Knowledge, Attitude and Practice Regarding Ankyloglossia in Children among Undergraduate Dental Students. - A Questionnaire Survey
V. J. Oviya1, Geo Mani2*, Deepa Gurunathan3
1 Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
2 Reader, Department of Pedodontics and Preventive Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
3 Professor and Head, Department of Pedodontics and Preventive Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
*Corresponding Author
Geo Mani,
Reader, Department of Pedodontics and Preventive Dentistry, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University,
Chennai, 600077, India.
E-mail: geomani.sdc@saveetha.com
Received: July 08, 2019; Accepted: August 03, 2019; Published: August 08, 2019
Citation: V. J. Oviya, Geo Mani, Deepa Gurunathan. Knowledge, Attitude and Practice Regarding Ankyloglossia in Children among Undergraduate Dental Students. - A Questionnaire Survey. Int J Dentistry Oral Sci. 2020;7(10):923-930. doi: dx.doi.org/10.19070/2377-8075-20000183
Copyright: Geo Mani© 2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Ankyloglossia or tongue tie is a congenital anomaly in which lingual frenulum is attached to the tongue and restricts its normal
movements. This hinders normal functions and affects the quality of life. Though there are conflicts in the management of this
anomaly, diagnosis is essential at an earlier age. Hence, this study is to analyse the knowledge and attitude of ankyloglossia in
children among dental undergraduates. A questionnaire study was conducted among randomly chosen 100 undergraduate dental
students. It consisted of questions regarding the knowledge, attitude and practice regarding ankyloglossia in children. The data was
collected and analysed through IBM SPSS statistical analysis. Descriptive statistics were done. Percentages and frequencies were
calculated and to test difference among variables chi square test was done with a p value <0.05 considered statistically significant.
In this study, about 96% of the students reported to know about ankyloglossia. Among them, only 57% have reported to come
across a patient with ankyloglossia. Only 70% of the students have been checking ankyloglossia during clinical examination in
every patient. About 79% of the students were aware of the treatment measures. Hence, this study concludes that dental undergraduates
had adequate knowledge on ankyloglossia within children.
2.Introduction
3.Materials and Method
4.Results and Discussion
5.Conclusion
6.Acknowledgement
7.References
Keywords
Ankyloglossia; Tongue Tie; Dental Undergraduates; Breastfeeding; Children.
Introduction
A frenulum is a small muscle, which is covered by a mucous membrane
and attaches the lips and tongue to the bones of the mouth.
Occasionally, considerable variations can occur in normal shape,
position of frenum [1]. The main function is to keep the lips and
tongue in harmony with the growing bone of the mouth during
foetal development. The tongue is usually short or even has a
bifid tip during birth with frenulum extending to the tip. Eventually,
it gets receded within 6 months to 6 years of life. Persistence
of this lingual frenum causes an anatomical abnormality called
Ankyloglossia [2].
Ankyloglossia otherwise referred to as tongue tie, is a congenital
anomaly which may decrease the mobility of the tongue. It is
characterised by an abnormally short, thickened or tight lingual
frenulum connecting the underside of the tongue to the floor of
the mouth [3]. Ankyloglossia varies in degree of severity from
mild cases presented with mucous membrane bands to complete
ankyloglossia in which the tongue is restrained to the floor of the
mouth [4].
Though ankyloglossia is uncommon, it's not rare. Ankyloglossia
can cause various problems such as difficulties in breastfeeding,
speech impediments, poor oral hygiene and being embarrassed by
peers during childhood and adolescents [5].
Ankyloglossia can be treated by frenectomy where the frenulum
is cut off with or without the consciousness by using local anaesthesia
[6]. These are usually performed by dentists, with quick
procedures which may rarely cause serious complications such as
scarring, infections etc [7].
There has been a controversy going on in the diagnosis and treatment
of ankyloglossia. Though there is an increase in the number
of frenectomy procedures, there are still variations in the outcome
of the treatment. Untreated ankyloglossia can cause breastfeeding
problems, due to the difficulty in latching, sucking and swallowing.
This results in loss of protective immunity for the child which
may even cause cognitive loss [8].
Hence detecting ankyloglossia in the early stage of the child’s life
is the primary step in the further management, either surgical or
psychological approach for improving the future of the child.
Dental undergraduates play a vital role in the detection of ankyloglossia
as they may come across such anomalies, when they clinically
evaluate every patient. Knowledge and treatment measures
should be well versed among dental undergraduates for the management
of ankyloglossia. Only limited studies have been done
among dentists regarding the awareness of Ankyloglossia.
Previously our team has conducted numerous cross sectional
studies [9-13], clinical trials [14-18], in-vitro studies [19, 20], case
studies [21] and literature reviews [22, 23] over the past 5 years.
Hence, this time, an attempt has been made to evaluate the knowledge,
awareness and attitude of dental undergraduates studying at
a University in Chennai regarding the ankyloglossia in Children.
A cross sectional questionnaire based study was carried out
among dental undergraduates of a University in Chennai who are
practising in clinics.
This study was conducted in an online setting. A total of 100 dental
undergraduates were chosen. Simple random sampling methodology
was employed, till the sample size was achieved.
Randomly selected students who are practising in clinics, till the
sample size was achieved.
All the postgraduates and students who were not attending any
clinics were excluded.
Those who were not willing to participate were excluded too.
Informed consent was obtained from all the participants before
conducting the study. Ethical clearance was obtained from the
Institutional Ethical Committee and Scientific Review Board of
the University.
A standard questionnaire was prepared. It was validated through conducting a pilot study among the subset of the study population.
It is then mailed to randomly chosen 100 dental undergraduates.
The questionnaire consisted of 3 parts. The first part
of the questionnaire consisted of participants' data such as age,
gender, year of study for the identification purpose. The second
portion consisted of questions regarding their knowledge of ankyloglossia
and its effects on patients. The third section consisted
of questions regarding their attitude and practice towards clinical
examination and treatment measures. The positive response came
from all the students with the response rate of 100%.
The data from their response were entered in the excel sheets.
The analysis was done using SPSS software through frequency
tests and Chi-square tests.
Results and Discussion
Out of 100, 35 males and 65 females participated in this study
(Table 1). All the participants belong to the age group ranging 19-
24 with the mean age of 21.64 (Table 2). Among them, 18% were
3rd years, 20% were final years and 64% were interns who are
studying and practising in the clinics (Table 3). In this study, 96%
were aware of ankyloglossia (Graph 1) and 85% of the participants
were aware that it is a congenital anomaly (Graph 2). About
87% of the students are aware of its effect in interfering breast
feeding (Graph 3) and 85% aware about its effect in affecting
speech of the child (Graph 4). Among them, 80% of the students
were aware of the treatment measures of ankyloglossia (Graph
5). In this study, among 100 students, only 57% of the students
have come across a patient with ankyloglossia (Graph 6). About
70% of the participants reported that they check for tongue tie in
every patient during clinical examination (Graph 7). About 85%
of the students reported that tongue tie should be treated at an
earlier age (Graph 8). About 79% of the students agreed that this
ankyloglossia in children causes psychological problems (Graph
9) and about 82% of the students reported that if ankyloglossia
left untreated may cause eating difficulty in children (Graph 10) In
this study, about 51% of the students strongly agreed and about
39% of the students agreed it is inevitable to check for abnormalities
in every dental checkup (Graph 11). In this study, 100%
of the male students gave positive responses and no negative responses
were reported. About 6.15% of the negative responses
were noted among females students, however this finding was not
statistically significant (Graph 12). There was no significant difference
in the knowledge among students of different years of study
and with gender (Graph 13).
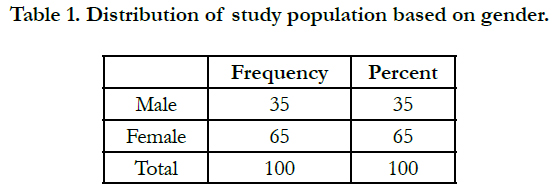

Table 1. Distribution of study population based on gender.
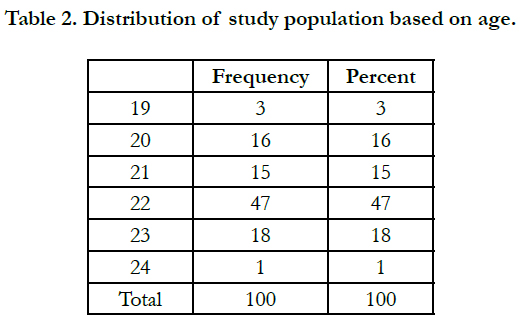
Table 2. Distribution of study population based on age.
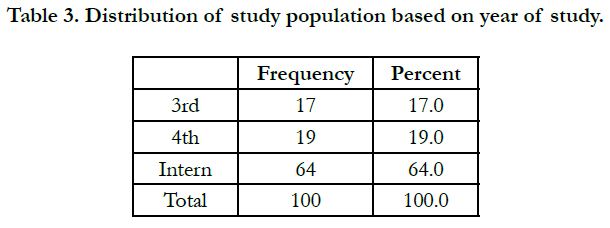
Table 3. Distribution of study population based on year of study.
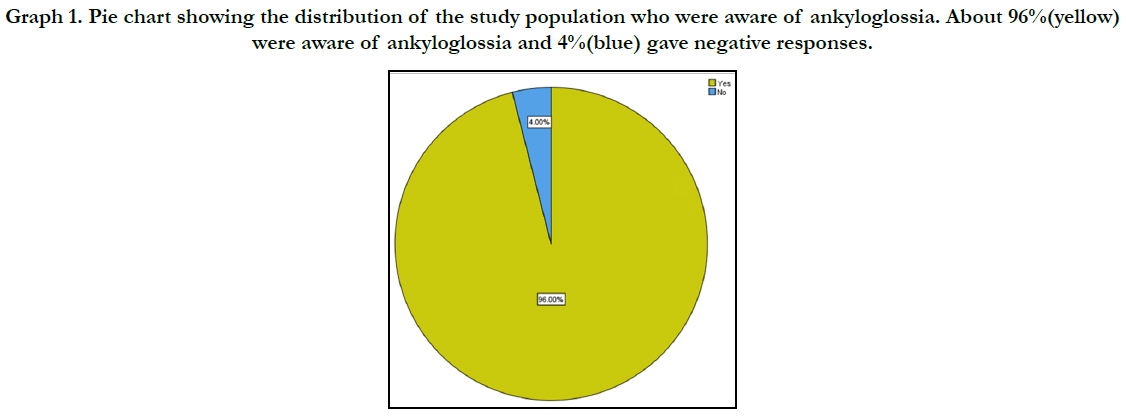

Graph 1. Pie chart showing the distribution of the study population who were aware of ankyloglossia. About 96%(yellow) were aware of ankyloglossia and 4%(blue) gave negative responses.
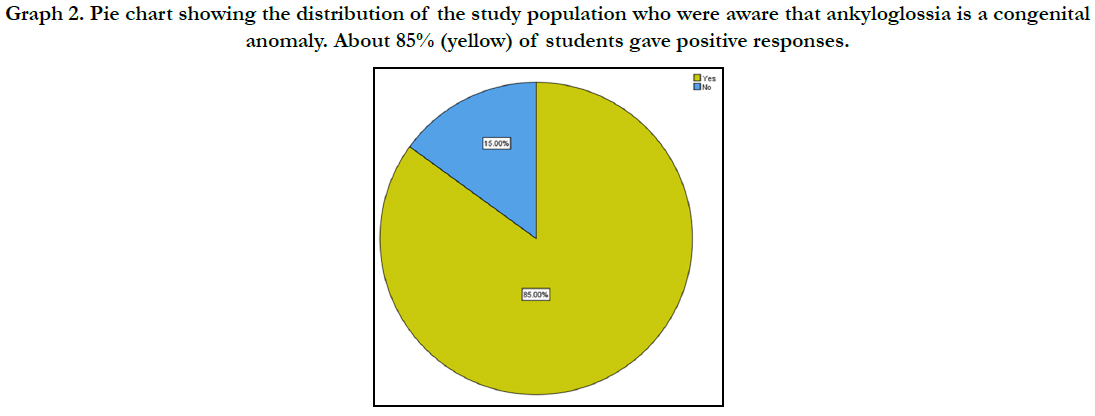

Graph 2. Pie chart showing the distribution of the study population who were aware that ankyloglossia is a congenital anomaly. About 85% (yellow) of students gave positive responses.
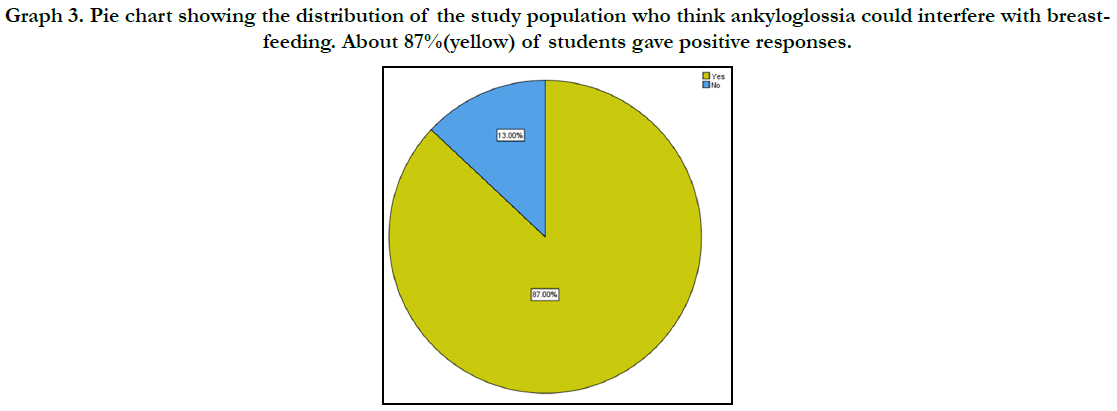

Graph 3. Pie chart showing the distribution of the study population who think ankyloglossia could interfere with breastfeeding. About 87%(yellow) of students gave positive responses.
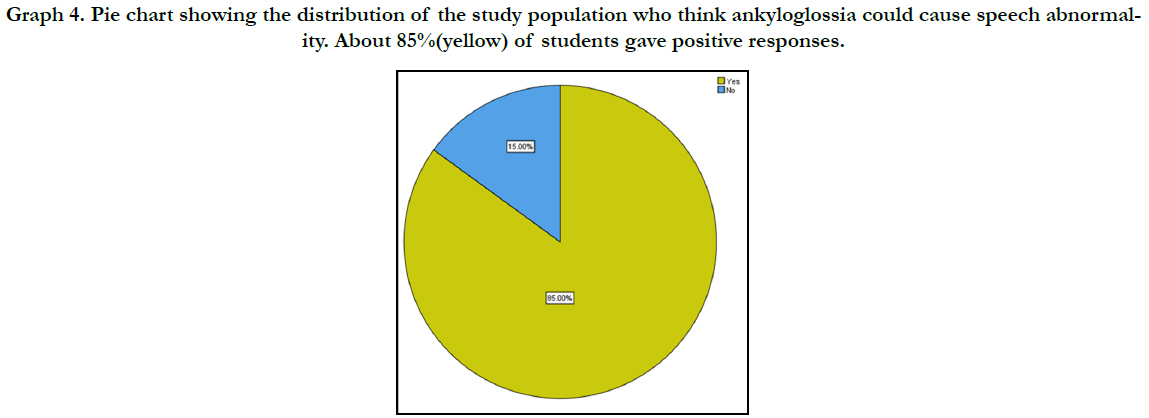

Graph 4. Pie chart showing the distribution of the study population who think ankyloglossia could cause speech abnormality. About 85%(yellow) of students gave positive responses.
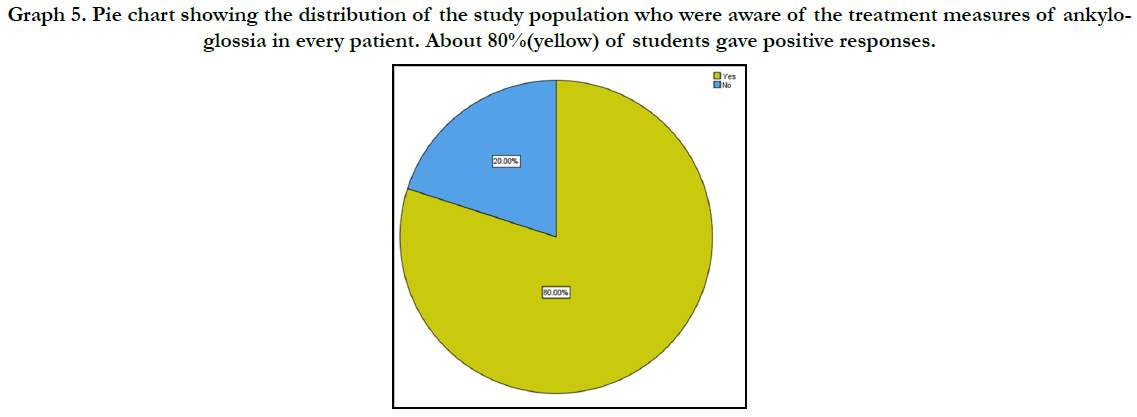

Graph 5. Pie chart showing the distribution of the study population who were aware of the treatment measures of ankyloglossia in every patient. About 80%(yellow) of students gave positive responses.
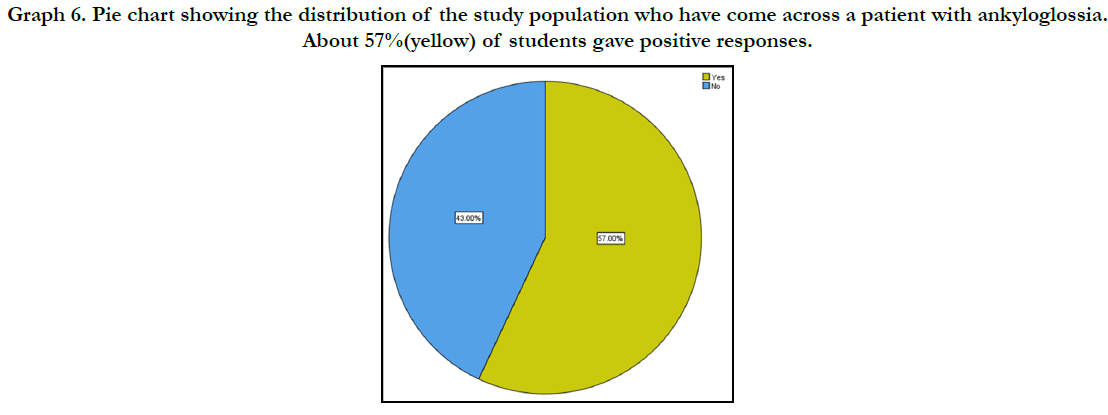

Graph 6. Pie chart showing the distribution of the study population who have come across a patient with ankyloglossia. About 57%(yellow) of students gave positive responses.
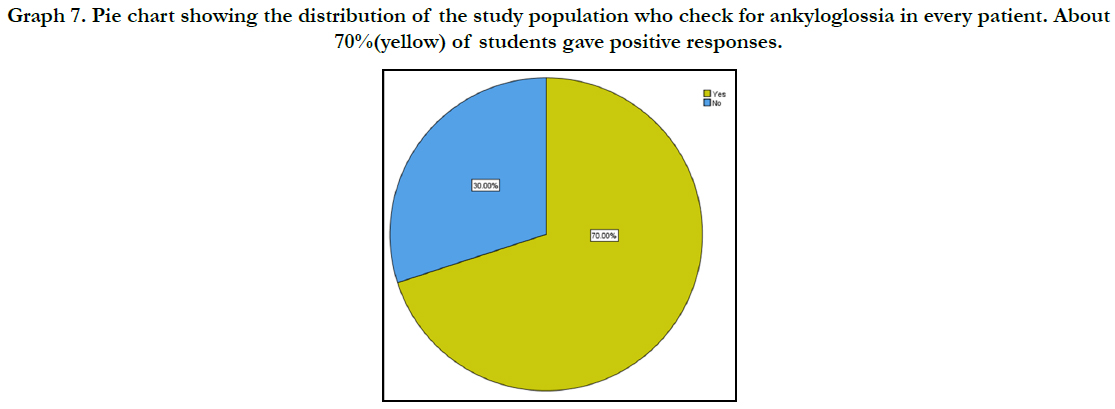

Graph 7. Pie chart showing the distribution of the study population who check for ankyloglossia in every patient. About 70%(yellow) of students gave positive responses.
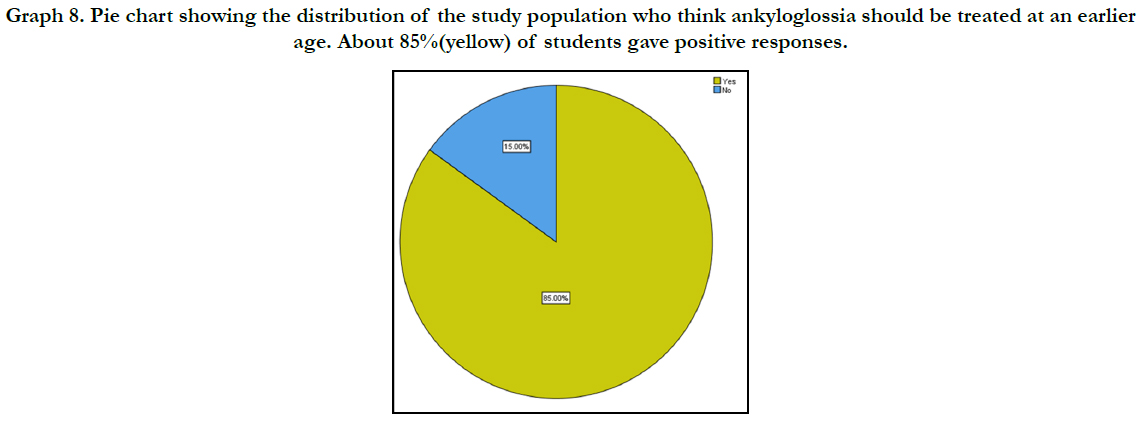

Graph 8. Pie chart showing the distribution of the study population who think ankyloglossia should be treated at an earlier age. About 85%(yellow) of students gave positive responses.
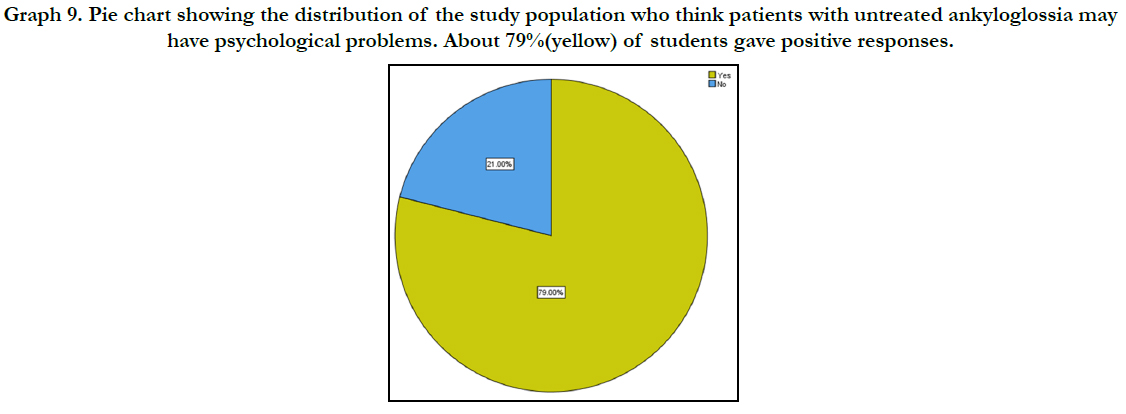

Graph 9. Pie chart showing the distribution of the study population who think patients with untreated ankyloglossia may have psychological problems. About 79%(yellow) of students gave positive responses.
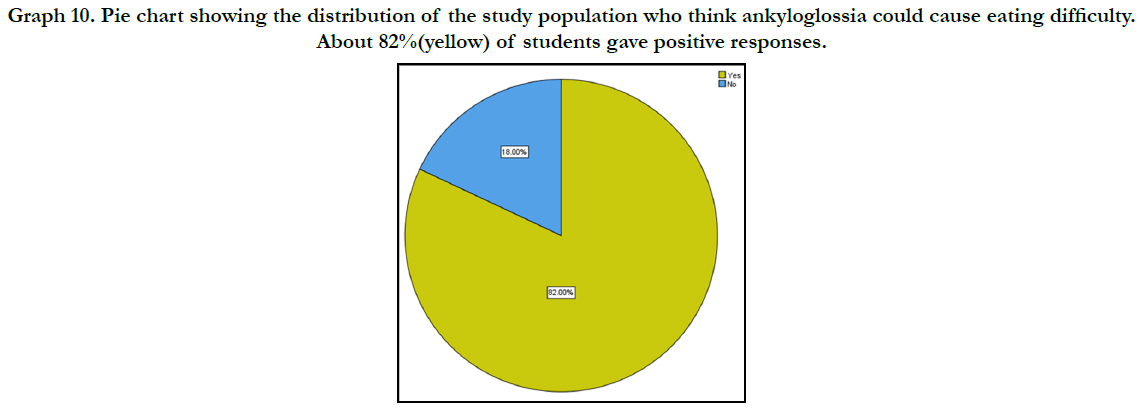

Graph 10. Pie chart showing the distribution of the study population who think ankyloglossia could cause eating difficulty. About 82%(yellow) of students gave positive responses.
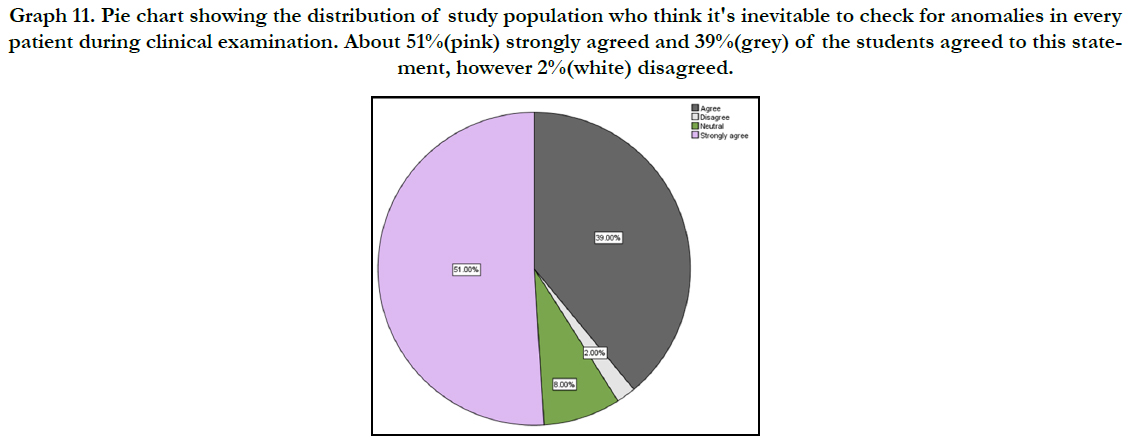

Graph 11. Pie chart showing the distribution of study population who think it's inevitable to check for anomalies in every patient during clinical examination. About 51%(pink) strongly agreed and 39%(grey) of the students agreed to this statement, however 2%(white) disagreed.
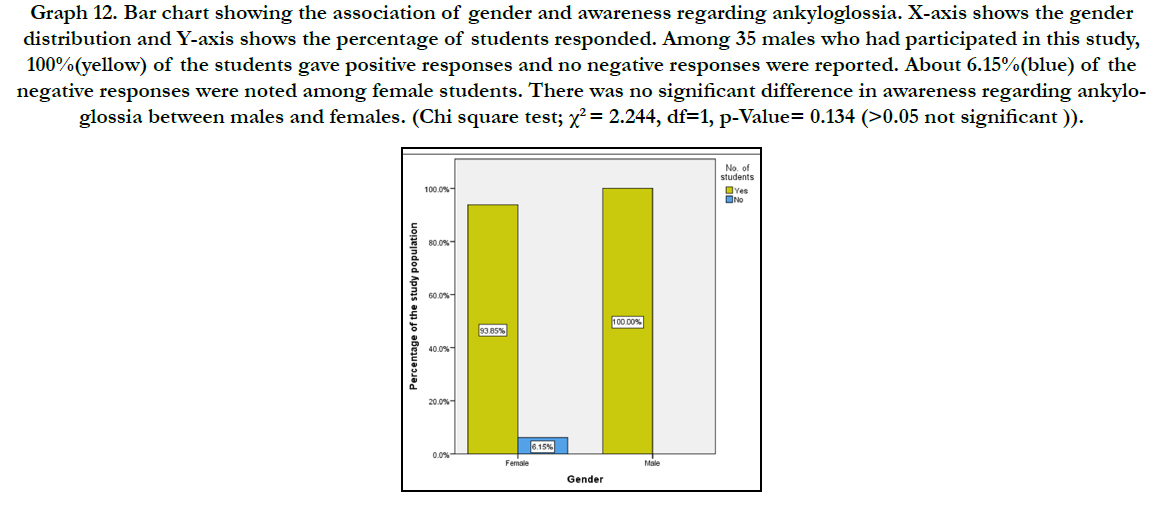

Graph 12. Bar chart showing the association of gender and awareness regarding ankyloglossia. X-axis shows the gender distribution and Y-axis shows the percentage of students responded. Among 35 males who had participated in this study, 100%(yellow) of the students gave positive responses and no negative responses were reported. About 6.15%(blue) of the negative responses were noted among female students. There was no significant difference in awareness regarding ankyloglossia between males and females. (Chi square test; χ2 = 2.244, df=1, p-Value= 0.134 (>0.05 not significant)).
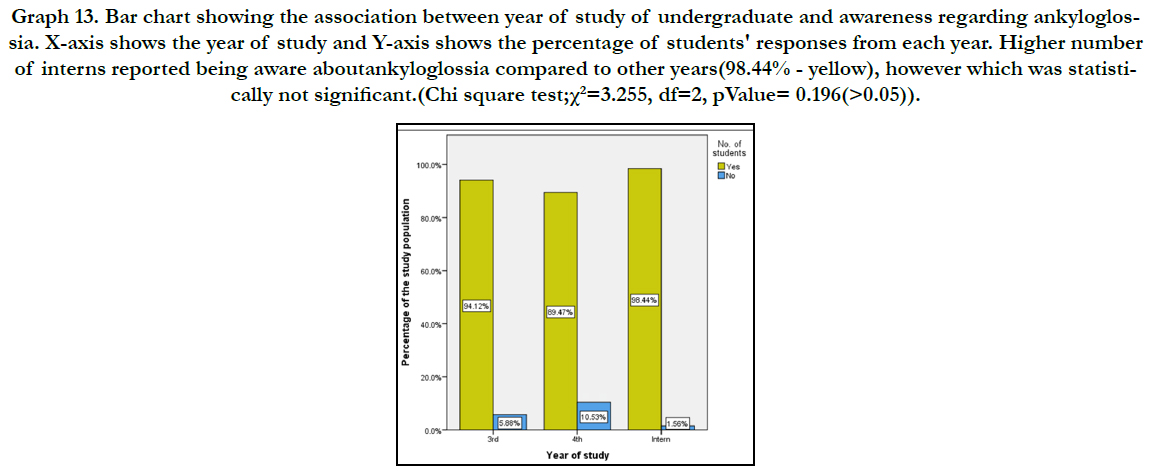

Graph 13. Bar chart showing the association between year of study of undergraduate and awareness regarding ankyloglossia. X-axis shows the year of study and Y-axis shows the percentage of students' responses from each year. Higher number of interns reported being aware aboutankyloglossia compared to other years(98.44% - yellow), however which was statistically not significant.(Chi square test;χ2=3.255, df=2, pValue= 0.196(>0.05)).
Tongue tie has been a much debatable topic due to various effects in the children with or without the treatment. Dentists along with pediatricians, otolaryngologists and lactation consultants plays a vital role in the diagnosis and management of ankyloglossia. The knowledge and awareness of ankyloglossia in children and its effects should be well versed among dentists. Hence this study was conducted among dental undergraduates who in the future get to treat patients with any other abnormality in the oral cavity.
In the present study, 96% of the students were aware of ankyloglossia and among them, 85% of the participants were aware about its congenital origin. Ankyloglossia occurs with increased rate in various congenital syndromes such as orofaciodigital syndrome, Simpson-Golabi-Behmel syndrome, Opitz syndrome, Beckwith-wiedemann syndrome, X-linked cleft palate [24].
In this study, 87% of the students were aware of the effects of tongue tie interference with breastfeeding. An infant with ankyloglossia has the difficulty in latching onto the nipple resulting in compression of the nipple against the gum pad which can lead to nipple pain. This may lead to switch feeding through bottle [25].
In this study, 79% of the undergraduates agreed that this anomaly in children causes psychological problems and 82% of the students reported that the children with ankyloglossia will face difficulty in eating food. A case study by Baxter et al., [26] reported that a child with ankyloglossia appeared shy and lacking confidence in communication with others and experienced selective eating and gagged on foods on various textures.
In the present study, 57% of the students have come across patients with ankyloglossia. Previous studies reported incidence vary widely from 0.02 to 5% [25]. It is more prevalent among neonates as the milder ones might get resolved with growth [27]. Messner et al28 reported higher prevalence in males with a ratio of 3:1.
About 80% of the students were aware of the treatment measures for ankyloglossia and 85% reported that it should be treated at an earlier age. A study by Jin et al., [29] reported variation between health care professionals in the treatment of ankyloglossia. This is due to varied and unclear outcomes in the treatment of ankyloglossia and its increased complications like damage to the anatomical structures. However, the untreated child may face various problems including speech, breastfeeding difficulties and it even affects the dentition with the need of orthodontic management.
Though few reports suggested the mechanism of breastfeeding in children with ankyloglossia is unclear, a study by Messner et al5 reported significant association between ankyloglossia and breastfeeding and concluded that there is a significant improvement in breastfeeding of children who had undergone surgical interventions. Dentists (35%) who participated in the study by Jin et al., [29] reported ankyloglossia as the cause of lactation difficulties.
In the present study, 85% of the students were aware of its effect in affecting speech of a child with ankyloglossia. Limited movement of the tongue for the increased period during childhood would affect the speech of the children. A study by Dollberg et al., [30] concluded that children who underwent frenectomy showed fewer articulation problems compared to the untreated children. But that study reported insignificant difference in the fluency and speech outcomes after the surgery. However Messner et al., [31] reported significant improvement in tongue mobility, protrusion, elevation and speech outcomes in his prospective study. A study conducted by Walls et al., [32] among the parents whose children underwent neonatal frenectomy concluded that improved speech outcomes and oral motor activities compared to individuals that declined surgical interventions. This is in accordance with the study conducted by Lalakea et al., [33] who reported similar findings. A study conducted by Qazi et al., [34] stated that 85% of dentists experienced alteration in the speech among patients with ankyloglossia.
In the present study, 70% of the students reported to check for ankyloglossia in every patient and 85% of the students agreed that it is a mandatory check for every other abnormality during the routine examination of the patients. Tongue is an important oral structure that affects speech, position of teeth, periodontal tissue, nutrition, swallowing, nursing and certain other social activities35. Hence, it is important for the dentists to regularly check for any abnormalities of the tongue and other oral structures regardless of its management.
An intervention is needed to improve the early detection of ankyloglossia due to its deleterious effect on the child’s quality of life. Hence, evaluating the knowledge, awareness and attitude of dentists about ankyloglossia, is a key step towards improving its management. Evaluating those data can immensely help in prevention and early diagnosis. The implementation of preventive measures such as dental counselling and social awareness programs will help to reduce delayed detection and its effects on child’s life. Based on the findings of this study, it can be concluded that the few dental undergraduates still lack sufficient knowledge and awareness regarding ankyloglossia in children. Their knowledge and attitude towards the ankyloglossia should be improved and updated to enable them to assess early diagnosis and provide treatment for this anomaly.
The main limitation of this study was limited sample size and it
was confined to limited geographical locations. For further scope
of the study increased sample size with inclusion of larger geographical
location would give better results.
Conclusions
Ankyloglossia affects a considerable number of infants and children.
It is important for the dentist to get accurate information
regarding its procedure and complications. In this study, majority
of the students were found to have adequate knowledge and
awareness of its effects, but however, a small group of the population
were found to be unaware and didn’t have enough knowledge
about ankyloglossia. Future actions with a view to improve
the knowledge and practice of dental students concerning the
management of ankyloglossia seems to be needed.
Acknowledgement
I sincerely express my gratitude and acknowledgement to the
management for their support and also thank the Research and IT
department of Saveetha dental college for their affable assistance
in obtaining the data.
References
- Northcutt ME. The lingual frenum. J ClinOrthod. 2009 Sep;43(9):557-65.
- Francis DO, Krishnaswami S, McPheeters M. Treatment of ankyloglossia and breastfeeding outcomes: a systematic review. Pediatrics. 2015 Jun 1;135(6):e1458-66.
- Ruffoli R, Giambelluca MA, Scavuzzo MC, Bonfigli D, Cristofani R, Gabriele M, et al. Ankyloglossia: a morphofunctional investigation in children. Oral Dis. 2005 May;11(3):170-4.Pubmed PMID: 15888108.
- Horton CE, Crawford HH, Adamson JE, Ashbell TS. Tongue-tie. Cleft Palate J. 1969 Jan 1;6(8):8-23.
- Messner AH, Lalakea ML. Ankyloglossia: controversies in management. Int. J. Pediatr. Otorhinolaryngol. 2000 Aug 31;54(2-3):123-31.
- Overview | Division of ankyloglossia (tongue-tie) for breastfeeding | Guidance | NICE. [cited 2020 Jun 13]; Available from: https://www.nice.org.uk/ guidance/ipg149
- Brinkmann S, Reilly S, Meara JG. Management of tongue-tie in children: a survey of paediatric surgeons in Australia. J Paediatr Child Health. 2004 Nov;40(11):600-5.Pubmed PMID: 15469527.
- Horta BL, Loret de Mola C, Victora CG. Breastfeeding and intelligence: a systematic review and meta-analysis. ActaPaediatr. 2015 Dec;104(467):14- 9.Pubmed PMID: 26211556.
- Govindaraju L, Jeevanandan G, Subramanian EM. Knowledge and practice of rotary instrumentation in primary teeth among Indian dentists: a questionnaire survey. J Int Oral Health. 2017 Mar 1;9(2):45.
- Ravikumar D, Jeevanandan G, Subramanian EM. Evaluation of knowledge among general dentists in treatment of traumatic injuries in primary teeth: A cross-sectional questionnaire study. Eur. J. Dent. 2017 Apr;11(2):232-7.
- Christabel SL, Gurunathan D. Prevalence of type of frenal attachment and morphology of frenum in children, Chennai, Tamil Nadu. World J Dent. 2015 Oct;6(4):203-7.
- Gurunathan D, Shanmugaavel AK. Dental neglect among children in Chennai. J Indian SocPedodPrev Dent. 2016 Oct 1;34(4):364-9.
- Govindaraju L, Gurunathan D. Effectiveness of Chewable Tooth Brush in Children-A Prospective Clinical Study. J ClinDiagn Res. 2017 Mar;11(3):ZC31-ZC34.Pubmed PMID: 28511505.
- Govindaraju L, Jeevanandan G, Subramanian EMG. Comparison of quality of obturation and instrumentation time using hand files and two rotary file systems in primary molars: A single-blinded randomized controlled trial. Eur J Dent. 2017 Jul-Sep;11(3):376-379.Pubmed PMID: 28932150.
- Jeevanandan G, Govindaraju L. Clinical comparison of Kedo-S paediatric rotary files vs manual instrumentation for root canal preparation in primary molars: a double blinded randomised clinical trial. Eur Arch Paediatr Dent. 2018 Aug;19(4):273-278.Pubmed PMID: 30003514.
- Govindaraju L, Jeevanandan G, Subramanian E. Clinical Evaluation of Quality of Obturation and Instrumentation Time using Two Modified Rotary File Systems with Manual Instrumentation in Primary Teeth. J ClinDiagn Res. 2017 Sep;11(9):ZC55-ZC58.Pubmed PMID: 29207834.
- Panchal V, Jeevanandan G, Subramanian E. Comparison of instrumentation time and obturation quality between hand K-file, H-files, and rotary Kedo- S in root canal treatment of primary teeth: A randomized controlled trial. J Indian SocPedodPrev Dent. 2019 Jan-Mar;37(1):75-79.Pubmed PMID: 30804311.
- Nair M, Jeevanandan G, Vignesh R, Subramanian EM. Comparative evaluation of post-operative pain after pulpectomy with k-files, kedo-s files and mtwo files in deciduous molars-a randomized clinical trial. Braz. Dent. Sci. 2018 Oct 24;21(4):411-7.
- Somasundaram S, Ravi K, Rajapandian K, Gurunathan D. Fluoride Content of Bottled Drinking Water in Chennai, Tamilnadu. J ClinDiagn Res. 2015 Oct;9(10):ZC32-4. doi: 10.7860/JCDR/2015/14691.6594. Epub 2015 Oct 1. PMID: 26557612.
- Subramanyam D, Gurunathan D, Gaayathri R, Vishnu Priya V. Comparative evaluation of salivary malondialdehyde levels as a marker of lipid peroxidation in early childhood caries. Eur J Dent. 2018 Jan-Mar;12(1):67-70. Pubmed PMID: 29657527.
- Jeevanandan G. Kedo-S Paediatric Rotary Files for Root Canal Preparation in Primary Teeth - Case Report. J ClinDiagn Res. 2017 Mar;11(3):ZR03- ZR05.Pubmed PMID: 28511532.
- Packiri S, Gurunathan D, Selvarasu K. Management of paediatric oral ranula: a systematic review. J ClinDiagn Res. 2017 Sep;11(9):ZE06-9.
- Ramakrishnan M, Bhurki M. Fluoride, Fluoridated Toothpaste Efficacy And Its Safety In Children-Review. Int. J. Pharm. Sci. Res. 2018 Oct 1;10(04):109-4.
- Ballard JL, Auer CE, Khoury JC. Ankyloglossia: assessment, incidence, and effect of frenuloplasty on the breastfeeding dyad. Pediatrics. 2002 Nov;110(5):e63.Pubmed PMID: 12415069.
- Kupietzky A, Botzer E. Ankyloglossia in the infant and young child: clinical suggestions for diagnosis and management. Pediatr Dent. 2005 Jan- Feb;27(1):40-6.Pubmed PMID: 15839394.
- Baxter R, Hughes L. Speech and feeding improvements in children after posterior tongue-tie release: a case series. Int. J. Clin. Pediatr. 2018 Jun 20;7(3):29-35.
- Suter VG, Bornstein MM. Ankyloglossia: facts and myths in diagnosis and treatment. J Periodontol. 2009 Aug;80(8):1204-19.Pubmed PMID: 19656020.
- Messner AH, Lalakea ML, Aby J, Macmahon J, Bair E. Ankyloglossia: incidence and associated feeding difficulties. Arch Otolaryngol Head Neck Surg. 2000 Jan;126(1):36-9.Pubmed PMID: 10628708.
- Jin RR, Sutcliffe A, Vento M, Miles C, Travadi J, Kishore K, et al. What does the world think of ankyloglossia? ActaPaediatr. 2018 Oct;107(10):1733- 1738.Pubmed PMID: 29385272.
- Dollberg S, Manor Y, Makai E, Botzer E. Evaluation of speech intelligibility in children with tongue-tie. ActaPaediatr. 2011 Sep;100(9):e125-7.Pubmed PMID: 21401716.
- Messner AH, Lalakea ML. The effect of ankyloglossia on speech in children. Otolaryngol. Head Neck Surg. 2002 Dec 1;127(6):539-45.
- Walls A, Pierce M, Wang H, Steehler A, Steehler M, Harley Jr EH. Parental perception of speech and tongue mobility in three-year olds after neonatal frenotomy. Int. J. Pediatr. Otorhinolaryngol. 2014 Jan 1;78(1):128-31.
- Lalakea ML, Messner AH. Ankyloglossia: the adolescent and adult perspective. Otolaryngol Head Neck Surg. 2003 May;128(5):746-52.Pubmed PMID: 12748571.
- Qazi S, Gangadhar S. Ankyloglossia-does it matter to us?. J Indian Prosthodont Soc. 2005 Jul 1;5(3):136.
- Bhattad MS, Baliga MS, Kriplani R. Clinical guidelines and management of ankyloglossia with 1-year followup: report of 3 cases. Case Rep Dent. 2013;2013:185803.Pubmed PMID: 23424685.





