Oral Hygiene Status and Dental Caries Experience in Patients with Dental Fluorosis Visiting A Private Dental Institution in Chennai
Nivetha G1, Sri Sakthi D2*, Arvind S3
1 Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
2 Reader, Department of Public Health Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
3 Reader, Department of Orthodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University,
Chennai, 600077, India.
*Corresponding Author
Sri Sakthi,
Reader, Department of Public Health Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077,
India.
Tel: 8122399966
E-mail: srisakthi@saveetha.com
Received: July 08, 2019; Accepted: August 03, 2019; Published: August 08, 2019
Citation: Nivetha G, Sri Sakthi D, Arvind S. Oral Hygiene Status and Dental Caries Experience in Patients with Dental Fluorosis Visiting A Private Dental Institution in Chennai. Int J Dentistry Oral Sci. 2020;7(10):955-959. doi: dx.doi.org/10.19070/2377-8075-20000189
Copyright: Sri Sakthi© 2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Dental fluorosis exhibits as enamel mottling, surface irregularities, leading to plaque accumulation and thereby leading to dental
caries and periodontal diseases. The aim of the study was find out the association of oral hygiene status and dental caries in
patients with dental fluorosis visiting Saveetha Dental College. A retrospective study was carried out in Saveetha Dental College
between June 2019-March 2020.The study population consisted of young adults who reported with dental fluorosis.The data was
collected from patients records analysed from the data of 86000 patients between June 2019-March 2020 and entered in Excel
sheets.The collected data were subjected to statistical analysis using SPSS software.A chi square test was done and a p value of <
0.05 was considered to be statistically significant. The independent variables present in this study were age and gender.The dependent
variables were fluorosis,DMFT and OHI scores. The results showed that 53% of fluorosis patients had less than score of
dental caries status and 56% of fluorosis had fair oral hygiene status. The study concludes that a lesser degree of dental caries and
fair oral hygiene status were found in out patients with dental fluorosis.
2.Introduction
3.Materials and Method
4.Results and Discussion
5.Conclusion
6.Acknowledgement
7.References
Keywords
Fluorosis; Oral Health; Young Adults.
Introduction
Oral health is recognised and accepted as equally important when
compared to general health. Oral health can be defined as standard
health of the oral and related tissues which enables individuals
to eat, speak and socialize without active-disease, discomfort
which contribute to general health [1]. Oral disease can be considered
as a public health problem due to their higher prevalence
and social impact [2]. Poor oral health affects the quality of life in
children, adults and old people. In adults, routine daily activities
may be disrespected and lead to economic loss [3]. Poor oral hygiene
and nutritional practices disturb the ecological homeostasis
in plaque thereby causing an inexorable shift in plaque ecology
towards highly cariogenic microorganisms [4].
Dental caries are multifactorial, primarily depending on host,
agent and environmental factors. It is formed by the interaction
between acid producing bacteria and fermentable carbohydrate
which leads to a break in the balance between demineralization
and remineralization [5]. Streptococcus mutans and Lactobacillus
acidophilus are the primary causative microorganisms for the
development of dental caries [6]. It is the most common chronic
disease that interferes with normal nutrition intake, speech, and
daily routine activities Dental caries are the major oral health
problems and indicators of oral health problems all over the
world [7]. The prevalence of dental caries has high graded society
and wide geographic spread [8]. Fluoride is an essential component
for normal mineralization of bones and dental enamel [9].
The main source of fluoride for the human body is usually in
drinking water that covers about 75-90% of daily intake [10]. The
higher concentrations of fluoride causes serious health problems
namely dental fluorosis, skeletal fluorosis and non-skeletal fluorosis. Dental fluorosis is considered the earliest sign of fluoride
intoxication. Fluorosis may have direct as well as indirect effect on
oral hygiene status. It causes failure of cementalresorption leading
to hypercementosis and osteonecrosis [11]. Indirectly, it causes
plaque associated periodontal disease [12].
Fluorides is the protective agent for dental caries [13] .The use
of fluorides for prevention of dental caries has been proven to
be a safe and effective public health strategy to reduce the burden
of dental disease of the population in industrialized and developing
countries. Adequate program monitoring and quality control
maintenance can minimize occurrence of enamel mottling
in communities using fluorides for dental caries prevention [14].
Previously our team has conducted numerous cross sectional
studies [7, 15, 16], clinical trials [4, 6, 17-20], in-vitro studies [9, 21,
24] and review (25 over the past 5 years. Now we are focussing
on epidemiological surveys. The present aimed to find out the degree
of dental caries and oral hygiene status in fluorosis patients
among young adults who visiting Saveetha Dental College.
Retrospective study.
A retrospective study was carried out among young adults reporting
to Saveetha Dental College and Hospital.The study was
conducted between June 2019-March 2020.The study population
consisted of young adults .i.e 18-35 years who were reported with
dental fluorosis.
Ethical approval was obtained from the Institutional Ethical
Committee and Scientific Review Board (SRB) of Saveetha Dental
College.SDC/SIHEC/2020/DIASDATA/0619-0320.
The data were collected by analyzing the records of 86000 patients
between June 2019-March 2020.The data comprised 100
patients who were reported with dental fluorosis.The data includes
patient’s details, OHI score, DMFT score and fluorosis score .The dental fluorosis were assessed by Dean’s Fluorosis Index
and categorized as very mild, mild and questionable. The oral
hygiene status were assessed by Oral Hygiene Simplified Index
and categorized as good, fair and poor. The dental caries status
were assessed by DMFT (Decayed-Missing-Filled-Teeth index)
and categorized as score of less than 5, 5-10 and greater than 10.
The collected data were entered in Excel sheet and subjected to
statistical analysis using SPSS software.Chi square test were done
between DMFT and fluorosis score, OHI and fluorosis and OHI
and DMFT.The independent variables were age and gender while
dependent variables were OHI, DMFT and fluorosis. The level of
significance is p<0.05.
Results and Discussion
Dental fluorosis is recognised as an oral health disease of public
health.It results in poor esthetic appearance which may have a
psychological bearing and leading to low confidence level [26].
Adulthood is the stage were the individuals lays the foundation
for oral health, environmental factors, parentalcare, socioeconomic
status are the elements which shapes the individuals attitude
towards oral hygiene and treatment needs.
Our aim in this study was to find out the association of oral hygiene
status,dental caries in fluorosis patients visiting Saveetha
Dental College. Totally, 100 fluorosis patients were included in
this study. About 41% were 18-25 age group ,47%were 26-32 age
group and 12% were 32+ age group (chart 1). Out of 100 fluorosis
patients, 77% were Male and 23% were females (chart 2).
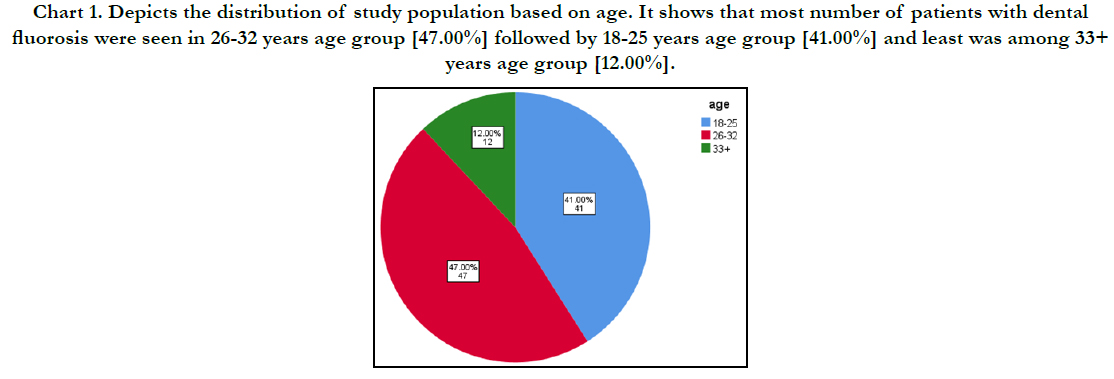
Chart 1. Depicts the distribution of study population based on age. It shows that most number of patients with dental fluorosis were seen in 26-32 years age group [47.00%] followed by 18-25 years age group [41.00%] and least was among 33+ years age group [12.00%].
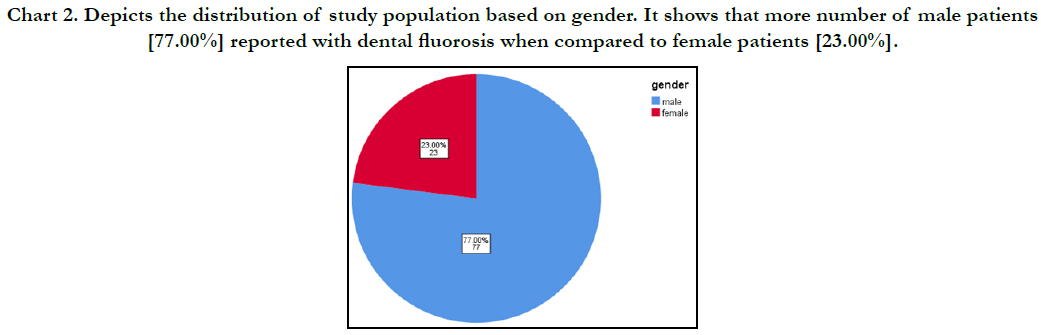
Chart 2. Depicts the distribution of study population based on gender. It shows that more number of male patients [77.00%] reported with dental fluorosis when compared to female patients [23.00%].
Majority of patients with very mild fluorosis had fair oral hygiene status and < 5 DMFT score whereas patients with mild fluorosis had fair oral hygiene status and were in 5-10 DMFT score category. Patients with questionable fluorosis had fair oral hygiene status and < 5 DMFT score status. About 56% fluorosis patients had scores of >5 DMFT score which was found to be statistically not significant (graph 1). Previous studies conducted by Sudhakar et al,Koteha et al, Tsutusi et al and Mascarenhas et al [27- 30] reported with lesser degree of dental caries status in dental fluorosis patients which is similar to our present study. 53% of dental fluorosis patients had fair oral hygiene status. Association between OHI(s) and dental fluorosis was found to be statistically not significant (graph 4). The study conducted by Vora k et al, Shetty et al., and Reddy et al., [31-33] concluded that poor oral hygiene status was seen in dental fluorosis patients which was dissimilar to our present study. More number of patients with fair oral hygiene status had <5 DMFT score. A chi square analysis was done to check the association between DMFT score and Oral hygiene status of study population, even though a difference was observed based on the level of oral hygiene, it was not found to be statistically significant (graph 5).
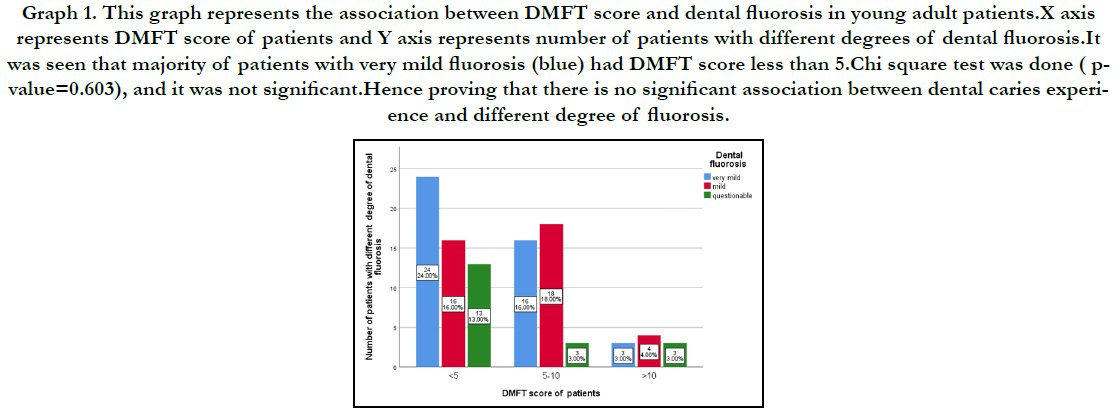
Graph 1. This graph represents the association between DMFT score and dental fluorosis in young adult patients.X axis represents DMFT score of patients and Y axis represents number of patients with different degrees of dental fluorosis.It was seen that majority of patients with very mild fluorosis (blue) had DMFT score less than 5.Chi square test was done ( pvalue= 0.603), and it was not significant.Hence proving that there is no significant association between dental caries experience and different degree of fluorosis.


Graph 2. This graph represents the association between OHI(s) and dental fluorosis of young adults. X axis represents OHI score of patients and Y axis represents number of patients with degree of dental fluorosis. It was seen that the majority of patients with fair oral hygiene status had very mild dental fluorosis (green). Chi square test was done (pvalue= 0.209),and it was not significant. proving that there is no significant association between Oral hygiene status of patients and patients with different degrees of dental fluorosis.

Graph 3. This graph represents the association between OHI(s) and DMFT scores of young adults.X axis represents DMFT score of patients and Y axis represents number of patients based on their oral hygiene status. Even though, majority of the patients with good (blue) and Fair (red) oral hygiene were in <5 and 5-10 DMFT score category, A chi square test done (p-value=0.884), revealed no statistically significant association between the two variables in the study population./strong>
The main of this study is limited sample size and confined to a
single source for data. Further descriptive studies on a larger scale
can help us to give comprehensive data for arriving at a conclusion
and to plan health oral health programs for the population
studied.
Conclusion
Within the limitations of the current study, it can be concluded
that low to moderate level of caries risk was found in patients
with dental fluorosis and cumulatively the oral hygiene status of
the patients was found to be fair; indicating the need to educate
the patients on proper brushing methods and oral hygiene practice,
thereby reducing the dental caries risk also.
Acknowledgement
I sincerely express my gratitude and acknowledgement to Dr. Sri Sakthi and Dr. Arvind Sivakumar and Dean and management for
their support and also thank the Research and IT department of
Saveetha dental college for their affable assistance in analyzing
the data.
References
- Azodo CC, Ehizele AO, Umoh A, Ojehanon PI, Akhionbare O, Okechukwu R, et al. Perceived oral health status and treatment needs of dental auxiliaries. Libyan J Med. 2010 Mar 15;5:4859.Pubmed PMID: 21483589.
- Nagaraj P, Mani G. Knowledge, Attitude and Practice Among 13–15 Years Old School Children Towards Oral Hygiene. Indian J Public Health Res Dev. 2019;10(3):149-53.
- Naito M, Yuasa H, Nomura Y, Nakayama T, Hamajima N, Hanada N. Oral health status and health-related quality of life: a systematic review. J Oral Sci. 2006;48(1):1-7.
- Samuel SR, Acharya S, Rao JC. School Interventions-based Prevention of Early-Childhood Caries among 3-5-year-old children from very low socioeconomic status: Two-year randomized trial. J Public Health Dent. 2020 Jan;80(1):51-60.Pubmed PMID: 31710096.
- Peres MA, Peres KG, de Barros AJ, Victora CG. The relation between family socioeconomic trajectories from childhood to adolescence and dental caries and associated oral behaviours. J Epidemiol Community Health. 2007 Feb;61(2):141-5.Pubmed PMID: 17234873.
- Prabakar J, John J, Arumugham IM, Kumar RP, Sakthi DS. Comparing the Effectiveness of Probiotic, Green Tea, and Chlorhexidine- and Fluoride-containing Dentifrices on Oral Microbial Flora: A Double-blind, Randomized Clinical Trial. ContempClin Dent. 2018 Oct-Dec;9(4):560-569.Pubmed PMID: 31772463.
- Prabakar J, John J, Srisakthi D. Prevalence of dental caries and treatment needs among school going children of Chandigarh. Indian J Dent Res. 2016 Sep-Oct;27(5):547-552.Pubmed PMID: 27966516.
- Manjiri J, Mansi T, Ajay P. Prevalence of dental caries, periodontal diseases and periapicalpathoses among patients attending a tertiary dental care centre in central Gujrat. A hospital-based cross-sectional study. Int J Exp Dent Sci. 2016;5:89-92.
- Kumar RP, Vijayalakshmi B. Assessment of fluoride concentration in ground water in Madurai district, Tamil Nadu, India. Res J Pharm Technol. 2017;10(1):309-10.
- Zohouri FV, Rugg-Gunn AJ. Sources of dietary fluoride intake in 4-year-old children residing in low, medium and high fluoride areas in Iran. Int J Food SciNutr. 2000 Sep;51(5):317-26.Pubmed PMID: 11103297.
- Haikel Y, Turlot JC, Cahen PM, Frank R. Periodontal treatment needs in populations of high- and low-fluoride areas of Morocco. J ClinPeriodontol. 1989 Oct;16(9):596-600.Pubmed PMID: 2677057.
- Krook L, Maylin GA, Lillie JH, Wallace RS. Dental fluorosis in cattle. The Cornell Veterinarian. 1983 Oct 1;73(4):340-62.
- Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century--the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003 Dec;31Suppl 1:3-23.Pubmed PMID: 15015736.
- Doumit M, Doughan B. Dental caries and fluorosis among children in Lebanon. Indian J Dent Res. 2018 May-Jun;29(3):317-322.Pubmed PMID: 29900915.
- KANNAN SS, KUMAR VS, RATHINAVELU PK, INDIRAN MA. AWARENESS AND ATTITUDE TOWARDS MASS DISASTER AND ITS MANAGEMENT AMONG HOUSE SURGEONS IN A DENTAL COLLEGE AND HOSPITAL IN CHENNAI, INDIA. WIT Transactions on The Built Environment. 2017 Sep 7;173:121-9.
- Neralla M, Jayabalan J, George R, Rajan J, MP SK, Haque AE, et al. Role of nutrition in rehabilitation of patients following surgery for oral squamous cell carcinoma. Int. J. Res. Pharm. Sci. 2019 Oct 16;10(4):3197-203.
- Prabakar J, John J, Arumugham IM, Kumar RP, Srisakthi D. Comparative Evaluation of Retention, Cariostatic Effect and Discoloration of Conventional and Hydrophilic Sealants - A Single Blinded Randomized Split Mouth Clinical Trial. ContempClin Dent. 2018 Sep;9(Suppl 2):S233-S239.Pubmed PMID: 30294150.
- Mathew MG, Samuel SR, Soni AJ, Roopa KB. Evaluation of adhesion of Streptococcus mutans, plaque accumulation on zirconia and stainless steel crowns, and surrounding gingival inflammation in primary molars: randomized controlled trial. Clin Oral Investig. 2020 Sep;24(9):3275-3280.Pubmed PMID: 31955271.
- Khatri SG, Madan KA, Srinivasan SR, Acharya S. Retention of moisturetolerant fluoride-releasing sealant and amorphous calcium phosphate-containing sealant in 6-9-year-old children: A randomized controlled trial. J Indian SocPedodPrev Dent. 2019 Jan-Mar;37(1):92-98. Pubmed PMID: 30804314.
- Pratha AA, Prabakar J. Comparing the effect of Carbonated and energy drinks on salivary pH-In Vivo Randomized Controlled Trial. Res J Pharm Technol. 2019;12(10):4699-702.
- Prabhakar AR, Murthy SA, Sugandhan S. Comparative evaluation of the length of resin tags, viscosity and microleakage of pit and fissure sealants - an in vitro scanning electron microscope study. ContempClin Dent. 2011 Oct;2(4):324-30.Pubmed PMID: 22346161.
- Pavithra RP, Jayashri P. Influence of Naturally Occurring Phytochemicals on Oral Health. Res J Pharm Technol. 2019;12(8):3979-83.
- Mohapatra S, Kumar RP, Arumugham IM, Sakthi D, Jayashri P. Assessment of Microhardness of Enamel Carious Like Lesions After Treatment with Nova Min, Bio Min and Remin Pro Containing Toothpastes: An in Vitro Study. Indian J Public Health Res Dev. 2019;10(10):375-80.
- Kumar RP, Preethi R. Assessment of Water Quality and Pollution of Porur, Chembarambakkam and Puzhal Lake. Res J Pharm Technol. 2017;10(7):2157-9.
- Harini G, Leelavathi L. Nicotine replacement therapy for smoking cessation- An overview. Indian J Public Health Res Dev. 2019;10(11):3588.
- Jackson SL, Vann Jr WF, Kotch JB, Pahel BT, Lee JY. Impact of poor oral health on children's school attendance and performance. Am J Public Health. 2011 Oct;101(10):1900-6.
- Anuradha B, Laxmi GS, Sudhakar P, Malik V, Reddy KA, Reddy SN, et al. Prevalence of dental caries among 13 and 15-year-old school children in an endemic fluorosis area: a cross-sectional study. J Contemp Dent Pract. 2011 Nov 1;12(6):447-50.Pubmed PMID: 22269235.
- Kotecha PV, Patel SV, Bhalani KD, Shah D, Shah VS, Mehta KG. Prevalence of dental fluorosis & dental caries in association with high levels of drinking water fluoride content in a district of Gujarat, India. Indian J Med Res. 2012 Jun;135(6):873-7.Pubmed PMID: 22825606.
- Tsutsui A, Yagi M, Horowitz AM. The prevalence of dental caries and fluorosis in Japanese communities with up to 1.4 ppm of naturally occurring fluoride. J Public Health Dent. 2000 Summer;60(3):147-53.Pubmed PMID: 11109211.
- Mascarenhas AK, Mashabi S. High fluoride concentration in drinking water may increase the prevalence and severity of dental fluorosis, and decrease occurrence of caries. J Evid Based Dent Pract. 2008 Mar;8(1):15-6.Pubmed PMID: 18346695.
- Vora KS, Vora PK. Assessment of periodontal status of the patients with dental fluorosis in area with natural high levels of fluoride: A cross-sectional survey. Dent. Hypotheses. 2013 Oct 1;4(4):127.
- Shetty P, Shamala A, Murali R, Mansi Y, Srivastava R, Debnath A. Dental fluorosis and oral health status of 13–15-Year-Old school children of Chikkaballapur District: A cross-sectional study. J Indian Assoc Public Health Dent. 2017 Apr 1;15(2):140.
- Reddy J, Parker JR, Africa CW, Stephen LX. Prevalence and severity of periodontitis in a high fluoride area in South Africa. Community Dent Oral Epidemiol. 1985 Apr;13(2):108-12.Pubmed PMID: 3857145.





