Prevalence Of Hypodontia among Orthodontic Patients - A Retrospective Study
Nilesh Suresh1, Naveen Kumar M2*
1 Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
2 Senior Lecturer, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
*Corresponding Author
Naveen Kumar M,
Senior Lecturer, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
Tel: +91 9791217568
E-mail: drnaveen2012@gmail.com
Received: September 06, 2020; Accepted: October 09, 2020; Published: October 24, 2020
Citation:Nilesh Suresh, Naveen Kumar M. Prevalence Of Hypodontia among Orthodontic Patients - A Retrospective Study. Int J Dentistry Oral Sci. 2020;7(10):913-917. doi: dx.doi.org/10.19070/2377-8075-20000181
Copyright: Naveen Kumar M© 2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Hypodontia is an anomaly that could affect and influence the orthodontic diagnosis and treatment planning. The purpose of this
retrospective study was to assess the prevalence and distribution of hypodontia in the permanent dentition, excluding the third
molars, in a sample of South Indian orthodontic patients. Orthopantomograms of 500 South Indian orthodontic patients (209
boys and 291 girls) between the ages of 10 and 18 years were examined for evidence of hypodontia. The casts were used as an
additional means of confirming the diagnosis. The prevalence of hypodontia was 7.4% (3.4% for boys, 4 % for girls) with no statistically
significant difference between the sexes. The average number of missing teeth per child was 1.6 (1.4 for boys, 1.8 for girls).
The most commonly missing teeth were the maxillary lateral incisors, followed by the mandibular second premolars mandibular
and lateral incisors, and the maxillary second premolars; minor differences in the order of prevalence existed among groups of
children classified by the number of missing teeth. The distinct characteristic of hypodontia in the South Indian population compared
with other populations was a higher prevalence of both advanced hypodontia and mandibular lateral incisor agenesis in
children with minor hypodontia.
2.Introduction
3.Materials and Method
4.Results and Discussion
5.Conclusion
6.References
Keywords
Bolton; Hypodontia; Microdontia.
Introduction
Tooth agenesis, which is defined as the congenital absence of one
or more primary or permanent teeth, is one of the most frequent
human dental anomalies. Tooth agenesis can be classified as hypodontia,
oligodontia, or anodontia. The term hypodontia is used
to describe agenesis of one to six teeth.
Hypodontia, or the congenital absence of at least one permanent
tooth or tooth germ, is a common dental anomaly [1-9]. Hypodontia
is a challenge for orthodontists and pedodontists. The
number of missing teeth and the location in the dentition represent
different diagnostic problems and treatment decisions. The
most suitable age for correct diagnosis of hypodon- tia is of great
clinical importance.
There is considerable literature about the prevalence and distribution
of hypodontia, excluding third molars [10-13]. The reported
prevalence of hypodontia, excluding the third [14-16] molars, in
both sexes combined varies from 0.3% in the Israeli population
[17, 18] to 10.1% in the Norwegian population [17, 19]. The wide
range of prevalence rates of hypodontia can be attributed to differences
in the methods of sampling and examination, and the
distribution of age, sex, and racial origin of the subjects. [17-22].
Although there are a few exceptions [34, 23], most studies report
that girls have a higher prevalence of hypodontia than boys. Most
previous studies show that the most frequent missing teeth are
either the mandibular second premolars or the maxillary lateral
incisors, although Niswander and Sujaku [24] and Davis [20, 24]
reported that the mandibular incisor was the most frequently absent
tooth in Japanese and Chinese populations, respectively. The
aim of this study was to assess the prevalence of Hypodontia
among orthodontic patients.
Materials and Methodology
The subjects were selected from the case files of South Indian
orthodontic patients, between the ages of 10 and 18 years, who had visited the orthodontic Department in Saveetha Dental College
and Hospital (Chennai,India). The orthodontic files, which
included orthopantomogram, full-mouth sets (10 films) of periapical
radiographs, study models were the only sources of information
used to diagnose hypodontia. If an accurate diagnosis of
hypodontia could not be made, the files were excluded from the
study. Patients with developmental anomalies such as ectodermal
dysplasia, cleft lip or palate, or Down’s syndrome, or who had
undergone orthodontic treatment previously were also excluded
from the study.
A total of 500 case records of children (209 boys, 291 girls) were
selected randomly from the database of patients who reported to
saveetha dental college seeking ortho trt . The diagnosis of hypodontia
from orthopantomogram has been verified to be reliable
in previous studies [25, 26, 22]. Longitudinal ortho pantomogram
of most children receiving orthodontic treatment after routine
orthodontic examinations were available. A tooth was diagnosed
as congenitally missing when no mineralization of its crown could
be identified on orthopantomogram or a full-mouth set of periapical
radiographs, and no evidence of its having been extracted
was found. Third molars were not included in this study.
Ten percent of orthopantomogram of children with and without
hypodontia were reexamined by another investigator 1 month after
the initial survey, and a complete reproducibility was obtained
in the identification of hypodontia.
The chi-square or the Welch t test was performed to determine
the significance of differences in prevalence. The level of significance
was set at 5%.
Results and Discussion
A total of 500 children were selected for the study of which
58.2% were girls and 41.8% were boys [Figure.1]. Among these, a
total 37 children (7.4%) [Figure 2] were found to have hypodontia
in the permanent dentition, excluding the third molars. In total,
4% girls and 3.4% boys presented with hypodontia while 54.2%
girls and 38.4% boys didn’t present with hypodontia [Figure.3].
It was observed that 55.1% of the teeth were missing in the maxilla
nad 44.9% were missing in the mandible [Figure.4]. Chi-square
test was performed to associate between the gender and missing
teeth in subjects with hypodontia. This was found to be statistically
significant with females having more number of missing
teeth in the mandibular arch (37.18%) with Pearson’s chi-square
value of 4.807 and p value of 0.028 (p<0.05) [Figure 5].
A total of 78 permanent teeth, excluding the third molars, were
missing, with an average of 1.6 teeth per child. The boys had 33
missing teeth, with an average of 1.4 teeth per child; the girls
had 45 missing teeth, with an average of 1.8 teeth. The difference
in the number of missing teeth per child between the sexes
was not statistically significant. It was also observed that the most
commonly missing teeth in hypodontia are maxillary lateral incisors
(28.2%) followed by mandibular second premolars (24.35%)
[Figure.6].
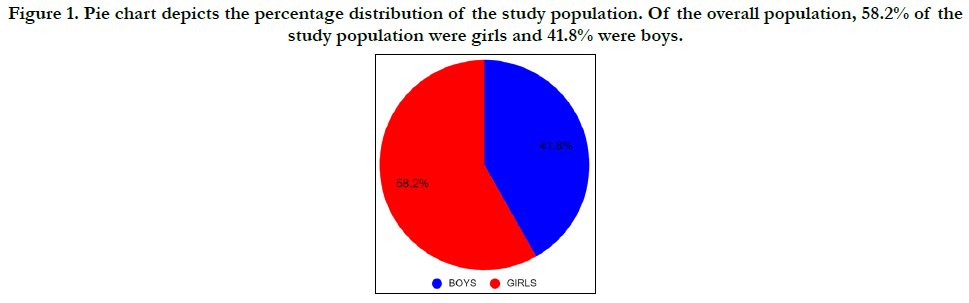
Figure 1. Pie chart depicts the percentage distribution of the study population. Of the overall population, 58.2% of the study population were girls and 41.8% were boys.
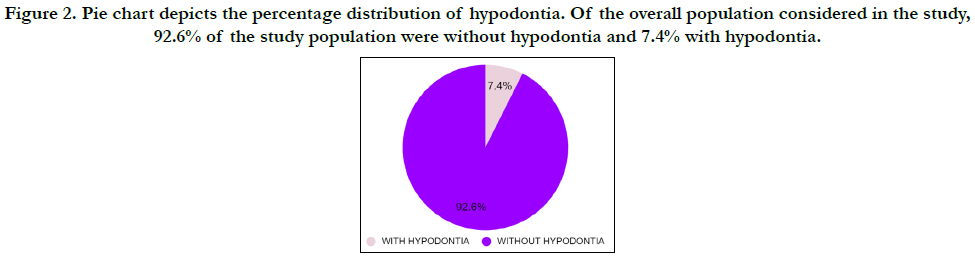

Figure 2. Pie chart depicts the percentage distribution of hypodontia. Of the overall population considered in the study, 92.6% of the study population were without hypodontia and 7.4% with hypodontia.
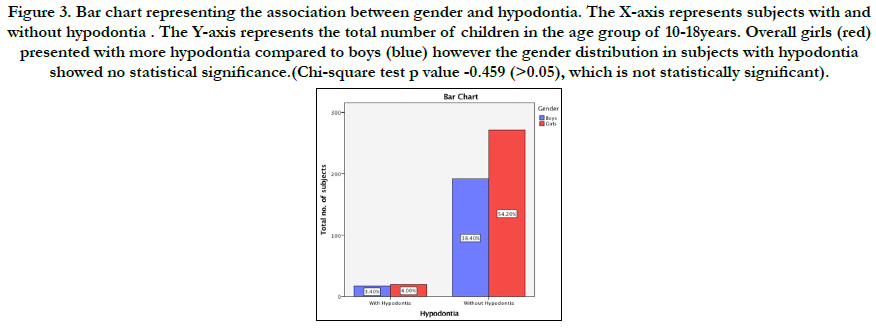
Figure 3. Bar chart representing the association between gender and hypodontia. The X-axis represents subjects with and without hypodontia . The Y-axis represents the total number of children in the age group of 10-18years. Overall girls (red) presented with more hypodontia compared to boys (blue) however the gender distribution in subjects with hypodontia showed no statistical significance.(Chi-square test p value -0.459 (>0.05), which is not statistically significant).
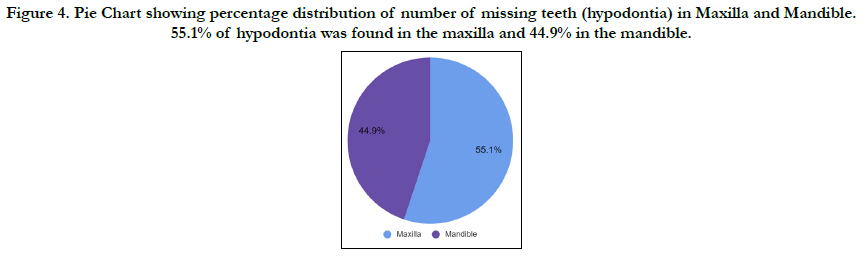
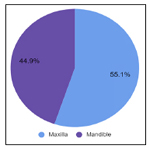
Figure 4. Pie Chart showing percentage distribution of number of missing teeth (hypodontia) in Maxilla and Mandible. 55.1% of hypodontia was found in the maxilla and 44.9% in the mandible.
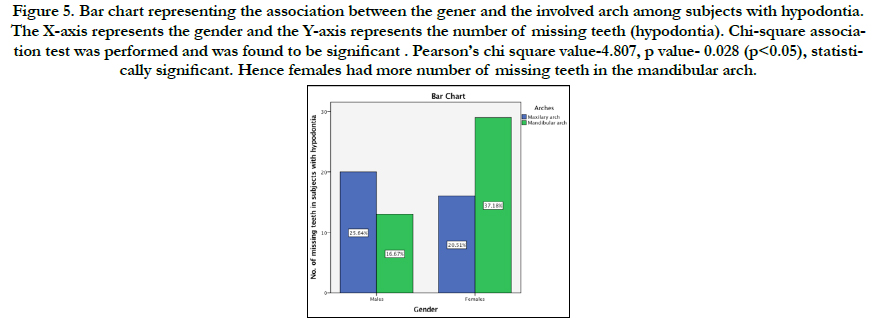
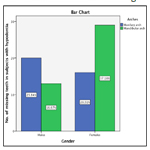
Figure 5. Bar chart representing the association between the gener and the involved arch among subjects with hypodontia. The X-axis represents the gender and the Y-axis represents the number of missing teeth (hypodontia). Chi-square association test was performed and was found to be significant . Pearson’s chi square value-4.807, p value- 0.028 (p<0.05), statistically significant. Hence females had more number of missing teeth in the mandibular arch.
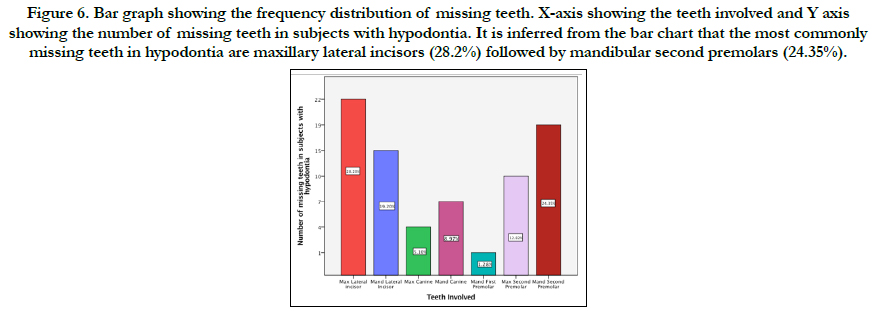
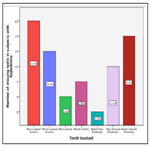
Figure 6. Bar graph showing the frequency distribution of missing teeth. X-axis showing the teeth involved and Y axis showing the number of missing teeth in subjects with hypodontia. It is inferred from the bar chart that the most commonly missing teeth in hypodontia are maxillary lateral incisors (28.2%) followed by mandibular second premolars (24.35%).
Our results varied with respect to the 3 most commonly missing teeth in each group classified by the number of missing teeth. (figure 5). Nonetheless, the maxillary lateral incisors were the most commonly missing teeth. Although minor differences existed among each sex and both sexes in the order of prevalence, the mandibular second premolars and mandibular lateral incisors followed the maxillary lateral incisors in children with 1 or 2 teeth absent.
The prevalence of missing teeth was higher in the maxilla than in the mandible in children with 1 or 2 teeth absent, and in all children with hypodontia. There were no statistically significant associations between sex and number of missing teeth in the maxilla and mandible, on the right and left sides.
The prevalence of hypodontia (excluding the third molars) was 3.4% for boys, 4% for girls, and 3.7% for both sexes combined. These figures are within the ranges of 0.2% to 8.6%, 0.4% [17] to 11.8%, [17, 19] and 0.3% to 10.1%, respectively, in the studies published previously. These percentages are much higher than those found in other studies except those by Volk, Haavikko [27], Hunstadbraten, Maklin et al, and Rolling [27, 28]. The number of missing teeth per child in both sexes combined-2.1 -is within the previously reported range of 1.541 to 4.843 and is also higher than reported in other studies except in those by Werther and Rothenberg [27-29], Brekhus et al, [10], Glenn, Horowitz [16], and Lai and Seow [23]. These higher prevalence rates of hypodontia and the larger numbers of missing teeth per child support the findings by Horowitz, Ringqvist and Thilander,and Silverman and Ackerman, who stated that teeth were more likely to be missing in orthodontic patients than in the general population. These higher prevalence rates might also represent the characteristics of the Japanese population as reported by Niswander and Sujaku [23, 24], that the hypodontia prevalence rates of 5.8% for boys, 9.2% for girls, and 7.4% for both sexes combined were relatively higher in the Japanese population than in other populations.This study showed that the prevalence of hypodontia was higher in girls than in boys with no statistically significant difference between the sexes.Furthermore, some investigators found statistically significant sex differences [17][30][31]. The number of missing teeth per child in our study was slightly higher in boys than in girls, although there is no consistent finding as to which sex is predominant in this regard.
The prevalence rate of 76.3% in children with either 1 or 2 missing teeth is within the previously reported range of 75.0% to 97.4%,20 except for the extremely low rate of 49.0% demonstrated by Lai and Seow. [23, 31]. The 76.3% prevalence is lower than those reported in other studies, except the study by Hunstadbraten (75.0%).[19, 20]. On the other hand, the 9.8% prevalence of advanced hypodontia in children is within the previously reported range of 0.0% [1, 41] to 11.3%, apart from the extremely high rate of 32.0% by Lai and Seow. This rate (9.8%) in our study is higher than those reported in other studies except the study by Grahnen (11.3%). These findings might suggest that children with minor hypodontia are involved less often, but children with advanced hypodontia are involved more often in the South Indian population.
Our findings that maxillary lateral incisor agenesis has a higher prevalence rate in children with 1 or 2 missing teeth and in all children with hypodontia disagrees with those by Niswander and Sujaku,24. Eidelman et al, [18, 24], Davis, Nik-Hussein [18, 24, 26], and Backman and Wahlin [22]. In particular, Niswander and Sujaku and Davis [20-22] showed that the mandibular incisors were the most commonly missing teeth in Japanese and Chinese populations, respectively.
Some investigators believe that the maxillary lateral incisors are followed by the mandibular second premolars [29, 10, 17, 32, 33]. which is similar to our study. An interesting finding is that the maxillary first premolars, canines, and first molars, which are likely to be more stable, have a relatively higher prevalence of hypodontia in children with 5 or more teeth missing. This means that no consistent pattern of tooth agenesis is found in children with advanced hypodontia. This agrees with observations by Aasheim and Ogaard [21, 33], Ogaard and Krogstad [34], and Endo et al. [34, 35]. This study indicated that the prevalence of maxillary lateral incisor agenesis was lower in children with advanced hypodontia; this is consistent with the result of Endo et al, [35] and supports the finding of Muller et al, [36] who stated that maxillary lateral incisor agenesis decreases with increasing hypodontia severity.
Many studies have demonstrated that there is no consistent finding as to which jaw has more missing teeth [21, 36, 22]. This supports the finding that more teeth were missing from the maxilla than from the mandible in children with 1 or 2 missing teeth, but the reverse is true of children with 4 or more missing teeth. There was a remarkable similarity in the distribution of missing teeth between the right and left sides in our subjects; this agrees with the results of most previous studies.
Our findings provide good information for clinicians on where to concentrate in orthodontic examinations of patients when hypodontia is suspected. However, the association between hypodontia and craniofacial morphology in Japanese orthodontic patients has been a controversial topic. To establish a better treatment procedure for hypodontia patients with malocclusions, the clarification of this relationship will be our central theme in future studies [37-51].
Conclusions
Within the limitation of the study it can be concluded that the
prevalence of hypodontia is 7.4% in the included study population.
The association between gender and the involved arch in
patients with Hypodontia was significant. Hypodontia was more
common in females and in the mandibular arch.
Acknowledgement
I would like to record my deep sense of gratitude to my research
supervisor Dr. Naveen Kumar M, Senior lecturer, Department
of Orthodontics, Saveetha Dental College and Hospitals, Chennai
for his inspiring guidance and encouragement with my work
during all stages. There was an equal contribution from all the
authors.
References
- Castaldi CR, Bodnarchuk A, MacRae PD, Zacherl WA. Incidence of congenital anomalies in permanent teeth of a group of Canadian children aged 6-9. J Can Dent Assoc (Tor). 1966 Mar;32(3):154-9.Pubmed PMID: 5217602.
- Helm S. Malocclusion in Danish children with adolescent dentition: an epidemiologic study. Am J Orthod. 1968 May;54(5):352-66.Pubmed PMID: 5238998.
- Salem G. Prevalence of selected dental anomalies in Saudi children from Gizan region. Community Dent Oral Epidemiol. 1989 Jun;17(3):162-3. Pubmed PMID: 2786794.
- Tal H. Familial hypodontia in the permanent dentition: a case report. J Dent. 1981 Sep;9(3):260-4.Pubmed PMID: 6944335.
- Thilander B, Pena L, Infante C, Parada SS, de Mayorga C. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogota, Colombia. An epidemiological study related to different stages of dental development. Eur J Orthod. 2001 Apr;23(2):153-68.Pubmed PMID: 11398553.
- Thilander B, Myrberg N. The prevalence of malocclusion in Swedish schoolchildren. Scand J Dent Res. 1973;81(1):12-21.Pubmed PMID: 4510864.
- Brook AH. Dental anomalies of number, form and size: their prevalence in British schoolchildren. J Int Assoc Dent Child. 1974 Dec;5(2):37-53. Pubmed PMID: 4535299.
- Locht S. Panoramic radiographic examination of 704 Danish children aged 9--10 years. Community Dent Oral Epidemiol. 1980 Oct;8(7):375-80.Pubmed PMID: 6937285.
- Tofangchiha M, Azimi S, Neirizi M. Frequency and distribution of dental anomalies in Iran: A radiographic survey. Int. J. Exp. Dent. Sci. 2013 Jan 1;2(1):14-7.
- Brekhus PJ, Oliver CP, Montelius G. A study of the pattern and combinations of congenitally missing teeth in man. J Dent Res. 1944 Apr;23(2):117- 31.
- Jha P, Jha M. Management of congenitally missing second premolars in a growing child. J Conserv Dent. 2012 Apr;15(2):187-90.Pubmed PMID: 22557822.
- Thompson GW, Popovich F. Probability of congenitally missing teeth: results in 1,191 children in the Burlington Growth centre in Toronto. Community Dent Oral Epidemiol. 1974;2(1):26-32.Pubmed PMID: 4153443.
- Järvinen S, Lehtinen L. Supernumerary and congenitally missing primary teeth in Finnish children. An epidemiologic study. Acta Odontol Scand. 1981;39(2):83-6.Pubmed PMID: 6948487.
- Hobkirk JA, Gill DS, Jones SP, Hemmings KW, Bassi GS, O'Donnell AL, Goodman JR. Hypodontia: a team approach to management. John Wiley & Sons; 2010 Nov 11:208.
- Becker A. Orthodontic Treatment of Impacted Teeth,Second Edition. CRC Press; 2007. 342 p.
- Horowitz JM. Aplasia and malocclusion: a survey and appraisal. Am J Orthod. 1966 Jun;52(6):440-53.Pubmed PMID: 5219037.
- Rosenzweig KA, Garbarski D. Numerical aberrations in the permanent teeth of grade school children in Jerusalem. Am J Phys Anthropol. 1965 Sep;23(3):277-83.Pubmed PMID: 5861224.
- Eidelman E, Chosack A, Rosenzweig KA. Hypodontia: prevalence amongst Jewish populations of different origin. Am J Phys Anthropol. 1973 Jul;39(1):129-33.Pubmed PMID: 4713560.
- Acev DP, Gjorgova J. Prevalence of hypodontia in the permanent dentition of Macedonian population. Balk J Dent Med. 2014 Jul 1;18(2):93-8.
- Davis PJ. Hypodontia and hyperdontia of permanent teeth in Hong Kong schoolchildren. Community Dent Oral Epidemiol. 1987 Aug;15(4):218-20. Pubmed PMID: 3476247.
- Aasheim B, Ögaard B. Hypodontia in 9‐year‐old Norwegians related to need of orthodontic treatment. Eur J Oral Sci. 1993 Oct;101(5):257-60.
- Bäckman B, Wahlin YB. Variations in number and morphology of permanent teeth in 7-year-old Swedish children. Int J Paediatr Dent. 2001 Jan;11(1):11-7.Pubmed PMID: 11309867.
- Lai PY, Seow WK. A controlled study of the association of various dental anomalies with hypodontia of permanent teeth. Pediatr Dent. 1989 Dec;11(4):291-6.Pubmed PMID: 2639323.
- Niswander JD, Sujaku C. CONGENITAL ANOMALIES OF TEETH IN JAPANESE CHILDREN. Am J Phys Anthropol. 1963 Dec;21(4):569-74. Pubmed PMID: 14185534.
- Wisth PJ, Thunold K, Böe OE. Frequency of hypodontia in relation to tooth size and dental arch width. Acta Odontol Scand. 1974;32(3):201-6.Pubmed PMID: 4155221.
- . Nik-Hussein NN. Hypodontia in the permanent dentition: a study of its prevalence in Malaysian children. Aust Orthod J. 1989 Oct;11(2):93-5.Pubmed PMID: 2639661.
- Haavikko K. Hypodontia of permanent teeth. An orthopantomographic study. Suom Hammaslaak Toim. 1971;67(4):219–25.
- Rølling S. Hypodontia of permanent teeth in Danish schoolchildren. Scand J Dent Res. 1980 Oct;88(5):365-9.Pubmed PMID: 6936762.
- Werther R, Rothenberg F. Anodontia.Am J Orthod Oral Surg. 1939;25: 61–81.
- Thilander B. Indications for orthodontic treatment in adults. The Eur. J. Orthod. 1979 Jan 1;1(4):227-41.
- NAKAHARA M, OKADA S, TANI H, KATSURA N. A survey of congenitally missing permanent teeth in Hokkaido. J Dent Health. 1977;27(1):21- 3.
- Ruprecht A, Batniji S, el-Neweihi E. Incidence of oligodontia (hypodontia). J Oral Med. 1986 Jan;41(1):43–6.
- Silva Meza R. Radiographic assessment of congenitally missing teeth in orthodontic patients. Int. J. Paediatr. Dent. 2003 Mar;13(2):112-6.
- Ogaard B, Krogstad O. Craniofacial structure and soft tissue profile in patients with severe hypodontia. Am J Orthod Dentofacial Orthop. 1995 Nov;108(5):472-7.Pubmed PMID: 7484966.
- Endo T, Yoshino S, Ozoe R, Kojima K, Shimooka S. Association of advanced hypodontia and craniofacial morphology in Japanese orthodontic patients. Odontology. 2004 Sep;92(1):48-53.Pubmed PMID: 15490305.
- Muller TP, Hill IN, Petersen AC, Blayney JR. A survey of congenitally missing permanent teeth. J Am Dent Assoc. 1970 Jul 1;81(1):101-7.
- Sivamurthy G, Sundari S. Stress distribution patterns at mini-implant site during retraction and intrusion--a three-dimensional finite element study. Prog Orthod. 2016;17:4.Pubmed PMID: 26780464.
- Samantha C, Sundari S, Chandrasekhar S, Sivamurty G, Dinesh S. Comparative Evaluation of Two Bis-GMA Based Orthodontic Bonding Adhesives - A Randomized Clinical Trial. J Clin Diagn Res. 2017 Apr;11(4):ZC40- ZC44.Pubmed PMID: 28571259.
- Krishnan S, Pandian S, Kumar S A. Effect of bisphosphonates on orthodontic tooth movement-an update. J Clin Diagn Res. 2015 Apr;9(4):ZE01-5. Pubmed PMID: 26023659.
- . Vikram NR, Prabhakar R, Kumar SA, Karthikeyan MK, Saravanan R. Ball Headed Mini Implant. J Clin Diagn Res. 2017 Jan;11(1):ZL02-3.
- Kamisetty SK, Verma JK, Arun, Sundari S, Chandrasekhar S, Kumar A. SBS vs Inhouse Recycling Methods-An Invitro Evaluation. J Clin Diagn Res. 2015 Sep;9(9):ZC04-8.Pubmed PMID: 26501002.
- Viswanath A, Ramamurthy J, Dinesh SP, Srinivas A. Obstructive sleep apnea: awakening the hidden truth. Niger J Clin Pract. 2015 Jan-Feb;18(1):1-7. Pubmed PMID: 25511335.
- Felicita AS. Quantification of intrusive/retraction force and moment generated during en-masse retraction of maxillary anterior teeth using mini-implants: A conceptual approach. Dental Press J Orthod. 2017 Sep- Oct;22(5):47-55.Pubmed PMID: 29160344.
- Rubika J, Felicita AS, Sivambiga V. Gonial angle as an indicator for the prediction of growth pattern. World J Dent. 2015;6(3):161-3.
- Jain RK, Kumar SP, Manjula WS. Comparison of intrusion effects on maxillary incisors among mini implant anchorage, j-hook headgear and utility arch. J Clin Diagn Res. 2014 Jul;8(7):ZC21-4.Pubmed PMID: 25177631.
- Pandian KS, Krishnan S, Kumar SA. Angular photogrammetric analysis of the soft-tissue facial profile of Indian adults. Indian J Dent Res. 2018 Mar- Apr;29(2):137-143.Pubmed PMID: 29652003.
- Ramesh Kumar KR, Shanta Sundari KK, Venkatesan A, Chandrasekar S. Depth of resin penetration into enamel with 3 types of enamel conditioning methods: a confocal microscopic study. Am J Orthod Dentofacial Orthop. 2011 Oct;140(4):479-85.Pubmed PMID: 21967934.
- Felicita AS. Orthodontic management of a dilacerated central incisor and partially impacted canine with unilateral extraction - A case report. Saudi Dent J. 2017 Oct;29(4):185-193.Pubmed PMID: 29033530.
- Felicita AS, Chandrasekar S, Shanthasundari KK. Determination of craniofacial relation among the subethnic Indian population: a modified approach - (Sagittal relation). Indian J Dent Res. 2012 May-Jun;23(3):305-12. Pubmed PMID: 23059564.
- Dinesh SP, Arun AV, Sundari KK, Samantha C, Ambika K. An indigenously designed apparatus for measuring orthodontic force. J Clin Diagn Res. 2013 Nov;7(11):2623-6.Pubmed PMID: 24392423.
- Felicita AS. Orthodontic extrusion of Ellis Class VIII fracture of maxillary lateral incisor - The sling shot method. Saudi Dent J. 2018 Jul;30(3):265- 269.Pubmed PMID: 29942113.





