Oral Hygiene and Oral Health Related Quality of Life of Children with Stunting in Indonesia
Husain Akbar F1*, Pratiwi R1, Sri Naca Hardiana AN2
1 Department of Dental Public Health, Faculty of Dentistry, Hasanuddin University, Makassar, Indonesia.
2 Clinical Student, Faculty of Dentistry, Hasanuddin University, Makassar, Indonesia.
*Corresponding Author
Fuad Husain Akbar,
Department of Dental Public Health, Faculty of Dentistry, Hasanuddin University, Makassar, Indonesia.
Tel: +62-81243422362
E-mail: fuadgi2@gmail.com
Received: December 23, 2019; Accepted: January 07, 2020; Published: January 09, 2020
Citation:Husain Akbar F, Pratiwi R, Sri Naca Hardiana AN. Oral Hygiene and Oral Health Related Quality of Life of Children with Stunting in Indonesia. Int J Dentistry Oral Sci. 2020;7(1):711-717. doi: dx.doi.org/10.19070/2377-8075-20000140
Copyright: Husain Akbar F©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: The purpose of this research is to find out about the description of oral hygiene, and the quality of life-related to dental and oral health in patients with stunting in Enrekang Regency.
Materials and Methods: This study was an observational analytic cross-sectional study design conducted on 29 April-3 May 2019. This study used BMI scores for height measurements, OHI-S scores for oral cavity and assessment of children's quality of life-related to oral health. using the Child Perception Questionnaire. During data collection, 334 subjects participated in the study until the end. Subjects aged 8-10 years as many as 70 people were given a CPQ8-10 questionnaire to assess the oral health related quality of life, while for subjects aged 11-12 years as many as 20 people were given a CPQ11-14 questionnaire to assess the quality of life-related to their oral health.
Results: There were 123 children from all subjects who were stunted. The mean value of OHI-S based on age and sex of the highest stunting children at 6-7 years old (2.03 ± 0.74). Based on sex the mean value of OHI-S was higher in males (1.83 ± 0.81).
Conclusion:Based on the results of the study, it can be concluded that children who experience stunting in Enrekang District have moderate oral hygiene status and based on the dimensions of quality of life, stunting children have the most complaints on the dimensions of oral symptoms.
2.Introduction
3.Materials & Methods
3.1 Study Design
3.2 Data Analysis
3.3 Ethics Aspect
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Stunting; Oral Hygiene; Quality of Life.
Introduction
Stunting is one of the nutritional problems faced in the world, especially in poor and developing countries. Stunting is a problem because it is associated with an increased risk of morbidity and death, suboptimal brain development so that motor development is delayed and stunted mental growth [1, 2].
Stunting is measured by an indicator of height measurement for age (TB/U) according to WHO child growth standard, that is if the z-score (TB/U ≤ 2 SD). Indicators (TB/U) indicates chronic nutritional problems as a result of long-standing conditions, such as poverty, unhealthy behavior, and poor parenting or eating patterns since a child is born to cause the child to become short [3, 4].
The prevalence of stunting in children under five based on Basic Health Research data in 2007 and 2010 in Indonesia is still very high, namely 36.8% (18.8% very short and 18.0% short) in 2007 and 35.6% (18.5 % is very short and 17.1% is short) in 2010 so it can be concluded that stunting occurs in more than one third of children under five in Indonesia [5, 6].
South Sulawesi Province experienced an increase in stunting from 2007 (29.1%), increasing in 2010 (36.8%) and again experiencing an increase in 2013 to 40.9%. This indicates that the problem of stunting in infants is a public health problem considered serious because it reaches a stunting prevalence of ≥ 40%. Enrekang Regency is the regency with the highest stunting prevalence, which is 53.37% in 2013 in South Sulawesi [8].
Dental and oral health is an integral part of body health, meaning that a healthy body is inseparable from having healthy teeth and mouth. Therefore, to carry out development in the field of health, development in the field of dental health must not be abandoned. However, at this time Indonesian people's awareness of the importance of having a healthy quality of dental health is still lacking. Tooth and mouth hygiene is a condition where the teeth inside the oral cavity are clean, free from plaque, tartar, and food scraps and not smell in the mouth. Good dental hygiene can affect a person's quality of life, such as: chewing, eating, swallowing and talking. Poor oral hygiene conditions such as calculus and stain, many dental caries, and toothless or toothless conditions can cause problems in daily life [9].
Parental knowledge is also very important in underlying the formation of behaviors that support children's dental and oral hygiene. Such knowledge can be obtained naturally or in a planned manner through the education process. Parents with low knowledge about dental and oral health will have an impact on behavior that is not supportive of maintaining the oral health of children. Children have a close relationship with parents, especially their mothers. Generally, the maintenance of children's health depends on the mother. The closeness of the mother's relationship with her child has been stated by Fukuta who stated that the mother's behavior regarding dental health can be used to predict the health status of her child's teeth. If the mother's behavior regarding dental health is good, it can be predicted that her child's dental health status is also good [10].
Short toddler problems describe the existence of chronic nutritional problems, influenced by the condition of the mother/ prospective mother, the fetus, and infancy/toddler, including illnesses, suffered during infancy. Like other nutritional problems, it is not only related to health issues but is also influenced by various other conditions that indirectly affect health [11]. Related to efforts to reduce and manage the prevalence of government stunting at the national level and then issue various policies and regulations that are expected to contribute to reducing prevalence stunting, including Minister of Health Regulation (Permenkes) No.15/2013 concerning Procedures for Providing Special Facilities for Breastfeeding and/or Milking, 23/2014 concerning Efforts to Improve Nutrition [12, 13].
Many factors cause a high incidence of stunting in infants. The direct cause is a lack of food intake and the presence of infectious diseases [14]. Other factors are lack of mother's knowledge, wrong parenting, poor sanitation and hygiene, and poor service. In addition, people do not realize that short children are a problem because short children in the community are seen as children with normal activities, unlike thin children who must be dealt with immediately. Likewise, maternal nutrition during pregnancy, the community has not yet realized the importance of nutrition during pregnancy contributing to the nutritional state of the baby to be born later [12, 15].
Based on the background description, the researchers are interested in conducting research on the description of oral hygiene, and quality of life-related to dental and oral health in patients with stunting in Enrekang Regency.
Type of this study is an observational analytic cross-sectional study design. This research was conducted in Enrekang District, Buntu Batu, Baraka and Malua Subdistricts in 6 elementary schools, namely SDN 94 Balla, SDN 20 Baraka, SDN 114 Balombong, SDN 24 Malua, SDN 106 Panyurak, and SDN 5 Pasui on April 29- May 3, 2019. The target population of this study is stunting children aged 6-12 years in three districts with the highest prevalence of stunting in Enrekang District, namely Baraka, Malua, and Buntu Batu Subdistricts. Willing to participate in the entire series of studies. Height and caries status checks were performed on 405 children, but 71 students did not return and complete the questionnaire. A total of 334 children participated in the study which filled out the questionnaire in full.
Height measurements are measured with an accuracy of 0.1 centimeters. Height data were then converted into a BMI z score for age and a high z score for age with the WHO AnthroPlus software, which uses the WHO 2007 Growth reference. Stunting is defined as a high-for-age z score <-2SDS; score ≥-2SD is classified as not stunting [12].
Assessment of oral hygiene using the OHI-S index. OHIS score:[16]
The degree of oral hygiene clinically associated with OHI-S scores are as follows:
Good: If the score is 0.0 - 1.2
Medium: If the score is 1.3 - 3.0
Poor: If the score is 3.1 - 6.0
Quality of life of children aged 8-10 years related to oral health is measured using the Child Perception Questionnaire (CPQ8-10). 4 domains are covering 25 questions contained in CPQ8-10 namely oral symptoms, functional limitations, emotional well-being and social well-being (attached). There are also questions about you and other people (attached). The response format for 25 questions is based on a Likert Scale. Each question is given a score of 0-4 (0 for never, 1 for once/twice, 2 for sometimes, 3 for often and 4 for almost every day/every day). A score of 0-2 is categorized as having no impact, and a score of 3-4 is considered as having an impact. The total score can vary from 0-100. A high score indicates a greater dental and oral health impact on the quality of life, meaning lower OHRQoL. Conversely, if a low score indicates dental and oral health less impact on the quality of life, it means that OHRQoL is high [17]. Quality of life of children aged 11-14 years related to oral health is measured using the Child Perception Questionnaire (CPQ11-14). 4 domains are covering 37 questions contained in CPQ11-14 namely oral symptoms, functional limitations, emotional well-being and social well-being (attached). Each question is given a score of 0-4 (0 for never, 1 for once/twice, 2 for sometimes, 3 for often and 4 for every day). A score of 0-2 is categorized as not having an impact, and a score of 3-4 is categorized as having an impact. The total range of scores obtained from 0 to 148. A high score indicates a greater impact on dental and oral health on quality of life, meaning a low OHRQoL. Conversely, if a low score indicates dental and oral health less impact on the quality of life, it means that OHRQoL is high [18].
Data were processed using the Statistical Package for Social Science/ SPSS software system version 25.0. the type of data used is primary data.
Permission was obtained from Faculty of Dentistry, Ethics and Research Advisory Committee, Hasanuddin University. Informed consent was obtained from all the subjects.
Results
Table 1 shows a descriptive description of the sociodemographic characteristics of the study sample used for children in the 6-12 year age group. The number of samples is 123 people. Based on sex, there were more 65 male samples. Based on ethnicity and religion, most people are Bugis tribes with 90 people, and Islam with 123 people.
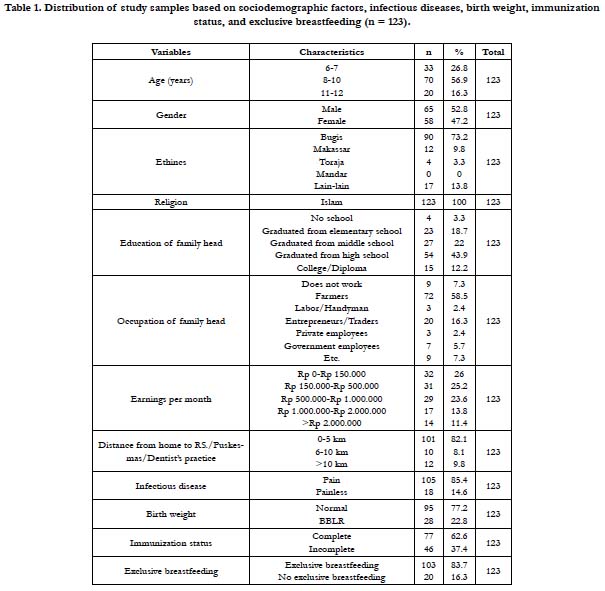

Table 1. Distribution of study samples based on sociodemographic factors, infectious diseases, birth weight, immunization status, and exclusive breastfeeding (n = 123).
Table 2 Distribution of mean OHI-S values based on age and sex of the highest stunting children at 6-7 years old (2.03 ± 0.74). Based on sex the mean value of OHI-S was higher in males (1.83 ± 0.81).
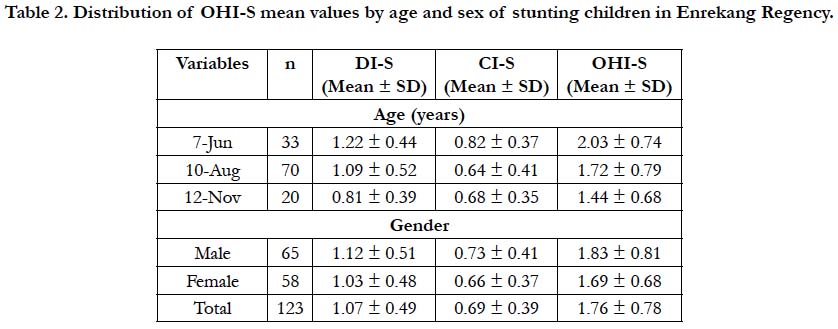
Table 2. Distribution of OHI-S mean values by age and sex of stunting children in Enrekang Regency.
Based on Table 3, the distribution of dental and oral hygiene status of the OHI-S index of stunting children based on age and sex. The results of the clinical examination on oral and dental hygiene status showed that the most oral and dental hygiene status in the medium category were 77 children (62.60%).
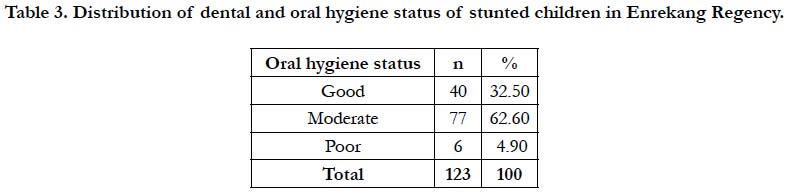
Table 3. Distribution of dental and oral hygiene status of stunted children in Enrekang Regency.
In this examination, only children aged 8-12 years were given CPQ questionnaires, but children aged 6-7 years were not given CPQ questionnaires because CPQ6-7 questionnaires were not developed so far.
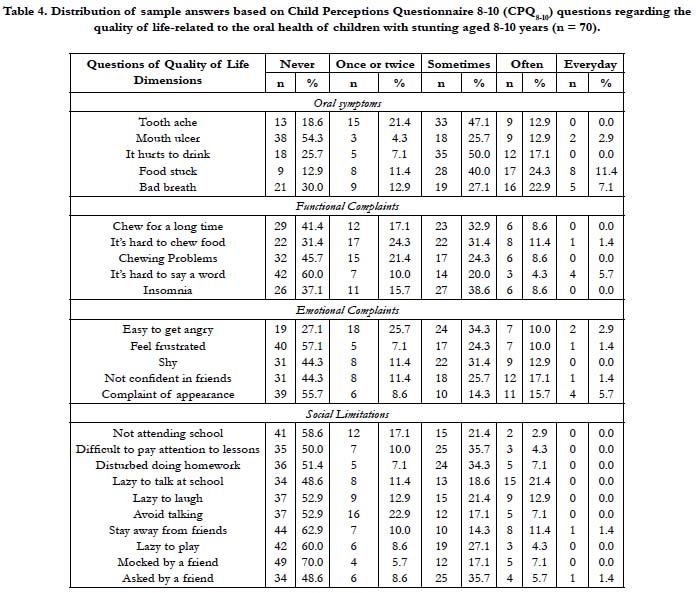
Table 4. Distribution of sample answers based on Child Perceptions Questionnaire 8-10 (CPQ8-10) questions regarding the quality of life-related to the oral health of children with stunting aged 8-10 years (n = 70).
Samples of 8-10 years old as many as 70 people were given a CPQ8-10 questionnaire to assess the oral health related quality of life. In the dimension of oral symptoms, the most frequently complained of children is food stuck to the teeth of 17 children (24.3%). In the functional complaint dimension, the child most often feels that it is difficult to chew food as many as 8 children (11.4%). In the dimension of emotional complaints the most frequently complained of children is a lack of confidence in friends as many as 12 children (17.1%). In the dimension of social limitations, the complaint most often felt by children is lazy to talk in school by 15 children (21.4%).
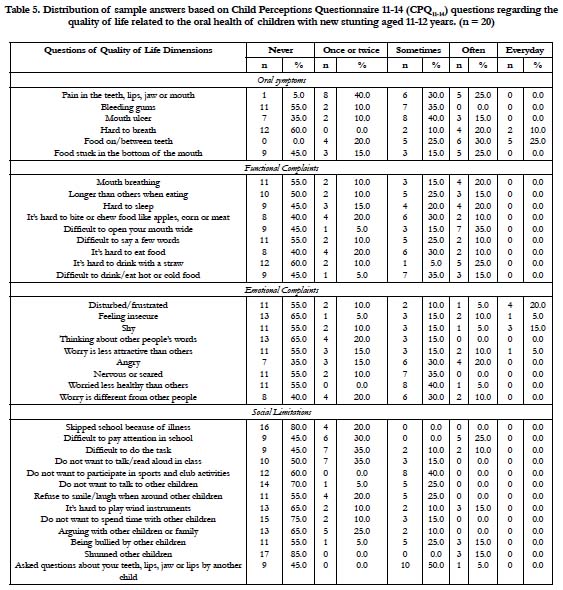
Table 5. Distribution of sample answers based on Child Perceptions Questionnaire 11-14 (CPQ11-14) questions regarding the quality of life related to the oral health of children with new stunting aged 11-12 years. (n = 20)
Samples aged 11-12 years as many as 20 people were given a CPQ11-14 questionnaire to assess the oral health related quality of life. In the dimension of oral symptoms the most frequently complained of children is food in/between teeth as many as 6 children (30%). In the functional limitation dimension, the complaint most often felt by children is that it is difficult to open a wide mouth as many as 7 children (35%). In the dimensions of emotional complaints that most often complained of children are angry because of the influence of teeth and mouth as many as 4 children (20%). On the social limitation dimension, the complaint most often felt by children is that it is difficult to pay attention in schools as many as 5 children (25%).
Discussion
Research on the description of oral hygiene and quality of liferelated to dental and oral health in children with stunting in Enrekang Regency. From the results of the study, 123 samples were obtained.
Based on Table 1 out of a total of 123 samples found in three sub-districts in Enrekang, namely kec. Baraka, Kec. Malua, Kec. Buntu Batu found the highest number of stunting found in Kec. Baraka. Table 2 shows a descriptive description of sociodemographic characteristics based on the age sample of 6-12 years. The number of samples is 123. Based on gender, there are more male samples, as many as 65 people, based on ethnicity and religion, most of which are Bugis as many as 90 people, and Islam as many as 123 people.
Table 3 presents data on clinical examination results in the study sample. Based on age, the highest OHIS is at the age of 6-7 years. Based on sex, the average OHIS values were higher in males. Based on Table 4 presents data on the results of the clinical examination of oral and dental hygiene status based on the OHIS index obtained the most oral and dental hygiene status in the medium category of 80 children. This is similar to previous research in Manado caused by the attitudes and behavior of girls who are more likely to pay attention to appearance compared to boys, while the value of knowledge from boys is almost the same as women, so the high level of children's knowledge about dental health affects hygiene teeth and mouth is supported by the attitude and behavior of the child. It can also be influenced by the knowledge and attention of parents by teaching and supervising a child's daily life in maintaining oral hygiene [19-21].
Child Perceptions Questionnaires (CPQ) were used in this study to assess the quality of life of children with stunting aged 8-10 and 10-14 years. CPQ is a self-reported questionnaire. Many studies have shown that children's reports about health-related quality of life are valid and reliable. There was no assessment of the quality of life at age 6-7 in this study, because CPQ6-7 has not yet been developed [18].
Based on table 5 distribution of answers to quality of life questions related to oral health samples aged 8-10 years as many as 70 people were given a CPQ8-10 questionnaire to assess the quality of life-related to oral health. On the dimensions of oral symptoms the most frequently complained of children is food stuck to the teeth, on the dimensions of functional complaints that most often children feel is difficult to chew food, on the dimensions of emotional complaints that most often complained of children is lack of confidence in friends, on the dimension of social limitations complaints the most often felt by children is lazy to talk at school. This is the same as research conducted in Brazil, the percentage of functional limitations most frequently experienced by respondents is a difficulty when eating. Caries can cause food easily stuck in cavities, causing discomfort and pain, which can cause chewing disorders and decreased appetite [22, 23].
In 8-10 years the child can already understand the nature or condition about himself and is also able to assess themselves which are shown in the form of emotions. Emotions that are commonly experienced at this stage of development are anger, fear, jealousy, curiosity and pleasure or happiness. Emotion is a dominant factor that influences a child's behavior. Children are often not able to hold emotions, children's emotions tend to appear and even excessive. This may be the cause of the emotional dimension most often experienced and cause interference with children [24].
Based on table 6 shows the distribution of answers to quality of life questions related to oral health samples aged 11-12 years as many as 20 people were given a CPQ11-14 questionnaire to assess the quality of life-related to oral health. In the dimension of oral symptoms, the most frequently complained of children is food in/between teeth, in the dimensions of functional limitations the most frequent complaints of children feel is difficult to open wide mouth. on the dimensions of emotional complaints that most often complained of children are angry because of the influence of teeth and mouth, on the dimension of social limitations the complaints that are most often felt by children are Difficult to pay attention to in school. The results of this study are higher than previous studies in children in Brazil, which are a pain in the teeth, lips, and jaw, difficult to drink hot or cold drinks [25].
Based on the dimensions of the condition of oral symptoms, functional complaints, emotional, and social limitations children who have never felt the complaint has the highest percentage. This is likely because children with a good quality of life have more numbers than children who have a poor quality of life. Previous studies have been carried out in Spain, the samples studied were children aged 6, 12 and 15 years and are residents of developed countries. The results of this study indicate that the sample distribution regarding the quality of life is relatively low. This can happen because most likely the sample already has good knowledge and practice the importance of maintaining oral health [26].
Conclusion
Based on the results of the research that has been done it can be concluded that children who experience stunting in Enrekang District have moderate oral hygiene status and based on the dimensions of quality of life, stunting children have the most complaints on the dimensions of oral symptoms.
References
- Situation of Short Toddler (Stunting) in Indonesia, data and information center, Republic of Indonesia Ministry of Health. Health Data and Information Window Bulletin 2018: p. 1-3 ISSN: 2088-270X
- World Health Organization, Multi-Center Growth Study Group. WHO child growth standards based on length/height, weight and age. Acta Paediatr . 2006; 450: 76–85.
- Anindita P. Relationship of mother's education level, family income, adequacy of protein & zinc with stunting (short) in toddlers aged 6 - 35 months in Tembalang District, Semarang City. Journal of Public Health, Diponegoro University. 2012; 1 (2): 617 - 626.
- Anugraheni HS, Kertasurya MI. Risk factors for stunting in children aged 12-36 months in Pati District, Pati Regency. Journal of Nutrition College. 2012; 1 (1): 30- 37.
- RISKESDAS. 2007 Indonesia Basic Health Research Report. Jakarta: Republic of Indonesia Ministry of Health, 2007.
- RISKESDAS. Report on Indonesian Basic Health Research Results in 2010. Jakarta: Ministry of Health Republic of Indonesia, 2010.
- Ministry of Health of the Republic of Indonesia. Basic Health Research 2013. Ministry of Health Health Research and Development Agency. Jakarta: 2013.
- Secretariat of the Vice President of the Republic of Indonesia. 100 Districts / Cities Priority for invertence of stunted children Summary (stunting). Jakarta: National Team for the Acceleration of Poverty Reduction. 2017: p. 5-8.
- Pintauli, S. Relationship Analysis of Dental and Mouth Health Behavior Relationship To Dental and Mouth Health Status of Elementary and Middle School Students in Medan. Journal of Education and Culture.2010: 16.
- Novita, C. F., Andriyany, P., S. I. M. Comparison of the Effectiveness of Poster and Cartoon Animation Counseling Media on Knowledge of Dental and Oral Health. Journal of the Syiah Kuala Dentistry Society. 2016; 1 (1): 65–72.
- UNICEF. Expanded global databases stunting April 2019. New York: UNICEF; 2019.
- Minister of Health of the Republic of Indonesia. Regulation of the Minister of Health Number 15 of 2013 concerning Procedures for Providing Special Facilities for Breastfeeding and / or Expressing Breast Milk Indonesia; 2013. http://www.kesjaor.kemkes.go.id/documents/01_Permenkes%20 No.15%20thn%202013%20ttg%20Facilities%20Special%20Milfeeding% 20and%20Merah%20ASI.pdf
- Minister of Health of the Republic of Indonesia. Minister of Health Regulation No. 23 of 2014 concerning Efforts to Improve Nutrition. Indonesia; 2014. http://sinforeg.litbang.depkes.go.id/upload/regulasi/PMK_No._23_ttg_Upaya_Perbaikan_Gizi_.pdf
- UNICEF. Improving child nutrition: the achievable imperative for global progress. New York: UNICEF; 2013.
- Onis MD, Blossner M, Borghi E. Prevalence and trends of stunting among pre-school children1990–2020. Public Health Nutrition 2011, 15(1): 6
- Wei H. Y., Lang P. N. Periodontal Epidemiological Indices for children and adolescents: II. Evaluation of Oral Hygiene; III. Clinical Applications. The American Pedodontics; 1962; 4 (2); 64-66.
- Hadzipasic A, Nazdrajic. Validation of the Child Perceptions Questionnaire 8-10 in Bosnia and Herzegovina. Materia socio medica 2012; 24(3): 157-9.
- Bekiroglu N,Bakkal M, Ozbay G, Karadeniz PG, Kargul B. Validity and reliability of Child Perception Questionnaire (CPQ11-14) by Rasch Analysis in Turkish children. Pediatric Dental Journal 2017;27(1): 14-20.
- Sampakang T, Gunawan PN, Juliatri. oral hygiene status of children aged 9-11 years according to the habit of brushing their teeth the night before going to sleep at SDN Melonguane. Journal of e-Dentistry (eG) 2015; 3 (1): 5.
- Ningsih D. S. Relationship of Gender To Oral Hygiene of Orphanage Children; Odonto Dental Journal: 2015: 2 (1): 4.
- Zetu I., et al. Gender Variations in the Psychological Factors as Defined by the Theory of Planned of Oral Hygiene Behavior: Procedia – Social and Behavioral Sciences: 2014: 5.
- Ramos-jorge J, Pordeus IA, Ramos-jorge ML, Marques LS, Paiva SM. Impact of untreated dental caries on quality of life of preschool children: different stages and activity.
- Piovesan C, Batista A, Ferreira F, Ardenghi T. Oral health-related quality of life in children: Conceptual issues. Dental Research Journal 2009; 24(1): 81-85.
- Riza M, Suharso A. Increasing Emotional Maturity through Content Mastery Services with Playing Techniques (Games). Indonesian Journal of Guidance and Counseling. 2014; 3 (1): 30-31.
- Abanto J, Thiago S, Fausto M, Marcia T, Bunecker M, Daniela P. Impact of oral disease and disorder on oral health-related quality of life of preschool children. Community Dent Oral Epidemid. 2011;39: 105-14.
- Almerich-Silla JM, Boronat-Ferrer T, Montiel-Company JM, Iranzo-Cortes JE. Caries prevalence in children from Valencia using ICDAS II criteria. Med Oral Patol Oral Cir Bucal. 2014;19 (6): e574-80.





