Effect Of Gender On The Prevalence Of Class II Restoration In Mandibular First Molars - A Retrospective Case Analysis Of 86,000 Cases
Sandhya A1, Surendar Sugumaran2*, Senthil Murugan P3
1 Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
2 Senior Lecturer, Department of Conservative and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
3 Associate Professor, Department of Oral and Maxillofacial Surgery, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
*Corresponding Author
Surendar Sugumaran,
Senior Lecturer, Department of Conservative and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University,
Chennai, 600077, India.
Tel: +919791183388
E-mail: surendars.sdc@saveetha.com
Received: September 06, 2020; Accepted: October 09, 2020; Published: October 27, 2020
Citation:Sandhya A, Surendar Sugumaran, Senthil Murugan P. Effect Of Gender On The Prevalence Of Class II Restoration In Mandibular First Molars - A Retrospective Case Analysis Of 86,000 Cases. Int J Dentistry Oral Sci. 2020;7(10):937-941. doi: dx.doi.org/10.19070/2377-8075-20000185
Copyright: Surendar Sugumaran©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Dental amalgam is one of the most versatile restorative materials used in dentistry. It constitutes approximately 75%
of all restorative materials used by dentists. It has served as a dental restoration for more than 165 years. There is still no adequate
economic alternative for dental amalgam. The combination of reliable long-term performance in load bearing situations and low
cost is unmatched by other dental restorative material.
Aim: The present study aims to evaluate the association between age and gender of patients who underwent amalgam class II
restoration in mandibular first molar.
Materials and Method: The study sample consists of all patients between the age group 18-71 years who underwent amalgam
class II restoration in mandibular first molar from june 2019 - april 2020 at the SDC. The data collected were analysed for the
number, age, gender for amalgam class II restoration in mandibular first molar. For a comparison between different variables,
statistical package IBM SPSS 20 software analyzer was used and the statistics were obtained.
Result: In this study, we can contemplate that Males(50.6%) have undergone more amalgam class II restoration in mandibular
first molar when compared to females. Whereas, people of age groups 18-30 years(37%) have undergone more amalgam class
II restoration in mandibular first molar. When compared to 36, more number of amalgam class II restoration was done in 46
(50.6%). There is no significant association between age, gender in patients undergoing amalgam class II restoration in mandibular
first molar. Risk analysis was done. It is observed that males have higher risk when compared to females with highest confidence
interval 1.490 and lowest confidence interval 0.785. (risk value - 1.082, males>females)
Conclusion: Within the limitations, the age group 18-30 years underwent more amalgam class II restoration in the mandibular
first molar. The Male population seem to have undergone more amalgam class II restoration in the mandibular first molar and are
at greater risk when compared to females.
2.Introduction
3.Materials and Method
4.Results and Discussion
5.Conclusion
6.Acknowledgement
7.References
Keywords
Age; Amalgam Class II Restoration; Mandibular 1st Molar; Gender.
Introduction
Dental caries is an infectious disease [1-4] that results in localised
dissolution and destruction of the calcified tissues of teeth. The
high prevalence of dental caries is thought to be strongly associated
with dietary habits and increased consumption of sugar [4].
Dental caries is the most prevalent infectious disease in humans,
affecting 97% of the population in their lifetimes [5]. It can affect
various sites of the tooth. The most common sites for caries to
occur are pits and fissure and proximal surfaces. These areas are
more difficult to clean and thus more prone to caries. First molar
is the first among the permanent teeth to erupt and get caries
earlier. Proximal caries can progress silently and may take years
to reach pulp.
Extensive studies of the setting reaction of dental amalgams, performed
by Gayler in 1937, further elucidated the mechanism of
setting of amalgam and influence of amalgam components on expansion due to the gamma-1 phase (Ag–Hg) and contraction
due to the formation of gamma-2 phase (Sn–Hg) [9]. Greener
in 1979 claimed that there is misinterpretation of Gayler’s work
regarding the concentration of Cu, that the concentration of Cu
above 5% produced increase expansion. What Gayler did say was
that if Cu was substituted for tin so that the concentration of
tin dropped below 25% expansion could occur; but if Cu was
substituted for silver so that tin concentration was maintained at
27%, no excess expansion occurred. This confusion surrounding
the concentration of Cu has resulted in a 25- 25–30 year delay
in the development of amalgams resistant to corrosion. In 1959,
Dr. Wilmer Eames recommended a 1:1 ratio of mercury to alloy,
thus lowering the 8:5 ratio of mercury to alloy that others
had been recommending. In 1962, a spherical particle dental alloy
was introduced. This was followed in 1963 by a high copper
dispersion alloy system that proved to be superior to its low
copper predecessors. Although this performance was theorized
to be the result of dispersion strengthening of the alloy, researchers
discovered that the additional copper combined with the tin,
creating a copper-tin phase that was less susceptible to corrosion
than the tin-mercury (gamma-2) phase found in low copper alloys.
Introduction of a new atomization process in the manufacture
of dental amalgams led to a dramatic improvement in the quality
and ease of manipulation with this material. This process involves
spraying of the molten alloy into a chamber containing an inert
gas by a patented atomization process. The molten metal forms
droplets which solidify. These spheres are then subjected to some
heat treatment. Thus, spherical particles are formed [6].
Composition of currently used amalgam alloy is silver 40-70%,
tin 12-30% and copper 12-24%. It may also include indium 0-4%,
palladium 0.5% and zinc up to 1%. Zinc prevents the oxidation
of other metals in the alloy during the manufacturing process [7].
[8, 9] Zinc also inhibits corrosion [10]. To overcome the limitation
of micro leakage with amalgams, a coating of unfilled resin over
the restoration margins and the adjacent enamel, after etching the
enamel, has been tried. Although the resin may eventually wear
away, it delays microleakage until corrosion products begin to fill
the tooth restoration interface.
Although adhesive dentistry and aesthetic restorative materials
have had significant development [11], choosing the best material
to restore dental structures is still controversial. A recent systematic
review of the literature highlights the benefits of dental amalgam
restorations in posterior teeth compared to resin composites
[12]. Indeed, the dental amalgam has been the chosen material
for more than 150 years, especially due to its excellent long-term
clinical performance and low cost [13]. However, a gradual decrease
in the use of amalgam has been noticed in some countries
[14], especially because it is non-aesthetical and it is not easily
available material. Besides its potential risk to human health, resin
composites have become more commonly used in the last years
in many places, regardless of the patients’ risk management decision.
On the other hand, in several countries, the amalgam is still
chosen for posterior teeth. In 2003, a research carried out in the
United Kingdom showed that 49% of dental surgeons used amalgam
instead of resin composites as restorative material. The main
reasons for choosing amalgam were its lower technical sensitivity
in procedures, higher resistance to tooth wear, lower cost for
patients, lower postoperative tooth sensitivity and higher clinical
longevity [15].
In some previous studies, it has been indicated that more extensive
resin composites restorations tend to cause more fractures
than amalgam and amalgam restorations may present satisfactory
clinical performance for more than 12 years [8]. Nevertheless, in
relation to their clinical longevity, their great performance and
success rate is well established [2]. Thus, amalgam is still a great
option for some clinical cases. Despite its limited indication for
posterior teeth and non- aesthetical anterior areas, its use is very
important when treating special patients. In the case of elderly
people, the use of amalgam can restore large tooth substance
losses with simple procedures and low cost. The same reasons
make it the preferred material for patients at high risk to dental
caries [13], like adolescents. It presents excellent performance for
occlusal cavities of pits and fissures and can help with chewing
for many years. The amalgam is an adequate solution for the cervical
area of posterior teeth, as it can be well polished and tolerate
gingival tissues. In the anterior teeth, it can also restore the lingual
face with remarkable advantages for patients that are more likely
to have cavities in the cingulum. Caries lesions in the cementum
area, which are a serious clinical problem, will be a source of relief
for the dentist and the patient alike because they are easy to
restore, as well as the restorative properties and the longevity of
the amalgam.
Certain studies were done in the institution on root canal fractures,
root canal irrigation [16-19]. In vitro studies and systematic
review on storage media for avulsed tooth were also carried out.
[17, 20-22]. Researches such as clinical performance of various
cements in noncarious cervical lesion and advancement in LA and
veneers were also conducted in the institution [23-26]. Various
studies such as questionnaire based study and an invivo study on
diagnostic tests for pulp vitality were also done in the institution.
[27-30] The present study aims to evaluate the association between
age and gender of patients who underwent amalgam class
II restoration in mandibular first molar.
This study is a single-center retrospective study, carried out in
the Department of Conservative and endodontic dentistry at the
SDC. Our study was approved by the ethical board of Saveetha
dental college – Institutional ethical committee [IEC]. Ethical approval
number SDC/SIHEC/2020/DIASDATA/0619-0320. All
available records of endodontic patients treated from June 2019
– April 2020, were examined and included in our data collection.
A total of 154 case sheets were reviewed. Cross verification of
data for error was done by presence of additional reviewers and
by photographs evaluation. Simple random sampling was done
to minimise sampling bias. It was generalised to the south indian
population. Two examiners were involved in the study.
Acquisition of data was done from the hospital digital database
which records all patient details. The data were entered in the system
in a methodical manner. For this study, Data on the number
of patients underwent amalgam class II restoration in mandibular
first molar and clinical variables such as gender, and age at the
start of treatment were collected. The data was then entered in excel manually and imported to SPSS for analysis. Incomplete or
censored data were excluded from the study.
Descriptive statistics were used to summarise the demographic
information of the patients included in this study. Descriptive
statistics is used for the acquisition of frequency of distribution
of the data.The number of patients underwent amalgam class II
restoration in mandibular first molar and clinical variables such
as gender, and age at the start of treatment were collected. For a
comparison between different variables, Statistical Package IBM
SPSS version 21.0 software analyser was used. The data was analyzed
using a chi- square test. The p value of less than 0.05 was
considered to be statistically significant. Risk analysis was also
done to interpret the study population.
Result and Discussion
Increasing number of amalgam class II restoration is done in 46
(50.65%) when compared to 36. (GRAPH 1) It is observed that
people of age group above 30 years(64.94%) have undergone
more amalgam class II restoration in the mandibular first molar
when compared to 18-30 years of age group. (GRAPH 2) The
graph shows that 50.65% of males and 49.35% of females have
undergone amalgam class II restoration in mandibular first molar.
From which it is observed that, males have undergone more
amalgam class II restoration in the mandibular first molar when
compared to females. (GRAPH 3) It is observed that females
(25.32%) have undergone more amalgam class II restoration in
36 than males (24.03%). The male population(26.62%) have undergone
more amalgam class II restoration in 46 than the female
population(24.03%). (GRAPH 4) Between the age group 18-30
years(green) 16.23% of them have undergone amalgam class II restoration in 36 and 18.83% of them have undergone amalgam
class II restoration in 46. Above 30 years of age group(yellow)
33.12% of them have undergone amalgam class II restoration in
36 and 31.82% of them have undergone amalgam class II restoration
in 46. From the chart it is observed that patients above 30
years of age group have undergone more amalgam class II restoration
in mandibular first molar. (GRAPH 5) Risk analysis was
also done to interpret the study population. It is observed that
males have higher risk when compared to females with highest
confidence interval 1.490 and lowest confidence interval 0.785.
(TABLE 1)
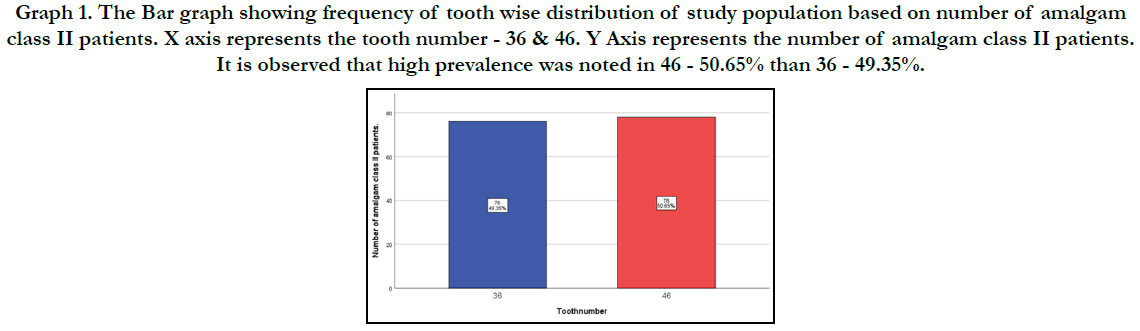
Graph 1. The Bar graph showing frequency of tooth wise distribution of study population based on number of amalgam class II patients. X axis represents the tooth number - 36 & 46. Y Axis represents the number of amalgam class II patients. It is observed that high prevalence was noted in 46 - 50.65% than 36 - 49.35%.
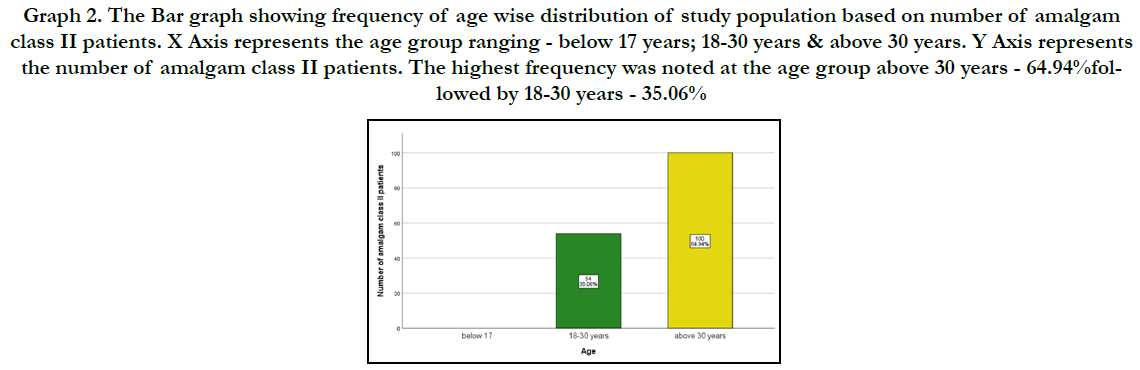
Graph 2. The Bar graph showing frequency of age wise distribution of study population based on number of amalgam class II patients. X Axis represents the age group ranging - below 17 years; 18-30 years & above 30 years. Y Axis represents the number of amalgam class II patients. The highest frequency was noted at the age group above 30 years - 64.94%followed by 18-30 years - 35.06%
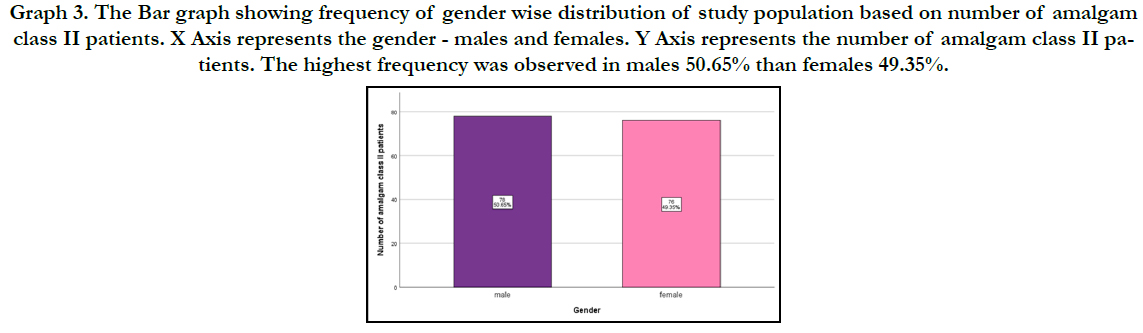
Graph 3. The Bar graph showing frequency of gender wise distribution of study population based on number of amalgam class II patients. X Axis represents the gender - males and females. Y Axis represents the number of amalgam class II patients. The highest frequency was observed in males 50.65% than females 49.35%.
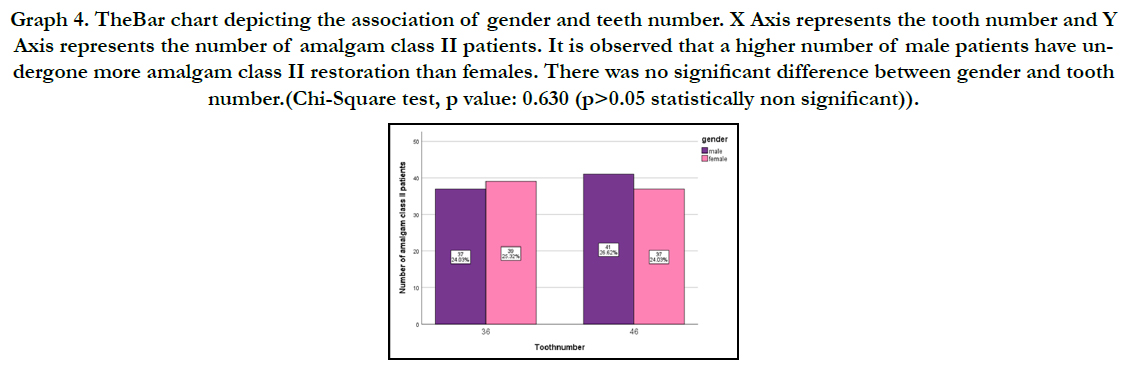
Graph 4. TheBar chart depicting the association of gender and teeth number. X Axis represents the tooth number and Y Axis represents the number of amalgam class II patients. It is observed that a higher number of male patients have undergone more amalgam class II restoration than females. There was no significant difference between gender and tooth number.(Chi-Square test, p value: 0.630 (p>0.05 statistically non significant)).
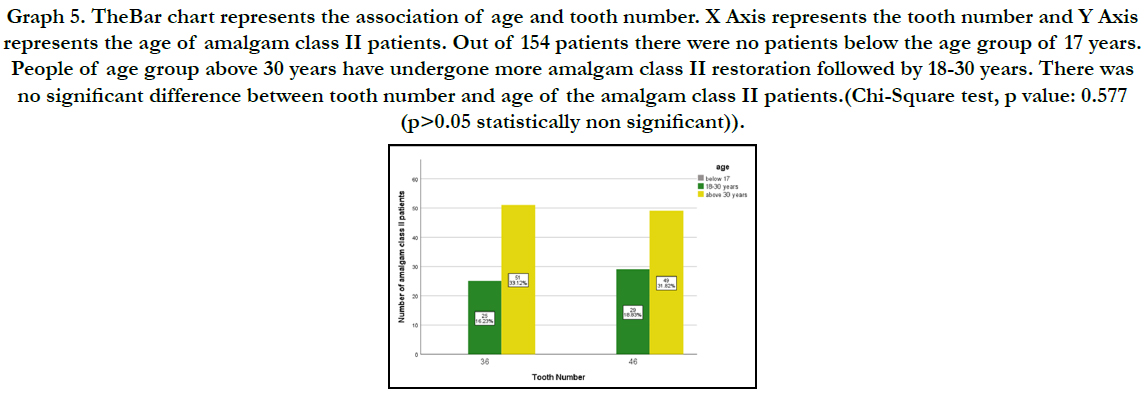
Graph 5. TheBar chart represents the association of age and tooth number. X Axis represents the tooth number and Y Axis represents the age of amalgam class II patients. Out of 154 patients there were no patients below the age group of 17 years. People of age group above 30 years have undergone more amalgam class II restoration followed by 18-30 years. There was no significant difference between tooth number and age of the amalgam class II patients.(Chi-Square test, p value: 0.577 (p>0.05 statistically non significant)).
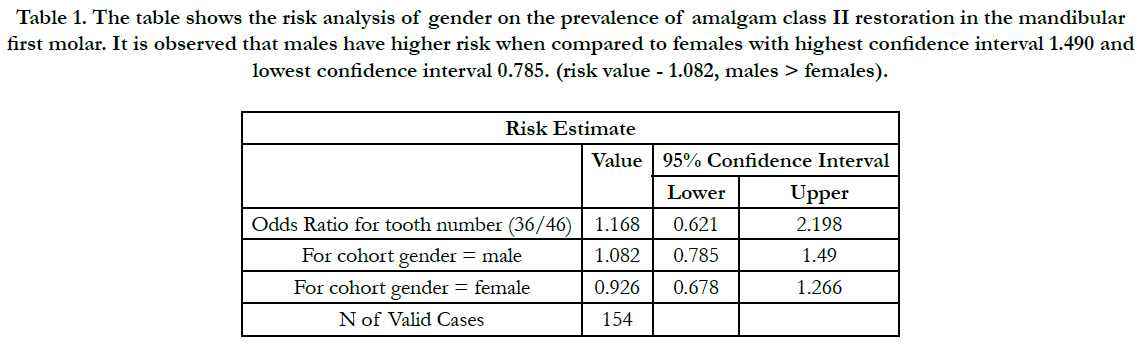

Table 1. The table shows the risk analysis of gender on the prevalence of amalgam class II restoration in the mandibular first molar. It is observed that males have higher risk when compared to females with highest confidence interval 1.490 and lowest confidence interval 0.785. (risk value - 1.082, males > females).
In this study male population had more prevalence of class II dental caries. This can be attributed to poor usage of interdental brush/ other cleaning aid. A study by yamamoto et al states that interdental brushes or other interdental cleaning aids can reduce caries incidence in proximal surfaces of the teeth [31]. bharti et al stated that the use of amalgam can be continued as a material of choice if esthetics is not a concern [6].
In some previous studies, it has been indicated that more extensive resin composites restorations tend to cause more fractures than amalgam and amalgam restorations may present satisfactory clinical performance for more than 12 years [32]. Amalgam restorations are also likely to fail in the daily practice. According to Healy and Phillips, the failures can be attributed to the preparation of cavities (56%) and incorrect manipulation of the material, while only 4% of those failures have been associated with other factors. Despite the long history and popularity of dental amalgam as a restorative material, there have been periodic concerns regarding the potential adverse health effects arising from exposure to mercury in amalgam. In this study, the age group of 18-30 years have more class II Cries and have undergone class II amalgam restoration. This can be overcome by usage of proper cleaning technique, Imai et al stated that interdental brush is easy to use and has high patient compliance [33]. Thus it is important to educate the patient on the same.
In a study by kilpatrick et al [34] he stated that Amalgam remains an appropriate choice of material for the restoration and also added that the factors other than durability are increasingly influencing its use in clinical practice. The pros of the study includes, flexibility of the study, less time consumption and accessibility. The cons of the study are limitations in the population group. Future studies should focus on various factors that influence amalgam class II restoration in conservative dentistry, larger sample size on varied population and long term follow up is needed.
Conclusion
Within the limitations the age group 18-30 years underwent more
amalgam class II restoration in the mandibular first molar. The
Male population seem to have undergone more amalgam class II
restoration in the mandibular first molar. There is no significant
association between the gender and age group with amalgam class
II restoration in the mandibular first molar.
Authors Contribution
First author, sandhya performed the data collection by reviewing
patient details, filtering required data, analysing and interpreting
statistics and contributed to manuscript writing.
Second author, Dr. Surendar contributed to conception of study
title, study design, analysed the collected data, statistics and interpretation
and also critically revised the manuscript.
Third author, Dr. SenthilMuruganP participated in the study and
revised the manuscript. All the three authors have discussed the
results and contributed to the final manuscript.
Acknowledgement
This research was supported by saveetha dental college and hospital.
We thank the department of Conservative and Endodontic
Dentistry, Saveetha Dental College for providing insight and expertise
that greatly assisted this research.
References
- Adinda C, Tedjosasongko U, Wibowo TB. Usiasaatinisialakuisisi Streptococcus mutansdanjumlaherupsigigisulungpadaanak (Initial acquisition age of Mutans Streptococci and number of erupted primary teeth in children). Dental Journal (MajalahKedokteran Gigi). 2014 Dec 1;47(4):202-5.
- Caufield PW. Dental caries--a transmissible and infectious disease revisited: a position paper. Pediatr Dent. 1997 Nov-Dec;19(8):491-8. PubmedPMID: 9442545.
- Caufield PW. Dental caries: an infectious and transmissible disease where have we been and where are we going? N Y State Dent J. 2005 Mar;71(2):23– 7.PubmedPMID:15887465.
- Saini S, Aparna, Gupta N, Mahajan A, Arora DR. Microbial flora in orodental infections. Indian J Med Microbiol. 2003 Apr;21(2):111–4.PubmedPMID: 17642993.
- Berg JH. The marketplace for new caries management products: dental caries detection and caries management by risk assessment. BMC Oral Health. 2006 Jun 15;6Suppl 1(Suppl 1):S6. PubmedPMID: 16934123.
- Bharti R, Wadhwani KK, Tikku AP, Chandra A. Dental amalgam: An update. J Conserv Dent. 2010 Oct;13(4):204-8. PubmedPMID: 21217947.
- Osborne JW, Norman RD. 13-year clinical assessment of 10 amalgam alloys. Dent Mater. 1990 Jul;6(3):189-94. PubmedPMID: 2086293.
- . Letzel H, van 't Hof MA, Marshall GW, Marshall SJ. The influence of the amalgam alloy on the survival of amalgam restorations: a secondary analysis of multiple controlled clinical trials. J Dent Res. 1997 Nov;76(11):1787-98. PubmedPMID: 9372797.
- Berry TG, Osborne JW. Effect of zinc in two non-gamma-2 dental amalgam systems. Dent Mater. 1985 Jun;1(3):98-100. PubmedPMID: 3861439.
- . Sarkar NK, Park JR. Mechanism of improved corrosion resistance of Zncontaining dental amalgams. J Dent Res. 1988 Oct;67(10):1312-5. PubmedPMID: 3170886.
- McDonald A. Advances and fixed in operative dentistry prosthodontics. Primary Dental Care. 2001 Jan 1;8(1):13-6.
- Alcaraz MGR, Graciela Rasines Alcaraz M, Veitz-Keenan A, Sahrmann P, Schmidlin PR, Davis D, et al. Direct composite resin fillings versus amalgam fillings for permanent or adult posterior teeth [Internet]. Cochrane Database Syst Rev. 2014 Mar 31;(3):CD005620.Pubmed PMID: 24683067.
- Rw P. Science of dental materials. 9thedn,WB. Sauders Co, Philadelphia; 1991. pp. 61-67.
- Mitchell RJ, Koike M, Okabe T. Posterior amalgam restorations--usage, regulation, and longevity. Dent Clin North Am. 2007 Jul;51(3):573-89. PubmedPMID: 17586144.
- Burke FJ, McHugh S, Hall AC, Randall RC, Widstrom E, Forss H. Amalgam and composite use in UK general dental practice in 2001. Br Dent J. 2003 Jun 14;194(11):613-8.PubmedPMID: 12819697.
- Ramamoorthi S, Nivedhitha MS, Divyanand MJ. Comparative evaluation of postoperative pain after using endodontic needle and EndoActivator during root canal irrigation: A randomised controlled trial. AustEndod J. 2015 Aug;41(2):78-87. PubmedPMID: 25195661.
- Siddique R, Jayalakshmi S. Assessment of Precipitate Formation on Interaction of Chlorhexidine with Sodium Hypochlorite, Neem, Aloevera and Garlic: An in vitro Study. Indian Journal of Public Health Research & Development. 2019 Nov 1;10(11).
- Ramanathan S, Solete P. Cone-beam Computed Tomography Evaluation of Root Canal Preparation using Various Rotary Instruments: An in vitro Study. The journal of contemporary dental practice. 2015 Nov 1;16(11):869-72.
- Teja KV, Ramesh S, Priya V. Regulation of matrix metalloproteinase-3 gene expression in inflammation: A molecular study. Journal of conservative dentistry: JCD. 2018 Nov;21(6):592.
- Rajakeerthi R, Ms N. Natural Product as the Storage medium for an avulsed tooth–A Systematic Review. Cumhuriyet Dental Journal. 2019;22(2):249- 56.
- Rajendran R, Kunjusankaran RN, Sandhya R, Anilkumar A, Santhosh R, Patil SR. Comparative Evaluation of Remineralizing Potential of a Paste Containing Bioactive Glass and a Topical Cream Containing Casein Phosphopeptide- Amorphous Calcium Phosphate: An in Vitro Study. Pesquisa- BrasileiraemOdontopediatria e ClínicaIntegrada. 2019;19.
- Kumar D, Canal DP. Negotiation-A Review [Internet]. Vol. 11. Research Journal of Pharmacy and Technology. 2018:3727.
- Nasim I, Hussainy S, Thomas T, Ranjan M. Clinical performance of resinmodified glass ionomer cement, flowable composite, and polyacidmodified resin composite in noncarious cervical lesions: One-year follow-up [Internet]. Vol. 21. Journal of Conservative Dentistry. 2018;21:510.
- Baskran RN, Pradeep S. Recent advancement of local anasthesia advancement to recent advancement of local anaesthesia administration. Research Journal of Pharmacy and Technology. 2016;9(10):1761-4.
- Ravinthar K. Recent advancements in laminates and veneers in dentistry. Research Journal of Pharmacy and Technology. 2018;11(2):785-7.
- Nasim I, Nandakumar M. Comparative evaluation of grape seed and cranberry extracts in preventing enamel erosion: An optical emission spectrometric analysis [Internet]. Vol. 21. Journal of Conservative Dentistry. 2018:516.
- Noor SS, Shihaab SS. Pradeep. Chlorhexidine: Its properties and effects [Internet]. Vol. 9. Research Journal of Pharmacy and Technology. 2016:1755.
- Jose J, P. A, Subbaiyan H. Different Treatment Modalities followed by Dental Practitioners for Ellis Class 2 Fracture – A Questionnaire-based Survey [Internet].The Open DentistryJournal. 2020; 14: 59–65.
- Janani K, Palanivelu A, Sandhya R. Diagnostic accuracy of dental pulse oximeter with customized sensor holder, thermal test and electric pulp test for the evaluation of pulp vitality: an in vivo study. Brazilian Dental Science. 2020 Jan 31;23(1):8-p.
- Manohar MP, Sharma S. A survey of the knowledge, attitude, and awareness about the principal choice of intracanal medicaments among the general dental practitioners and nonendodontic specialists. Indian Journal of Dental Research. 2018 Nov 1;29(6):716. .
- Yamamoto N, Hasegawa K, Sueda T, Kinoshita S. The effects of interdental brush and dental floss in the reduction of interdental plaque (author's transl). Nihon ShishubyoGakkaikaishi. 1975 Sep;17(2):258-64.
- Opdam NJ, Bronkhorst EM, Loomans BA, Huysmans MC. 12-year survival of composite vs. amalgam restorations. Journal of dental research. 2010 Oct;89(10):1063-7.
- Hennequin‐Hoenderdos NL, Van der Sluijs E, van der Weijden GA, Slot DE. Efficacy of a rubber bristles interdental cleaner compared to an interdental brush on dental plaque, gingival bleeding and gingival abrasion: A randomized clinical trial. International Journal of Dental Hygiene. 2018 Aug;16(3):380-8.
- Kilpatrick NM, Neumann A. Durability of amalgam in the restoration of class II cavities in primary molars: a systematic review of the literature. European Archives of Paediatric Dentistry. 2007 Mar 1;8(1):5-13.





