Rehabilitation of Bilateral Cleft Lip and Palate in Adult Patient with Modification of Maxillary Overlay Cobalt Chromium Obturator
Noorhayati Raja Mohd*, Enas Etajuri Abdalla, Yusnidar Tajul Ariffin, Muaiyed Mahmoud Buzayan
Faculty of Dentistry, Department of Restorative Dentistry, University of Malaya, Malaysia.
*Corresponding Author
Noorhayati Raja Mohd,
Faculty of Dentistry, Department of Restorative Dentistry, University of Malaya, Malaysia.
Tel/Fax: +60379674814
E-mail: hayatiraja@um.edu.my
Received: September 14, 2020; Accepted: October 02, 2020; Published: October 07, 2020
Citation:Noorhayati Raja Mohd, Enas Etajuri Abdalla, Yusnidar Tajul Ariffin, Muaiyed Mahmoud Buzayan. Rehabilitation of Bilateral Cleft Lip and Palate in Adult Patient with Modification of Maxillary Overlay Cobalt Chromium Obturator. Int J Dentistry Oral Sci. 2020;7(10):840-843. doi: dx.doi.org/10.19070/2377-8075-20000165
Copyright: Noorhayati Raja Mohd©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Cleft lip and palate can result indiscontinuity of the oral-nasal and maxillary sinus cavities. It can have a devastating effect on a patient's appearance and speech. Prosthetic rehabilitation is usually required to cover the defect and to restore normal functions. Retention of the obturator is a significant problem while rehabilitating large defects. A suitable technique for fabrication should be selected to achieve this. This article presents the prosthodontic rehabilitation of a congenitally bilateral cleft lip and palate on an adult patient with a distinct method to fulfill the patient's needs, esthetics, and psychological well-being. The treatment plan was to provide her with maxillary overlay cobalt-chromium obturator. A cobalt-chromium framework with a special design was fabricated to aid in the retention. The antral bulb, which covers the defect, was modified and fabricated with a distinctive hollow design. Aesthetics was achieved and patient- reported satisfaction with the outcome.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Bilateral Cleftlip and Palate; Cobalt-Chromium Maxillary Obturator; Maxillary Obturator.
Introduction
Rehabilitating patients with cleft lip and palate with missing
foremost teeth and insufficient alveolar ridge presents a difficult
task for the dental practitioner. A comprehensive rehabilitation
strategy that includes multidisciplinary treatment planning by
surgeons, orthodontists, and restorative dentists should be considered
for each case [1]. While bone grafting and orthodontics
are the preferred treatment for the cleft area; several patients are
rehabilitated with a variety of prosthetic treatment, including
conventional implant-supported removable partial dentures, fixed
prosthodontic treatments, multi-unit veneered resin bonded, fiber-
reinforced composite resin bonded, a removable partial denture
with extra coronal attachment and combination of fixed and
removable dental treatment [2, 3]. The aim of maxillofacial prosthetic
rehabilitation is to restore the esthetic and functional health
of patients with craniofacial defects. Prosthetic rehabilitation is
typically required in the form of a palatal obturator to replace the
defect and promote better oral functions. This enables patients to
eat and drink during mastication without fear of having food or
drink, reaching the oro-nasal and oro-antral cavities. In the cases
of patients with minimal dentition, the application of an obturator
becomes even more difficult as the mechanism of retention is
compromised. A palatal obturator provides better retention and
stability and requires proper design for long-term use. The conventional
method has a hollow antral part but usually a solid oral
part, which adds to the weight of the prosthesis, pressurizing the
soft tissues, which affects the function and esthetics. This article
demonstrates the modification of the antral bulb, which covers
the defect. It was designed considering the potential difficulties
shared by the patient is wearing the conventional closed hollow
bulb design. This technique, when followed, was beneficial in reducing
the weight of the prosthesis and enhancing retention and
allowed the patient to perform regular functional movements.
Case Report
A 48 years old Chinese lady was referred to the Department of
Restorative at the University Malaya, Malaysia, due to her complaint
of looseness of the maxillary obturator following repeated
fracture of her denture, which leads to difficulty in eating and
chewing. She was diagnosed with a complete repaired bilateral
cleft of the lip, primary and secondary palates. Partial medical history
revealed that she underwent multiple cleft repaired surgery and had been wearing an obturator for more than 20 years. The
present obturator was fabricated in 2010 with numerous repairs
that had been made. Clinical examination revealed severe loss of
dental hard tissue with the presence of sizeable oro-nasal fistula
with little or no alveolar ridge, especially on the right side. Displaceable
tissues were noted surrounding the defect area (Figure
1). The radiographic findings revealed a generalized horizontal
bone loss of 2/3 root length of teeth with no alveolar bone noted
on the anterior region present, and radiopacity noted on the
right and left zygoma region indicating the plate screw (Figure
2). Treatment planning was to provide her with maxillary overlay
cobalt-chromium obturator.
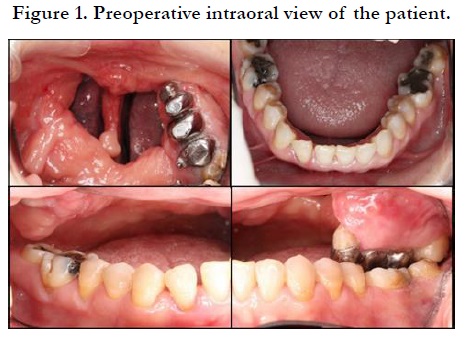

Figure 1. Preoperative intraoral view of the patient.
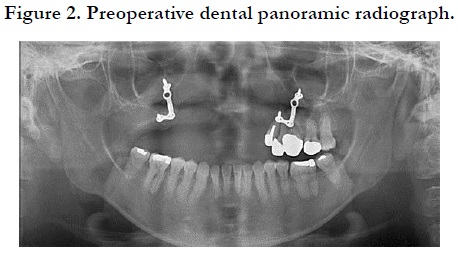
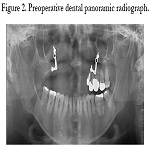
Figure 2. Preoperative dental panoramic radiograph.
The primary model of each jaw was made. Maxillary final impressions were taken using regular body polyvinyl siloxane impression material (GC Exaflex regular, GC America, Alsip, USA). It was poured with type III dental stone (Elite Rock, Zhermack SpA, Via Bovazecchino, Badia Polesine, Italy) to produce a working cast (Figure 3). The master cast are duplicated, and the refractory cast was obtained. The unique design of the framework was made with overlay coping with cobalt-chromium (Figure 4(a) and 4(b)). Fitting was done intraorally (Figure 4(c)). Maxilla-mandibular relationship in centric relation was registered and transferred on a semi-adjustable articulator (Protar Evo 5, Kavo, Illinois, USA), and teeth setting were done (Figure 5). The wax obturator was tried in the patient's mouth and checked for correct extension and aesthetic. Then, the obturator was processed with an open hollow bulb design. The prosthesis was issued to the patient after confirming the stability, retention, and the patient's comfort. On subsequent review visit (four weeks followed by six months), the patient was pleased as her aesthetic and functional compromised has been restored and met her expectation).
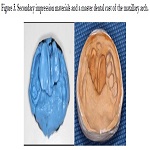
Figure 3. Secondary impression materials and a master dental cast of the maxillary arch.
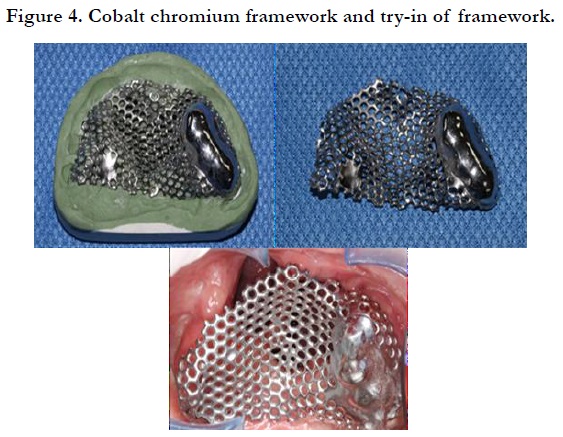
Figure 4. Cobalt chromium framework and try-in of framework.
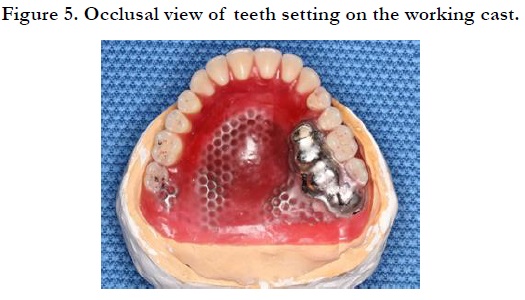
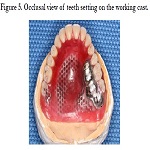
Figure 5. Occlusal view of teeth setting on the working cast.
Discussion
For this patient, treatment consisted of providing her an overlay
cobalt-chromium open bulb obturator. In this case, the presence
of a large oro-nasal fistula dramatically compromised the stability,
retention, and support for the denture. The non-resilient nature
of the peripheral tissues can make it challenging to achieve
an adequate peripheral seal. Based on the technique mention by
research, the utilization of the metal crown coping as an overdenture
will slightly improve the retention and stability of the obturator
[4]. According to same study, the portion of the overlay denture,
which in direct contact with the dentition, should never be
made with acrylic resin. The porous resin harbors a multitude of
microorganisms, and as a result, the overlaid dentition will soon
become carious despite good oral hygiene [4]. The risk of caries
of the overlaid dentition will be substantially reduced if the portion of the prosthesis that overlays the dentition is fabricated
in metal. Rehabilitation with an obturator prosthesis on a larger
defect area could be problematic because its vertical extension
has to be large enough to cover the entire defect making it heavy,
uncomfortable, and challenging to adapt to [5]. Obturators can
be fabricated in an open or closed hollow prosthesis with many
different methods available [6]. It is known that the open hollow
bulb obturator is easier to fabricate and adjust. However, it is difficult
to polish and clean the open hollow bulb obturator. The
polishing process on the fitting surfaces of the acrylic part, that
located in the defect zone, can be considered as a pool, cannot
be performed thoroughly [7]. This may lead to the accumulation
of food and nasal secretions inside the hollow part and, in turn,
leads to malodor, an increase in weight, and chances of infection.
Relatively, in this case, the design of the open obturator was
chosen and was design such a way for the patient to clean it easily.
The wall height of the obturators entering specific proportions
within the nasal defect contributes to the separation, stability, and
retention; therefore, it can lead to better aesthetic and phonation
of the patient. The shape and height of the obturator wall are
essential, but it should be noted that the weight of the obturator
will also lead to the loss of restraint and even to the dislodgement
forces in the supporting teeth [8, 9]. Furthermore, the extension
of the obturator was made into the nasal defect area to achieve
the retention and stability of the prosthesis. Open space obturators
with a low medial wall height have been reported to be more
successful as compared to the closed bulb [10]. Concerning the
nasal extension, with these types of unfavorable defects, it may
be beneficial to extend the obturator into the nasal aperture or
onto the nasal surface of the soft palate to augment retention. According to Pigno and Funk 2001, total engagement of the nasal
aperture space will significantly increase obturator retention [11].
When completely engaging the space area, it is crucial to access
a specific insertion route that is commonly used for placement
and removal of the obturator. Fabrication of such design, in this
case, was to improve the weight, retention, and stability of the
prosthesis.
Acknowledgement and Declarations
We want to express our appreciation to our dedicated prosthetic
laboratory assistant for their excellent job in the constructions of
the prostheses and also our dental surgery assistant who had assisted
in the treatment sessions. There are no conflicts of interest
among the authors regarding the publication of the manuscript.
References
- Dogan E, Dogan EI,Dogan S. Interdisciplinary treatment approaches for cleft lip and palate patients to obtain esthetic and functional results. J. Dent. Oral Hyg. 2019; 11(1):1-5.
- Freitas JA, Garib DG, Oliveira M, LaurisRde C, Almeida AL, Lucimara Teixeira Neves, et al. Rehabilitative treatment of cleft lip and palate: Experience of the hospital for rehabilitation of craniofacial anomalies USP (HRAC USP) – Part 2: Pediatric dentistry and orthodontics. J Appl Oral Sci. 2012; 20(2):268-281.Pubmed N PMID: 22666849.
- Geethu RM, Anilkumar S. Esthetic and Functional Rehabilitation of an Adult Cleft Lip and Palate Patient Using Combined Fixed and Removable Prosthesis. Journal of Interdisciplinary Dentistry. 2018 Jan 1;8(1):35.
- Beumer III J, Marunick MT, Esposito SJ. Maxillofacial rehabilitation: prosthodontic and surgical management of cancer-related, acquired, and congenital defects of the head and neck. Quintessence Pub. 2011;276.
- Kumar VA, Hofstede TM, Ginsberg LE. CT imaging features of obturator prostheses in patients following palatectomy or maxillectomy. AJNR Am J Neuroradiol. 2011; 32(10): 1926-1929. Pubmed PMID: 21799037.
- Deogade SC, Mantri SS, Naitam D, Dube G, Gupta P, Dewangan A. A direct investment method of closed two-piecehollow bulb obturator. Case Reports in Dentistry. 2013;2013:326530.Pubmed PMID: 23936685.
- Sharaf MY, Ibrahim SI, Eskander AE, Shaker AF. Prosthetic versus surgical rehabilitation in patients with maxillary defect regarding the quality of life: systematic review. Oral Maxillofac Surg. 2018; 22(1):1-11. Pubmed PMID: 29388055.
- Breeze J, Rennie A, Morrison A, Dawson D, Tipper J. Health-related quality of life after maxillectomy: obturator rehabilitation compared with flap reconstruction. Br J Oral Maxillofac Surg. 2016; 54(8):857-862.Pubmed PMID: 27266975.
- Wang F, Huang W, Zhang C, Sun J, Qu X, Yiqun Wu. Functional outcome and quality of life after a maxillectomy: a comparison between an implant supported obturator and implant supported fixed prostheses in a free vascularized flap. Clin Oral Implants Res. 2017; 28(2):137-143. PubmedPMID: 26725478.
- Litty Francis. Rehabilitation of a patient with palatal defect- A case report. Journal of Surgery and Surgical Research. 2017;11(3):ZD19-ZD20.PubmedPMID: 28511525.
- Pigno MA, Funk JJ. Augmentation of obturator retention by extension into the nasal aperture: A clinical report. Journal of Prosthetic Dentistry. 2001; 85(4):349-51.Pubmed PMID: 11319531.





