing sports, engaging in hobbies, and smokingto deal with stress. Dentists who had recent graduated were more likely than other age groups to report playing sports and spending money, while older dentists were less likely than other age groups to report eating. Changing the work environment was a strategy used more by married dentists (73, 50%) than unmarried (74, 38.3%). Spending money and eating used as stress-coping strategies by fewer of more experienced dentists. Whereas, engaging in hobbies and resting used by fewer of less experienced dentists to manage stress. More dentists who work > 20 (hr./wk.) reported using drugs, eating, and changing the work environment as strategies for coping with job-related stress, and fewer dentists who have the best Monthly-pensions reported eating, drinking alcohol, and interacting with people as strategies for coping with stress. Whereas dentists who have the highest Monthly- pensions and work >40 (hr. /wk.) reported resting as a strategy to deal with stress. Fewer busier dentists (those who treated, on average, at least 12 patients per day) identified resting, eating, and playing sports as strategies for coping with work stress (Table 6).
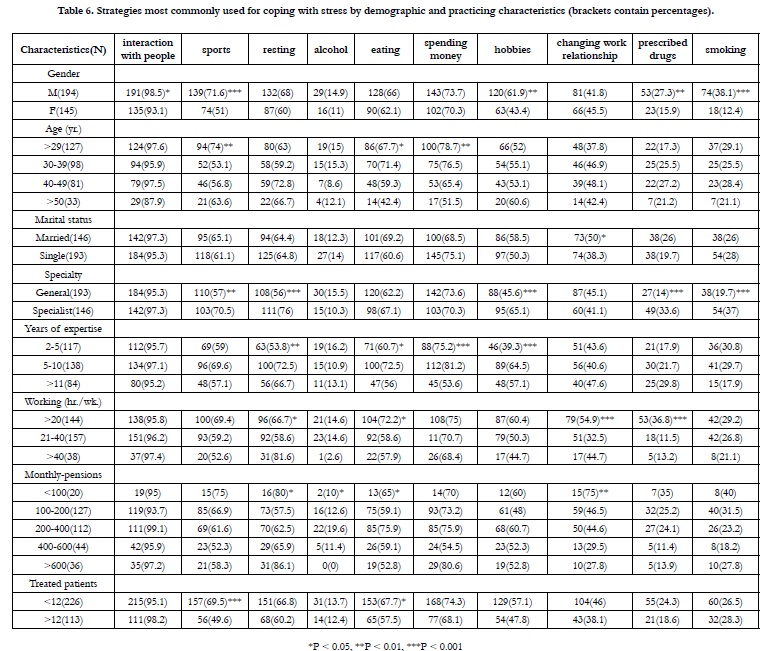
Table 6. Strategies most commonly used for coping with stress by demographic and practicing characteristics (brackets contain percentages).
Coping (incl.sports, spending money, resting, prescribed drugs, changing work relationships, and hobbies, respectively) served as a mediator between stress and experienced job satisfaction. With emotion focused coping, feeling loneliness and derogative were significantly correlated with job satisfaction which gave rise to advanced levels of psychological disturbance (Table 7).
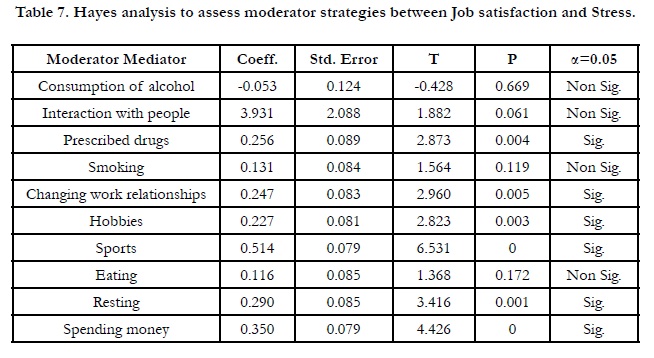
Table 7. Hayes analysis to assess moderator strategies between Job satisfaction and Stress.
Variables perceived stress and non-adaptive strategies to cope in addition to adaptive strategies and mindfulness were positively correlated with each other.
Discussion
Stress has widely documented physical and psychological consequences,
such as anxiety, burnout and the development of cardiovascular
diseases [18]. Although there is a number of more
recent stress measures used in the literature, we chose a modified
version of that used by Cooper et al., [17] to allow comparison
with previous work involving dentists.The current study found
that there was a considerable variation in the number of stressors
that dentists experienced frequently or all the time, with the number per dentist ranging from 1 to 28, This result is consistent
with those reported by dentists in New Zealand, the variation is
ranging from 0 to 31 [9].
61.86% of the dentists surveyed suffered from stress. Similar results
have been reported in studies of general dentists in the UK
(68.4%) [18], dentists in Denmark (59.7%) [21].
MTCS and mean overall professional satisfaction subscale score
were 122.3 out of 185 and 3.46 out of 5, respectively. These findings are parallel to other observations conducted in china, which
were 123.12 out of 190 and 3.28 out of 5 [19], respectively. Also,
in Australia, and Sweden studies [22, 23].
The most common stressors among dentists were related to the
nature of work (e.g., maintaining concentration, repetitive nature
of work, and the need to empathizing with children) that caused
their dissatisfaction with their success in their work under pressure.
Many of the frustrations associated with time pressures were
also evident, possibly due to pressure on dentists to schedule as many appointments as possible with limited time, long working
hours, and satisfaction with time was generally average (neutral)
that included professional interrelationship, overseas relations, official
obligations, transportation, In addition to private interrelations
(time allocated for personal relations and community meetings,
time assigned for research, and other interests not related to
work).
These frustrations may be partly the result of external pressures
to meet certain responsibilities (e.g., pressures by family and
friends, colleagues, and the medical community); but may also in
part be the result of the dentists’ own personal set of values and
sense of responsibilities, and urgent needs for enduring vocational
development, as there is a great emphasis these days on conducting
and publishing research, such circumstances undoubtedly
lead to increased tension, creating difficulties in integrating work
responsibilities with social life.These results are similar to those
in previously reported study [24]. Ayers et al. reported that the
second and third most common sources of stress among general
dentists in New Zealand were time-related pressure (48%) and the
need to maintain high levels of concentration at work (43%) [9].
In a study of dentists in Islamabad, Pakistan, finding enough time
for family and friends was reported as the most common source
of stress [24]. Cooper et al. indicated that time management problemswere
a common source of stress among dentists [17]. Other
study indicated that respondents were dissatisfied with stress and
time management [19].
Dentists in this study also pointed out many aspects of the practice
related to the conditions of the profession in general and
reported that it was stressful and negative for them ( e.g., feeling
with colleagueship marginalization, flooding of dentists in marketplace,
the urgent needs for enduring vocational development ,
fear of making mistakes or actually committing them, incompetency
in dealing with abrupt interventions through surgical operation,
equipment breakdown/defective materials, and unsatisfactory
laboratory service from technicians).
52.2% of respondents experiencing of medical emergency in the
dental surgery [9], although it has been found to be one of the
most highly ranking stressors in the UK [17], only 15% of dentists
reported that this was a stressor very often or all the time [9].
This may reflect a difference in the wording of the questionnaires
used; Cooper et al. [17] used a five point Likert-type scale ranging
from ‘no stress’ to ‘a great deal of stress’, whereas we used
a similar scale labeled ‘never’ to ‘all the time’. Although a medical
emergency would be one of the greatest potential sources of
stress, it does not occur commonly, and many dentists may not
have experienced such an event. Dentists also reported low satisfaction
with professional relationships, such as their relationships
with specialists in the medical arena and their contact with global
expertise.
Pressure related to income is clearly visible in dentists' self-reports
at work. Dentists have struggled with a conflict between profit
and professional ethics due to the increase in the general costs of
running a dental clinic and the necessity to pay specific fees, so
they need to work harder and see more patients and working long
hours to generate sufficient income.Income-related stressors are
reported to behigh for dentists working in the National Health
Service [25], where there is a perceived need to work quickly inorder
to generate sufficient income.
Job satisfaction with financial condition was low which included
pension, overall expenditures, conciliating paid-salaries and allowances,
billings, and premium-insurance payment.It seems that
negative attitudes about the health care system were predicted by
dissatisfactions and frustrations with procedures, limitations, and
bureaucratic regulations imposed on the profession by the government,
these pressures were less than previously reported [26].
The least frequent stressors were patient-related stressors (e.g.,
treatment of patient with troubles in comprehensive response,
treating non-responsive children, and feeling of devaluation from
patient).Ayers et al. [9] reported the most common source of
stress was treating uncooperative children (52%), and Kay et al.
reported that the most common stress is the patient’s demands
(75%), in the UK involved treating difficult or uncooperative
patients (64.8%) [27]. Dentists were satisfied with their patient
relations, as many dentists enter into medical school with noble
ideas of helping those who are suffering and in pain, and that
helping patients and being able to treat illness during patients’ adherence
to medication regimen were aspects of medical practice
that dentists valued and found meaningful. It is possible that the
gratification of knowing that someone in need has been helped is
one factor that makes the long hours and heavy workloads of the
dentist’s job more manageable.
Dentists appeared that the least sources of stress are the problems
of staff, majority of dentists were highly satisfied with performance
of the medical assistants, teamwork in healthcare, team
involvement in troubleshooting, this is due that staff was hired
and managed by the dentist or the organization affiliated with it.
Kay et al. reported that problems associated with staff are the
most common (56%) [27]. It is evident that the work of a dentist
still provides a great deal of general satisfaction as a career choice.
Respondents were neutral in their satisfaction with the practice
of the profession (dentistry fulfills current career aspirations,
satisfaction in work, ability dealing with disabilities, continuous
desire to gain knowledge, unwillingness to change career, and urging
high-school students to study dentistry), possibly it relates to
wanting to move away from any health-related job, having been
dissatisfied with one health-related career, it may also be that these
alternatives are more financially rewarding with less stress.
A number of stressors contributed significantly to dissatisfaction
with work as a dentist, the same stressors that contributed
to overall stress also contributed to dissatisfaction with practice.
It is difficult to speculate on the causal relationship between the
concepts of satisfaction and stress, the results show a negative
significant correlation between stress and job satisfaction.
Therefore, improving work condition is essential in order to
increase the level of satisfaction and thus to lower the level of
stress. Similar results were obtained in other professions [19].
No significant differences in occupational stress were observed
betweenmales and females, this finding mirrored two studiesin
Yemen and Iran which reported nostatistical differencesin stress
among men and women. However, Rogers et al.reported that
female Irish dentists were morestressed than males [20]. It was
found that males suffer from pressures related to the nature of
work more than females, one study showed males suffer from maintaining high levels of concentration and causing pain more
than females [9], perhaps because of childrearing and familyresponsibilities
greatly impact females’ working life and thatfemale
dentists are more likely to take a career break by more personal
time and relatively long maternity leave. While, female dentists
have suffered from financial and patient-related pressures more
than male, due to mismatch between the number of patients
treated and personal obligations.
The results reveal no gender differences in satisfaction levels, this
result is consistent with previous observation [15], and contrast
with two studies from Australia which referred to that female dentists
had higher job satisfaction than male dentists [22, 25]. Other
study conducted in Turkey reported that male dentists had higher
mean career satisfaction scores than female dentists [28].
Additionally, there were no significant differences in general stress
according to age, and this is consistent with a study reporting no
relationship between stress and age [24]. Older dentists were less
concerned about patient pressures, this is due to they are often
more experienced, which increases the ability to treat patients
with weak response, in addition to our society's traditions of respecting
and appreciating older dentists.Contrary to our findings,
there is no statistically significant difference in satisfaction according
to age; several previous studies indicated that older dentists
were more satisfied or less depressed with dentistry [15, 25].
There were no statistically significant differences in general stress
according to the working hours per week. More working hours
caused time pressures and more patients to secure sufficient income,
and increased fears of future. Ayers et al., reported that
time pressures and long work hours had a significant impact on
the stress of the dentist, and stated that weekly workload increased
fears related to future [9]. General satisfaction was not
associated with hours worked per week, but Chinese study, dentists
who work less than 40 hours per week were generally more
satisfied with dentistry [19].
According to years of experience, there were no statistically significant
differences in general stress, compared to study in Iran
that found dentists with fewer than 10 yrs. of experience exhibited
higher stress than dentists with over 20 yrs. of experience.
Similarly indicated in previous studies reported that experience is
a factor in controlling and managing stress [17, 24].
More satisfaction with dentists had 5-10 yrs. (vs. 2-5 yrs.); this can
be attributed to the decrease in practical and clinical experience,
and the increased fear of making mistakes in the younger dentists.
Overall occupational satisfaction in a study was significantly different
based on years of practice, it was reported that dentists
practicing > 5 yrs. were the most satisfied overall [19], with the
lowest satisfied for dentists with 6-10 yrs., this decrease may result
from increased professional responsibilities in both management
and research and patient care.
There were no statistically significant differences in general stress
and job satisfaction according to the number of patients who were
treated per day. In another study, it was found that longer working
hours also meansless personal time and less freedom of a working
schedule,contributing to lower job satisfaction [27]. There was an
increase in profession-related stressors (e.g.,fear of committing
mistakes or actually committing), in contrast, an increase in fear of the future whit more patients, was attributed to more consumption
of equipment and the possibility of increasing defects.
Specialistdentists were generally more satisfied with dentistry and
less stress than general dentists. They had significantly lower degrees
of time pressure, work pressures, financial pressures, patient
pressures, and fears of future than general dentists. This would
strongly suggest that, in order to improve job satisfaction, practitioners
should define their preferred fields of dentistry, and strive
to gain more experience and training, while avoiding areas where
they have less interest or ability.
There were no significant differences in overall stress and satisfaction
according to income. While there is an increase in professionrelated
stressors, the lower the monthly income, the reason may
be that dentists resort to using less quality materials or because of
their inability to equip their patients with modern equipment that
helps them in continuing professional development because of
the high prices that contradict their low income.
The most common techniques for managing stress identified
in the current study were interactions with people (92.2%); this
strategy did not modify the relationship between satisfaction and
stress, it is likely that dentists interact with people more, without
identifying this as a technique to manage stress, spending
money (72.3%) and resting (64.6%). The least commonly used
were smoking (27.1%), prescribed drugs (22.4%) and alcohol
consumption (13.3%). In New Zealand, the most common reference
strategy was interactions with people (77.3%), while the least
strategies were smoking (4%) and prescribed drugs (3%) [9].
Tobacco use as a coping mechanism is similarly low in the UK
8.6% and in Iran 4.3% of dentists reporting that they smoke to
manage stress [17, 27] Similarly, smoking and drug use were not
frequently reported as strategies used by Dutch dentists to manage
stress [29].
13.3% of the respondents used alcohol to relieve stress, other
authors have reported worrying use of alcohol by dentists [29].
Conversely,Myers and Myers [18] reported that, although .90%
of dentists in their sample consumed alcohol regularly, the mean
weekly consumption was low.
Consistent with reports from previous study [30], dentists tended
not to apply active coping strategies forstress management. The
gender differences were not unexpected with males more likely
to report using sports, interacting with people, practicing hobbies,
using drugs and smoking, have been reported as strategies
to relieve stress.There were no statistically significant differences
between males and females regarding the use of the strategy to
change the work environment, and it contradicts a study that
found that more males (26%) use it compared to females (16%).
The strategies used by dentists were similar regardless of their
monthly income, except that a smaller percentage of dentists with
higher income ate and changed the work environment, and none
of them recorded drinking alcohol.
Conclusion
A major cause of stress among dentists is a lack of knowledge
about managing stress [27], the most common type of stress in dentists in Syria has been maintaining high levels of concentration,
time pressure, repetitive nature of work, and empathizing
with children, there are differences in the strategies used by male
and female practitioners to manage stress.
For Syrian dentists, total career satisfaction was judged to be good
overall. Delivery of care, patientand staff relations, and respect
were most satisfied factors, while lack of personal time, lower income,
and stress were the least satisfied factors. A clear increase
in job satisfaction scores was predicted on the basis of specialty
(more specialist) and years of practice 5-10 (vs. 2-5).
Therefore, Policies defining the standard of dental care need to be
made, stress management and coping strategies should therefore
be included in the dental curriculum in order to avoid physical
and psychological problems that may occur later as a result of
occupational stress, and workshops, seminars and education programs
on occupational stress and practice management for dental
students and dentists should be organized periodically.
Stress literature is curious, particularly given its importance in the
depression literature.
Further exploration of the importance of this variable may therefore
remain a good avenue for further research.
Future studies exploring the job satisfaction of Syrian dentistscan
build upon this study byother regions with different demographicsand
investigating how leadership roles impact job satisfaction,
to identify interventions that can be used to reduce stress between
dentists and improve their working conditions.
References
- Johnson PR, Indvik J. Stress and workplace violence: it takes two to tango. J ManagPsychol. 1996 Sep 1;11(6):18-27.
- Selye H. Stress without Distress. In: Serban G. (eds) Psychopathology of Human Adaptation. Springer, Boston, MA, pp.137-146, 1976.
- Gangwar A, Kiran UV. Occupational Stress among Dentists.J Sci Eng Res. 2016;4(7):28-30.
- Donald I, Taylor P, Johnson S, Cooper C, Cartwright S, Robertson S. Work environments, stress, and productivity: An examination using ASSET. Int J Stress Manag. 2005 Nov;12(4):409.
- Islam MM, Ekuni D, Yoneda T, Yokoi A, Morita M. Influence of Occupational Stress and Coping Style on Periodontitis among Japanese Workers: A Cross-Sectional Study. Int J Environ Res Public Health. 2019 Sep 22;16(19):3540.Pubmed PMID: 31546684.
- Boran A, Shawaheen M, Khader Y, Amarin Z, Hill Rice V. Work-related stress among health professionals in northern Jordan. Occup Med (Lond). 2012 Mar;62(2):145-7.Pubmed PMID: 22121245.
- Denton DA, Newton JT, Bower EJ. Occupational burnout and work engagement: a national survey of dentists in the United Kingdom. Br Dent J. 2008 Oct 11;205(7):E13.Pubmed PMID: 18849939.
- Collin V, Toon M, O'Selmo E, Reynolds L, Whitehead P. A survey of stress, burnout and well-being in UK dentists. Br Dent J. 2019 Jan 11;226(1):40- 49.Pubmed PMID: 30631165.
- Ayers KM, Thomson WM, Newton JT, Rich AM. Job stressors of New Zealand dentists and their coping strategies. Occup Med (Lond). 2008 Jun;58(4):275-81.Pubmed PMID: 18296684.
- Chipchase SY, Chapman HR, Bretherton R. A study to explore if dentists' anxiety affects their clinical decision-making. Br. Dent. J. 2017 Feb;222(4):277-90.
- Gorter RC, Albrecht G, Hoogstraten J, Eijkman MAJ. Professional burnout among Dutch dentists. Community Dent Oral Epidemiol. 1999;27(2):109-116.
- Hall DT, Chandler DE. Psychological success: When the career is acalling. J Organ Behav 2005;26(2):155-176.
- Shugars DA, DiMatteo MR, Hays RD, Cretin S, Johnson JD. Professional satisfaction among California general dentists. J Dent Educ. 1990 Nov;54(11):661-9.Pubmed PMID: 2229622.
- Folkman S, Lazarus RS, Dunkel-Schetter C, DeLongis A, Gruen RJ. Dynamics of a stressful encounter: cognitive appraisal, coping, and encounter outcomes. J Pers Soc Psychol. 1986 May;50(5):992-1003.Pubmed PMID: 3712234.
- Gilmour J, Stewardson DA, Shugars DA, Burke FJ. An assessment of career satisfaction among a group of general dental practitioners in Staffordshire. Br Dent J. 2005 Jun 11;198(11):701-4.Pubmed PMID: 15951785.
- Folkman S, Moskowitz JT. Positive affect and the other side of coping. Am Psychol. 2000 Jun;55(6):647-54.Pubmed PMID: 10892207.
- Cooper CL, Watts J, Kelly M. Job satisfaction, mental health, and job stressors among general dental practitioners in the UK. Br Dent J. 1987 Jan 24;162(2):77-81.Pubmed PMID: 3468971.
- Myers HL, Myers LB. 'It's difficult being a dentist': stress and health in the general dental practitioner. Br Dent J. 2004 Jul 24;197(2):89-93.Pubmed PMID: 15272347.
- Cui X, Dunning DG, An N. Satisfaction among early and mid-career dentists in a metropolitan dental hospital in China. J Healthc Leadersh. 2017 Jun 6;9:35-45.Pubmed PMID: 29355243.
- Roth SF, Heo G, Varnhagen C, Glover KE, Major PW. Job satisfaction among Canadian orthodontists. Am J Orthod Dentofacial Orthop. 2003 Jun;123(6):695-700.Pubmed PMID: 12806353.
- Moore R, Brødsgaard I. Dentists' perceived stress and its relation to perceptions about anxious patients. Community Dent Oral Epidemiol. 2001 Feb;29(1):73-80.Pubmed PMID: 11153566.
- Luzzi L, Spencer AJ. Job satisfaction of the oral health labour force in Australia. Aust Dent J. 2011 Mar;56(1):23-32.Pubmed PMID: 21332737.
- Ordell S, Söderfeldt B, Hjalmers K, Berthelsen H, Bergström K. Organization and overall job satisfaction among publicly employed, salaried dentists in Sweden and Denmark. Acta Odontol Scand. 2013 Nov;71(6):1443-52. Pubmed PMID: 23972204.
- Alvi H. The prevalence of stress and associated factors in dentists working at Islamic International Dental College Hospital, Islamabad. Pak Oral Dent J. 2010 Dec 1;30(2):521-5.
- Luzzi L, Spencer AJ, Jones K, Teusner D. Job satisfaction of registered dental practitioners. Aust Dent J. 2005 Sep;50(3):179-85. Pubmed PMID: 16238216.
- Humphris GM, Cooper CL. New stressors for GDPs in the past ten years: a qualitative study. Br Dent J. 1998 Oct 24;185(8):404-6.Pubmed PMID: 9828501.
- Pouradeli S, Shahravan A, Eskandarizdeh A, Rafie F, Hashemipour MA. Occupational Stress and Coping Behaviours Among Dentists in Kerman, Iran. Sultan Qaboos Univ Med J. 2016 Aug;16(3):e341-6.Pubmed PMID: 27606115.
- Sur H, Hayran O, Mumcu G, Soylemez D, Atli H, Yildirim C. Factors affecting dental job satisfaction: a cross-sectional survey in Turkey. Eval Health Prof. 2004 Jun;27(2):152-64.Pubmed PMID: 15140292.
- Gorter RC, Eijkman MA, Hoogstraten J. Burnout and health among Dutch dentists. Eur J Oral Sci. 2000 Aug;108(4):261-7.Pubmed PMID: 10946759.
- Newton JT, Gibbons DE. Stress in dental practice: a qualitative comparison of dentists working within the NHS and those working within an independent capitation scheme. Br Dent J. 1996 May 11;180(9):329-34.Pubmed PMID: 8664089.





