Prevalence of Broken Denture in Completely Edentulous Patients - A Retrospective Study
Prashaanthi. N1, Jessy. P2*, Subhabrata Maiti3, Shantha sundari. K.K4
1 Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
2 Senior Lecturer, Department of Pedodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
3 Senior Lecturer, Department of Prosthodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
4 Professor, Department of Orthodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077, India.
*Corresponding Author
Jessy. P,
Senior Lecturer, Department of Pedodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, 600077,
India.
Tel: 8861646189
E-mail: jessyp.sdc@saveetha.com
Received: September 06, 2020; Accepted: October 09, 2020; Published: October 24, 2020
Citation:Prashaanthi. N, Jessy. P, Subhabrata Maiti, Shantha sundari. K.K. Prevalence of Broken Denture in Completely Edentulous Patients - A Retrospective Study. Int J Dentistry Oral Sci. 2020;7(10):898-902. doi: dx.doi.org/10.19070/2377-8075-20000178
Copyright: Jessy. P© 2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Replacement of missing teeth and the associated structures are done with the help of artificial prosthesis. One of the most common
complications of the denture is the fracture. There are numerous factors contributing to the fracture of denture. The aim
of the study was to evaluate the prevalence of broken complete denture among completely edentulous patients.This retrospective
study included patients who reported with complete edentulism from July 2019 to March 2020 in a dental hospital. The case
records of all patients were retrieved and details were recorded. Variables such as age, gender, status of the denture whether fractured
or not were also extracted from the case records. Data was tabulated and statistically analysed using IBM SPSS version 20.0
and results were obtained. Descriptive and chi square analysis was done to get the association among age, gender and the broken
denture. P value <0.05 was considered as statistically significant.In the present study, out of 355 completely edentulous patients ,
8.2% reported with broken denture. On comparing the different age groups, there was higher prevalence among 51-60 years age
groups(5.07%). On analysing the prevalence of broken dentures among gender, 5.92% of males and 2.25% of females reported
with broken dentures, with a higher prevalence among males. There was statistically significant association between age and broken
denture (p<0.05) and no statistically significant association was found between gender and the broken denture (p>0.05). Within
the limitations of the present study, there was higher prevalence of broken denture among males which could be due to high
masticatory forces. And the broken dentures were more commonly reported among old aged population which could be due to
long term usage of the denture.
2.Introduction
3.Materials and Method
4.Results and Discussion
5.Conclusion
6.Acknowledgement
7.References
Keywords
Denture Fracture; Mastication; Occlusal Prematurity; Porosity.
Introduction
The ideal treatment for completely edentulous patients is rehabilitation
by conventional complete denture. The esthetics, mastication,
speech are affected in a completely edentulous patient
wherein there is a need for the construction of the complete denture.
The factors causing problems in the complete denture fabrication
and adaptation by the patients may be classified as adverse
intraoral anatomical factors, clinical factors such as poor denture
stability, technical factors such as failure to preserve the peripheral
seal on a master cast and patient adaptional factors [1].
After the complete denture delivery, acceptance and wearing complete
dentures is one of utmost important factors for the success
of complete denture [2]. The patient’s face various problems or
interferences in wearing the denture. One of the interferences in
wearing dentures is the fracture of the denture. Previous studies
have reported that the most common complication of the denture
is the denture fracture which leads to the discontinuity of
denture wearing among patients [2].
Denture fractures cause functional insufficiency, compromised
esthetic and financial burden on its users for its repair or refabrication
[3-5].
One of the reasons for the fracture of the denture could be the
masticatory efficiency , bite and chewing efficiency of the patients
which has an important role in the functional adaptation of prosthetic
rehabilitation [6]. The relative measures for the preparation
and adaptation to the swallowing capacity of the individual
should be taken into consideration during the construction and
fabrication of the denture [7-9].
Other factors that exacerbates the deformation of the base or
alters its stress distribution are the polymethyl methacrylate dentures
which are prone for fractures [10]. The challenges faced during
the construction of the denture is the displacement of the
denture during chewing and speaking [11]. Adequate follow up of
the patients is one of the difficulties faced after the denture insertion.
The selection of appropriate dental material and technique
has an important role in the maintenance and success of the complete
denture. Proper oral hygiene maintenance by the patient also
has an essential role in the denture wearing patients [4].
Hence there should be adequate longer follow up in order to
check whether the patient continued to wear denture or not and
also to assess the status of the denture. If there is a fracture ,
the identification of the fracture on which part of the denture,
whether on the denture base or on the artificial teeth has to be
noted and further repair or rebasing should be carried out to
replace the fractured denture among patients [1, 4]. Previously
our institutional team has done various awareness studies [12-14],
clinical studies [15-22] ,systematic reviews [21, 23-26]. Now we
are focussing on epidemiological studies. The thought for this
study stemmed from the present interest in our community.Hence
the aim of this study was to assess the prevalence of completely
edentulous patients reporting with broken denture.
This retrospective study was conducted to evaluate the patients
reporting with broken dentures who visited Saveetha dental college
and hospital from July 2019 to March 2020. The study was
initiated after approval from the Institutional ethical committee.
Ethical approval number was SDC/SIHEC/2020/DIASDATA/
0619-0320.
After thorough assessment of 86000 case records in the university
patient data records, case records of all completely edentulous
patients were included in the study. The exclusion criteria was
missing or incomplete data. Cross verification of data for errors
was done with the help of an external examiner.
The case records of the completely edentuous patients from July
2019 to March 2020 were examined by a single calibrated examiner.
Relevant factors such as status of the denture whether broken
or not broken were retrieved. Demographic details such as age ,
gender were also recorded.
The collected data was tabulated and analysed with a statistical
package for windows, IBM SPSS version 20.0 and results were
obtained. Categorical variables were expressed in frequency and
percentage. Chi Square tests were employed to analyse the association
of categorical variables with a level of significance set at
p<0.05.
Results and Discussion
In our study, out of 355 completely edentulous patients, 8.2%
of the patients reported with broken denture. On comparing the
distribution percentage of broken dentures among different age
groups it was found that 5.07% were under 51-60 years, 2.25%
were under 61-70 years, 0.56% under 41-50 years, 0.28% were
under 31-40 years age groups. On analysing the association of
broken dentures, the higher prevalence was found among 51-60
years (5.07%) followed by the 61- 70 years age group (2.3%). [Figure
1] There was a statistically significant association between the
status of the dentures among different age groups. (p value-0.001)
[Table 1, Figure 2]
In our study out of 355 completely edentulous patients , 57.92%
were males and 41.97% were females. On analysing the association
between the status of the dentures among gender, there was
a higher prevalence among males (5.92%) than females(2.25%).
[Figure 3] No statistically significant association was found between
the status of the denture and gender.(p value -0.101). [Table
1, Figure 4]. The result of the study shows that the most affected age group is 51-60 years. The prevalence of broken denture is
more common in males and less in females. There is a positive
correlation in between the broken denture and the different age
groups.
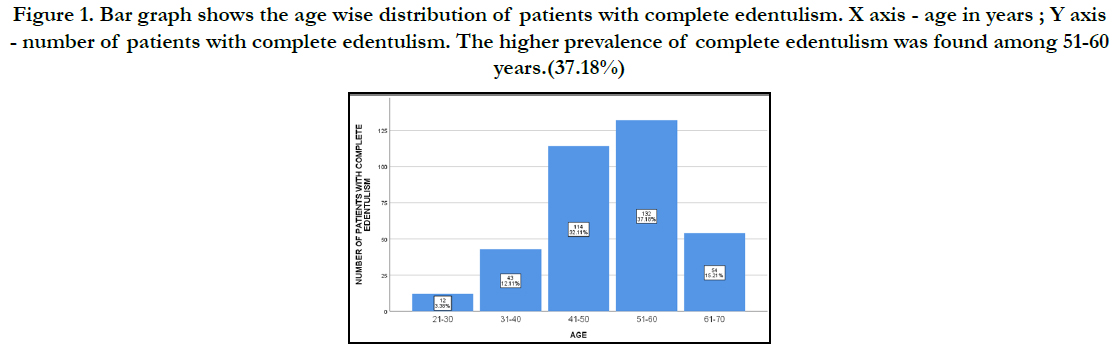
Figure 1. Bar graph shows the age wise distribution of patients with complete edentulism. X axis - age in years ; Y axis - number of patients with complete edentulism. The higher prevalence of complete edentulism was found among 51-60 years.(37.18%)
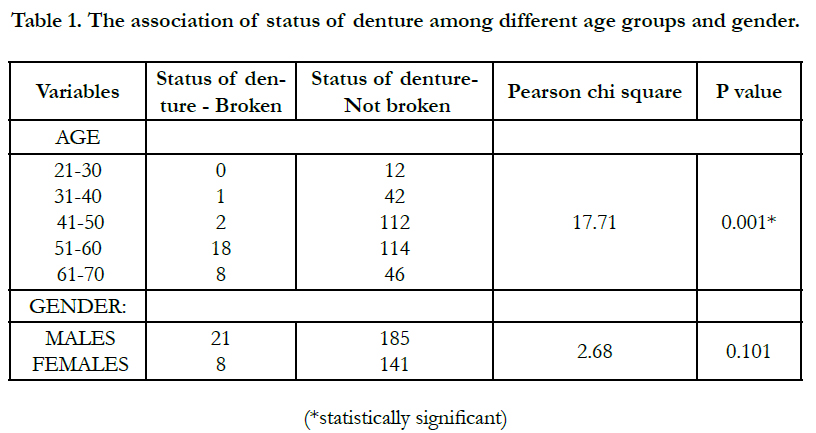

Table 1. The association of status of denture among different age groups and gender.
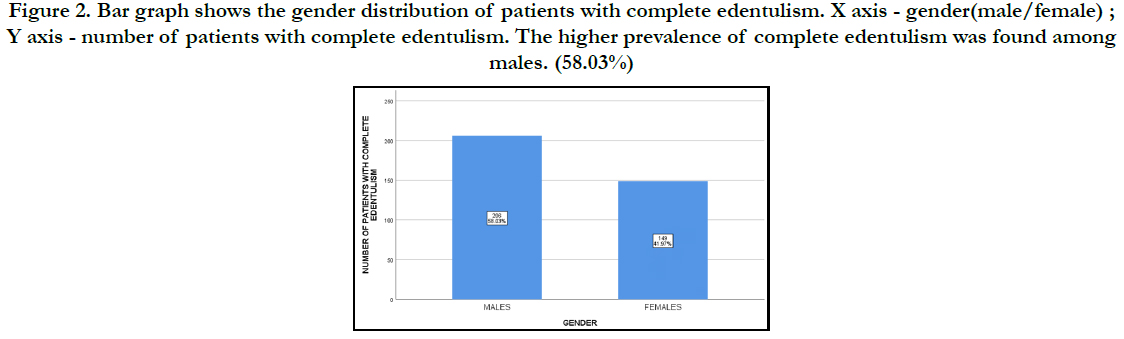
Figure 2. Bar graph shows the gender distribution of patients with complete edentulism. X axis - gender(male/female) ; Y axis - number of patients with complete edentulism. The higher prevalence of complete edentulism was found among males. (58.03%)
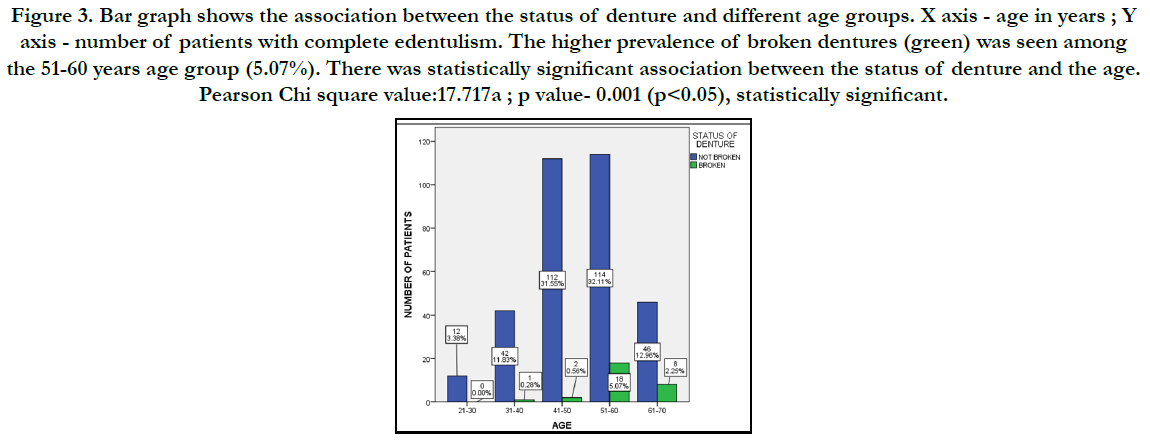
Figure 3. Bar graph shows the association between the status of denture and different age groups. X axis - age in years ; Y axis - number of patients with complete edentulism. The higher prevalence of broken dentures (green) was seen among the 51-60 years age group (5.07%). There was statistically significant association between the status of denture and the age. Pearson Chi square value:17.717a ; p value- 0.001 (p<0.05), statistically significant.
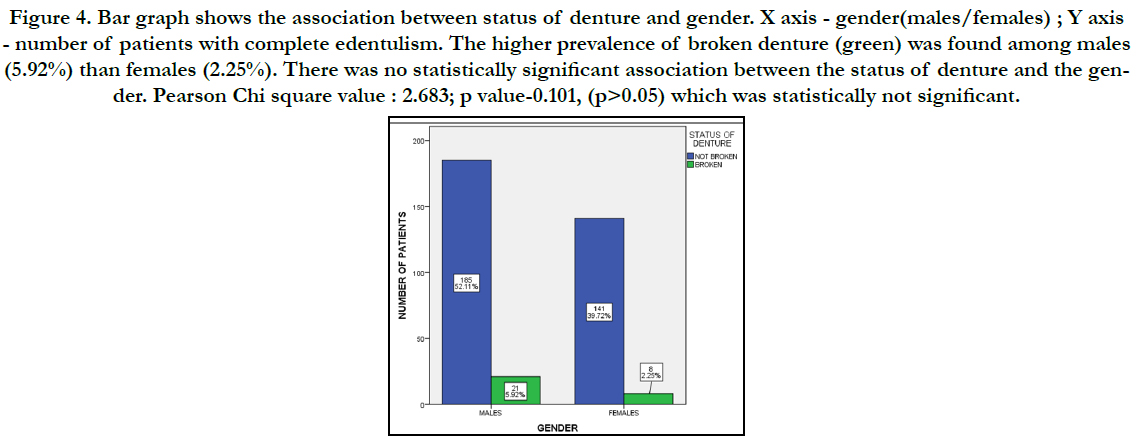
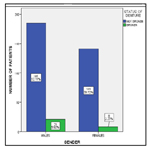
Figure 4. Bar graph shows the association between status of denture and gender. X axis - gender(males/females) ; Y axis - number of patients with complete edentulism. The higher prevalence of broken denture (green) was found among males (5.92%) than females (2.25%). There was no statistically significant association between the status of denture and the gender. Pearson Chi square value : 2.683; p value-0.101, (p>0.05) which was statistically not significant.
In the present study, there was a higher prevalence of broken denture among males. Previous studies have said that the more prevalence of broken dentures among males could be due to increased masticatory force and fatigue of the denture, this is in acceptance to our study, where there is a male predominance (6.40%) [5, 27, 28]. There is association of biting force and the fracture of the denture. Among the young old aged patients, they are recent denture wearers, where there is increased biting force which leads to fracture of the denture. Study done by Sampa Ray 1 et.al, he said there is denture fracture due to increased biting force [27]. Studies done by Beley,et.al Hargreaves A.S, et.al, has said that the cause of the denture can either be mechanical or accidental [10, 29].
In the present study , the prevalence of broken dentures were higher among 51 to 60 years age groups followed by 61 to 70 year age groups. The prevalence among old aged people could be due to longer denture usage and also could be due to improper handling and hygiene maintenance among the patients. Previous studies have reported that the prevalence of broken dentures were more prevalent above 80years age followed by 40 to 50 years age groups [30]. The reason for the variation in prevalence of broken dentures could be due to the geographic location, denture maintenance and the duration of denture wearing by the patient.
Denture fractures can be prevented by patient education on denture maintenance and oral hygiene maintenance and motivation to change the denture incase of any fracture or breakage.The case selection and the appropriate treatment planning are important for the delivery of the denture to the edentulous patients.
Recent advances such as use of a BPS denture base and CAD CAM milling dentures are commonly preferred in the clinical practice for the construction of complete denture [31-33]. The lucitone , metal base and modified acrylic denture bases can be used as an alternative due to their increased mechanical property [34]. The effect of practicing BPS dentures (modification of processing), by injection molding technique records the area more accurately which aids in the retention and stability of the denture. The use of T scan for bite force evaluation and occlusal equilibrium can be used to assess the masticatory efficiency of the individual and construct the denture accordingly [35]. All the above factors along with definite dental prosthetic principles should be taken into consideration for denture construction.
The limitation of the present study was that it was a retrospective study where we used data from the online digital case records. The prevalence of broken denture was evaluated from the patient's history which were recorded in the case records of the patients. To reduce the subjective variation , the case records were analysed by a single calibrated examiner. Records did not contain the history on the type, duration and cause of the fracture of the denture which could have been a profound factor in our study.
Conclusion
Within the limitation of the present study there was a male predominance
of broken denture which can be due to high masticatory
load. Secondly, completely edentulous old aged patients
reported with breakage indicating long term use. On the other
hand, for young aged completely edentulous patients, denture
breakage chances were seen due to high masticatory forces following
recent extractions. Hence forth change of new denture is
recommended for the patients after a period of time and development
towards denture material and technique is a need.
Authors Contribution
Prashaanthi. N contributed acquisition of data, analysis, literature
collection and also in drafting the article and revising it critically
for important intellectual content. Jessy .P and Subhabrata Maiti contributed in conception, the study design, interpretation of
data, formatting, manuscript preparation, supervision and guidance.
Shantha sundari. K.K contributed in editing, supervision
and final approval of the submitted version of the manuscript.
Acknowledgement
We take pleasure to acknowledge our University for granting permission
to utilize the patient records for data collection.
References
- McCord JF, Grant AA. Identification of complete denture problems: a summary. Br Dent J. 2000 Aug 12;189(3):128-34.Pubmed PMID: 11041628.
- Takamiya AS, Monteiro DR, Marra J, Compagnoni MA, Barbosa DB. Complete denture wearing and fractures among edentulous patients treated in university clinics. Gerodontology. 2012 Jun;29(2):e728-34.Pubmed PMID: 21883425.
- Vallittu PK, Lassila VP, Lappalainen R. Evaluation of damage to removable dentures in two cities in Finland. Acta Odontol Scand. 1993 Dec;51(6):363- 9.Pubmed PMID: 8304013.
- Darbar UR, Huggett R, Harrison A. Denture fracture--a survey. Br Dent J. 1994 May;176(9):342-5.
- Smith DC. The acrylic denture mechanical evaluation mid-line fracture. Br. Dent. J.. 1961;110:257-67.
- Moraru AM, Preoteasa CT, Preoteasa E. Masticatory function parameters in patients with removable dental prosthesis. J Med Life. 2019 Jan;12(1):43-8.
- Liedberg B, Ekberg O, Owall B. Chewing and the dimension of the pharyngoesophageal segment. Dysphagia. 1991;6(4):214-8.Pubmed PMID: 1778099.
- Woda A, Hennequin M, Peyron MA. Mastication in humans: finding a rationale. J Oral Rehabil. 2011 Oct;38(10):781-4.Pubmed PMID: 22093138.
- Fontijn-Tekamp FA, Slagter AP, Van Der Bilt A, Van 'T Hof MA, Witter DJ, Kalk W, et al. Biting and chewing in overdentures, full dentures, and natural dentitions. J Dent Res. 2000 Jul;79(7):1519-24.Pubmed PMID: 11005738.
- Beyli MS, von Fraunhofer JA. An analysis of causes of fracture of acrylic resin dentures. J Prosthet Dent. 1981 Sep;46(3):238-41.Pubmed PMID: 7021802.
- Shala K, Tmava-Dragusha A, Dula L, Pustina-Krasniqi T, Bicaj T, Ahmedi E, et al. Evaluation of Maximum Bite Force in Patients with Complete Dentures. Open Access Maced J Med Sci. 2018 Mar 13;6(3):559-563.Pubmed PMID: 29610620.
- Ashok V, Suvitha S. Awareness of all ceramic restoration in rural population. Res J Pharm Technol. 2016;9(10):1691-3.
- Vijayalakshmi B, Ganapathy D. Medical management of cellulitis. Res J Pharm Technol. 2016;9(11):2067-70.
- Basha FYS, Ganapathy D. Oral Hygiene Status among Pregnant Women. Res J Pharm Technol. 2018.
- Jyothi S, Robin PK, Ganapathy D. Periodontal health status of three different groups wearing temporary partial denture. Res J Pharm Technol. 2017;10(12):4339-42.
- Duraisamy R, Krishnan CS, Ramasubramanian H, Sampathkumar J, Mariappan S, Navarasampatti Sivaprakasam A. Compatibility of Nonoriginal Abutments With Implants: Evaluation of Microgap at the Implant-Abutment Interface, With Original and Nonoriginal Abutments. Implant Dent. 2019 Jun;28(3):289-295.Pubmed PMID: 31124826.
- Ganapathy D, Sathyamoorthy A, Ranganathan H, Murthykumar K. Effect of Resin Bonded Luting Agents Influencing Marginal Discrepancy in All Ceramic Complete Veneer Crowns. J Clin Diagn Res. 2016 Dec;10(12):ZC67- ZC70.Pubmed PMID: 28209008.
- Ranganathan H, Ganapathy DM, Jain AR. Cervical and Incisal Marginal Discrepancy in Ceramic Laminate Veneering Materials: A SEM Analysis. Contemp Clin Dent. 2017 Apr-Jun;8(2):272-278.Pubmed PMID: 28839415.
- Venugopalan S, Ariga P, Aggarwal P, Viswanath A. Magnetically retained silicone facial prosthesis. Niger J Clin Pract. 2014 Mar-Apr;17(2):260-4. Pubmed PMID: 24553044.
- Ajay R, Suma K, Ali SA, Kumar Sivakumar JS, Rakshagan V, Devaki V, et al. Effect of Surface Modifications on the Retention of Cement-retained Implant Crowns under Fatigue Loads: An In vitro Study. J Pharm Bioallied Sci. 2017 Nov;9(Suppl 1):S154-S160.Pubmed PMID: 29284956.
- Jain AR, Nallaswamy D, Ariga P, Ganapathy DM. Determination of correlation of width of maxillary anterior teeth using extraoral and intraoral factors in Indian population: A systematic review. World J Dent. 2018 Jan;9:68-75.
- Ashok V, Nallaswamy D, Benazir Begum S, Nesappan T. Lip Bumper Prosthesis for an Acromegaly Patient: A Clinical Report. J Indian Prosthodont Soc. 2014 Dec;14(Suppl 1):279-82.Pubmed PMID: 26199531.
- Selvan SR, Ganapathy D. Efficacy of fifth generation cephalosporins against methicillin-resistant Staphylococcus aureus-A review. Res J Pharm Technol. 2016;9(10):1815-8.
- Subasree S, Murthykumar K. Effect of Aloe Vera in Oral Health-A Review. Res J Pharm Technol. 2016;9(5):609-12.
- Kannan A. Effect of Coated Surfaces influencing Screw Loosening in Implants: A Systematic Review and Meta-analysis. World. 2017 Nov;8(6):496- 502.
- Kannan A, Venugopalan S. A systematic review on the effect of use of impregnated retraction cords on gingiva. Res J Pharm Technol. 2018;11(5):2121-6.
- Ray PK, Makhal M, Sen SK. Incidence and causes of fracture of acrylic resin complete denture. J. Evol. Med. Dent. Sci. 2014 Dec 11;3(69):14787-94.
- Broz M, Omrcen A, Ropac D. Characteristics of fractures in complete dentures. Vojnosanit Pregl. 1991 Jan 1;48(1):46-50.
- Hargreaves AS. The prevalence of fractured dentures. A survey. Br Dent J. 1969 May 20;126(10):451-5.
- Bosânceanu DN, Beldiman A, Baciu RE, Bolat M, Bosânceanu DG, Forna NC. Complete dentures fractures–causes and incidence. J. Oral Rehabil. 2017 Jan;9(1).
- Saini V, Singla R. Biofunctional prosthetic system: A new era complete denture. J Pharm Bioallied Sci. 2011 Jan;3(1):170-2.Pubmed PMID: 21430969.
- John AV, Abraham G, Alias A. Two-visit CAD/CAM milled dentures in the rehabilitation of edentulous arches: A case series. J Indian Prosthodont Soc. 2019 Jan-Mar;19(1):88-92.Pubmed PMID: 30745760.
- Han W, Li Y, Zhang Y. Design and fabrication of complete dentures using CAD/CAM technology. Medicine. 2017 Jan;96(1): e5435.
- Phukela SS, Chintalapudi SK, Sachdeva H, Dhall RS, Sharma N, Prabhu A. Comparative evaluation of different mechanical modifications of denture teeth on bond strength between high-impact acrylic resin and denture teeth: An in vitro study. J Int Soc Prev Community Dent. 2016 Mar- Apr;6(2):161-6.Pubmed PMID: 27114957.
- Agbaje JO, Casteele EV, Salem AS, Anumendem D, Shaheen E, Sun Y, et al. Assessment of occlusion with the T-Scan system in patients undergoing orthognathic surgery. Sci Rep. 2017 Jul 13;7(1):1-8.Pubmed PMID: 28706294.





