Comparative Evaluation of Efficacy of Endodontic Irrigant Delivery to Working Length using Conventional Needle Syringe, Endovac and Self-Adjusting File System on Prepared Mesiobuccal Canal of Mandibular First Molar by using Radiographic Contrast Media: An In Vivo Study
Abrar S1, Jaiprakash R2*, Mahala H3, Naviwala GA4, Ramugade M5, Sapkale K5
1 Professor (Academics) & Head of Department, Department of Conservative Dentistry and Endodontics, Government Dental College & Hospital, Mumbai, India.
2 Associate Professor in Dentistry,Government Medical College, Aurangabad, India.
3 Private practitioner, Dahanu, Palghar District, India.
4 Medical officer (Dental), Directorate of Health Services, Mumbai, India.
5 Associate Professor, Department of Conservative Dentistry and Endodontics, Government Dental College & Hospital, Mumbai, India.
*Corresponding Author
Dr. Jaiprakash Ramchandra Rathod,
Associate Professor in dentistry, Government Medical College, Aurangabad, Maharashtra, India.
Tel: +91 90297 71903
E-mail: drjprathod@gmail.com
Received: September 01, 2019; Accepted: October 31, 2019; Published: December 11, 2019
Citation:Bashir Ahmed SA, Ramchandra Rathod J, Mahala H, Anwar NG, Ramugade M, Sapkale K. Comparative Evaluation of Efficacy of Endodontic Irrigant Delivery to Working Length using Conventional Needle Syringe, Endovac and Self-Adjusting File System on Prepared Mesiobuccal Canal of Mandibular First Molar by using Radiographic Contrast
Media: An In Vivo Study. Int J Dentistry Oral Sci. 2019;6(6):706-710. doi: dx.doi.org/10.19070/2377-8075-19000139
Copyright: Ramchandra Rathod J©2019. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Endodontic treatment is essentially a debridement procedure, followed by sealing of pulp space and restoration of tooth.
Aim: To compare the efficacy of endodontic irrigant delivery to working length using conventional needle syringe, EndoVac and Self Adjusting file system on prepared mesiobuccal canal of mandibular first molar using radiographic contrast media.
Materials and Methods: 60 patients, who were scheduled for root canal treatment of Permanent First Molars, were randomly selected. The prepared mesiobuccal canals were then assigned into 3 different groups for evaluation of irrigant delivery using radiographic dye. Different irrigation protocol was performed for each group.
Results: The analysis of variance test showed statistically significant differences between groups (<0.001) Tukey’s honestly significant post hoc tests showed significant statistical differences between group 1 (the conventional needle and syringe irrigation) and group 2 (the EndoVac) and group 1 and group 3 (the Self-adjusting file system) (P <0.001). No significant difference was observed between group 2 and group 3 (P =0.080).
Conclusion: To do a better cleaning of the root canals, the delivery systems and techniques which are proven superior and safe, such as EndoVac and Self-adjusting file should be integrated in routine clinical practice. This will not only enhance cleaning but also the quality of the final sealing and ultimately enhance overall success.
2.Introduction
3.Materials & Methods
3.1 Inclusion Criteria
3.2 Exclusion Criteria
3.3 Statistical Analysis
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Endodontic Treatment; Root Canal Irrigation; EndoVac; Self-Adjusting File.
Introduction
Endodontic treatment is essentially a debridement procedure, followed by sealing of pulp space and restoration of tooth. Endodontic procedures can be divided into three basic phases’ namely diagnostic phase, preparatory phase and obturation phase. The preparatory phase which is considered to be the most important, comprises of chemo mechanical debridement for the purpose of elimination of pulpal tissue, microbiota, their by-products, organic and inorganic debris by using instruments and intracanal irrigants [1]. All this is done to prevent spread of infection and create an environment conducive for regeneration and repair the periapical tissues. Studies have demonstrated that mechanical instrumentation alone cannot sufficiently disinfect root canals even by modern rotary Ni-Ti instrumentation techniques [2, 4]. So, complete cleaning and shaping involves irrigation with chemicals along with mechanical instrumentation. Mechanical instrumentation involves establishing a specific cavity form which permits easy access to the root canal space. Instruments mainly shape the canals and irrigants further perform the function of cleaning. The irrigant can penetrate and reach complicated micro anatomical features of the canal where the instruments can’t. Specific canal shape created by instrumentation facilitates delivery and action of the irrigant to all the parts of complex root canal system. A variety of chemicals have been proposed and promoted for this purpose. An ideal irrigant kills the bacteria, dissolve the necrotic tissue, lubricate the canal, remove the smear layer and does not irritate healthy tissues [2]. It is important that, the irrigant is brought into the contact with the entire canal surfaces over its total micro anatomic complexity for effective action, particularly in the apical portions of root canals where it is most complex and crucial [3].
Conventionally a needle and syringe have been used to deliver the irrigant to the root canal systems for debridement and remains widely practiced. However, it has been demonstrated that the flushing action of syringe irrigation is not sufficient as theirrigation solution was delivered only 1 mm deeper thanthe tip of the needle [4]. Lately, for irrigant delivery different irrigation techniques and devices have been introduced in an attempt to successfully deliver the irrigant to the working length such as Endobrushes, NaviTip FX, Manual-dynamic agitation: hand-activated well-fitting gutta-percha points, Rotary brushes, continuous irrigation during rotary instrumentation, Sonic devices, Ultrasonic devices, Pressure alternation devices (EndoVac, RinsEndo) and Self-Adjusting file. The recently introduced EndoVac and Self- Adjusting file which is being used to provide inherent irrigation seem to be the promising options for the better irrigation delivery [2].
Manufacturers of Self-Adjusting file and EndoVac claim that, by usingtheir systems the irrigant reaches apical one third very effectively [5-7]. However, clinical data for confirmation of the same is scanty. Hence the study was proposed for comparative evaluation of efficacy of endodontic irrigant delivery to working length using conventional needle syringe, EndoVac and Self Adjusting file system on prepared mesiobuccal canal of mandibular first molar using radiographic contrast media.
Materials & Methods
For this in vivo study 60 patients, irrespective of gender, above 16 years of age, who were scheduled for root canal treatment of Permanent First Molars, were randomly selected from scheduled appointment system of the Department of Conservative Dentistry and Endodontics. Ethical clearance was obtained from institutional ethics committee.
• Mandibular first permanent molar with intact mesial root with two canals.
• Teeth having sufficient tooth structure to allow the placement of rubber dam.
• Radiographic evidence of periapical radiolucent lesion and externalroot resorption.
• Calcified canals evident on radiograph.
• Incompletely formed roots.
• Anatomical variations such as extremely curved canals.
• Apparently narrow roots in which apical preparation with #35 file would be overzealous.
• Patient allergic to anything used in this procedure especially rubberdam material and Iohexol (radiographic contrast media).
• Medically unfit patient.
Instruments used for diagnosis, access preparation and shaping included Mouth mirror, Probe, Explorer, Tweezer, DG 16 (API Germany) Air rotor hand piece (NSK Japan), Micro motor with contra angle hand piece (NSK Japan), Endo access burs (MDT Israel), Disposable needle and syringe, Disposable suction tip (Capri), Endodontic hand k-files, Gates Glidden drills, Mtwo rotary file system (VDW, Munich, Germany), EDTA (prep canal), Rubber dam kit (Hygenic, Coltene, Whaledent), Local anaesthetic solution (with adrenaline) - Xicaine 2% with Adrenaline 1 in 80,000 (ICPA Health Products Ltd), Normal saline (Aculife Healthcare Pvt Ltd), Sodium hypochlorite- 5%(Dentpro, Amdent) and Iohexol (Omnipaque) (GE Healthcare USA).
Systems used for endodontic irrigation:
• Syringe and 27-guage side venting needle (Miraject Endotec Duo, Hager Werken, Germany)
• EndoVac system (Kerr Endodontics, Orange, CA)
• Self-adjusting File system (ReDent-Nova, Ra'anana, Israel)
Other equipments:
• X-SMART (Dentsply Maillefer)
• Apex Locator - iRoot (Meta Systems, Korea)
• Endoblock mini (Dentsply Maillefer)
• RVG Machine and Sensor (Planmeca)
The selected patients were given complete information about the purpose, aim, objectives and methodology of the study & written consent was taken from the patients who were willing to participate. The Intraoral Periapical Radiographs of the mandibular first molars of the selected patients were examined and those first molars with two completely formed roots having two mesial canals were chosen for further investigations. Access opening was made under local anaesthesia and rubber dam adhering to all the standard norms. Working length was determined by tactile, electronic method and confirmed by radiographic method by keeping 0.5mm short of the apex. All mesiobuccal canals were prepared with Mtwo (VDW, Munich, Germany) rotary files to size 35/0.04. The canals were irrigated with 2ml of 5% sodium hypochlorite between each file during whole preparation procedure with syringe irrigation. The prepared mesiobuccal canals were then assigned into 3 different groups for evaluation of irrigant delivery using radiographic dye.
Group 1- Conventional needle syringe irrigation (n=20)
Group 2- EndoVac irrigation system (n=20)
Group 3- Self-Adjusting file system (n=20)
Different irrigation protocol was performed for each group.
• For Conventional needle syringe irrigation (Group 1): a 27-gauge side-vented needle was placed into the deepest possible position and without binding the wall of the root canal. Then the canal was irrigated with 2ml of Iohexol (omnipaque) with a flow of 1ml per minute.
• For EndoVac (Group 2): 2ml of iohexol contrast medium was delivered in pulp chamber and was suctioned with macro cannula at middle third of the root canal and then micro cannula placed at working length adhering to manufacturer’s instructions.
• For self-adjusting file system (Group 3): 2ml of iohexol contrast medium was delivered through the hollow file by silicone tube attached to its hub when self-adjusting file system in operation at a setting of 5000 vibrations/min and flow rate of 4ml/min for period of 30 seconds adhering to manufacturer’s instructions.
Now with the contrast medium inside the canal, a digital radiographic image (Planmeca) was obtained for each tooth and then the distance between working length and maximum irrigant penetration was measured and evaluated on RVG software (Apixia, CA, USA). After obtaining digital radiographs, radiographic contrast media was eliminated from the canal system by using aspiration with needle syringe and copious irrigation using normal saline solution. Endodontic therapy of the teeth was completed according to the standard treatment protocol.
The responses were coded and entered in Microsoft excel and analyzed using IBM SPSS statistics 20.0 [IBM Corporation, Armonk, NY, USA]. Descriptive and inferential statistical analyses were carried out in the present study. Results on continuous measurements were presented on Mean ± SD. Level of significance was fixed at p=0.05 and any value less than or equal to 0.05 was considered to be statistically significant. Analysis of variance (ANOVA) was used to find the significance of study parameters between the groups (Inter group analysis). Further post hoc analysis was carried out if the values of ANOVA test were significant.
Results
A total of 60 patients participated in the study with equal number of patients in each group. The results of the statistical analysis were as follows: Group 1 (The conventional needle and syringe irrigation)-showed longest distances between working length and maximum irrigant penetration, with mean distance of 1.88 + 0.35mm. Group 2 (The EndoVac) - showed shortest distance between working length and maximum irrigant penetration, with mean distance of 0.10 + 0.14mm. Group 3 (The self-adjusting file system) showed mean distance of 0.28 + 0.27mm. The analysis of variance test showed statistically significant differences between groups (<0.001) Tukey’s honestly significant post hoc tests showed significant statistical differences between group 1 (the conventional needle and syringe irrigation) and group 2 (the EndoVac) and group 1 and group 3 (the Self-adjusting file system) (P <0.001). No significant difference was observed between group 2 and group 3 (P =0.080).
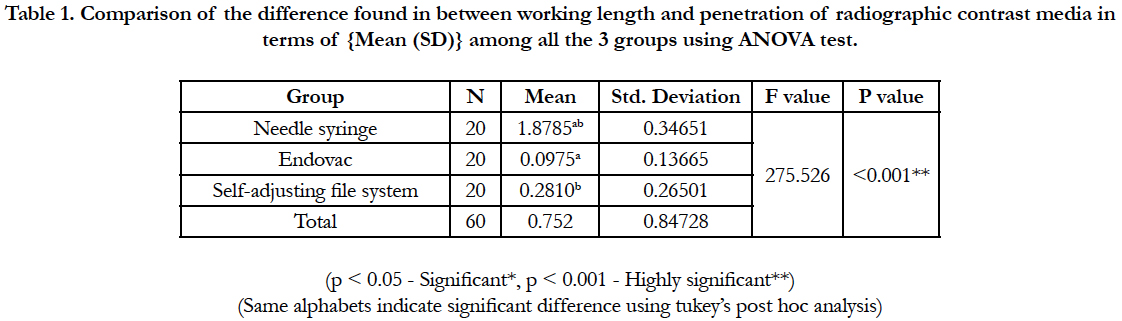

Table 1. Comparison of the difference found in between working length and penetration of radiographic contrast media in terms of {Mean (SD)} among all the 3 groups using ANOVA test.
Discussion
This study was undertaken for determining and comparing the delivery of irrigating solutions (depth of penetration) using the conventional needle syringe, EndoVac and self-adjusting file system. 60 patients, irrespective of gender, above 16 years of age, which were appointed for root canal treatment of Permanent Mandibular First Molars, were randomly selected from scheduled appointment system of the Department of Conservative Dentistry and Endodontics.
The findings of this study revealed that group 1 (the conventional needle syringe group) was effective at delivering the endodontic irrigant to the coronal and middle third of the working length of root canal but was ineffective in doing so at the apical third. Thus on the basis of the results of this study, it can be stated that irrigation only with needle syringe may not be sufficient for proper cleaning of the root canals to the full working length.
Initial work in this regard was done by Chow (1983) [4] where, he concluded that, the apical extent of effectiveness of irrigation is function of the depth of needle insertion. In his in vitro study he used glass tubes having internal diameters and taper along with bead-form gel stained with ink to simulate clinical situation. This in vivo study was done on the same line and substantiates this finding by Chow. Walters et al., (2002) [8] in an in vitro study on extracted teeth produced similar results as this study. They used measurement of residual debris from the canal after irrigation with needle syringe to evaluate the efficacy of the irrigation. Rodig T et al., (2010) [9], in an in vitro study used sonic device (Vibringe), syringe irrigation, and passive ultrasonic irrigation and found out syringe irrigation was not better at the apical third of the root canal in the removal of debris from simulated root canal irregularities.
Earlier in vivo study in this concern was done by Salzgeber et al., (1977) [10] on canals of molar tooth, results of which were not in accordance with our study. In this study he evaluated the penetration of an irrigating solution in root canals using hypaque (radiographic dye) as an irrigation solution and concluded that when root canals are prepared serially by a flaring technique, the irrigating solution penetrates to the full depth of instrumentation. The different findings might be because, the canals were irrigated with hypaque using needle syringe at every step. The pulp chamber was irrigated, working length was taken and instrumentation was done till size #30, at this point the irrigant remained short of the apex. After this the canal was further enlarged to size #35 by file and #2 Gates-Glidden drill, this may have agitated the irrigant in the canal and allowed it to reach till the full working length. One of the samples used in this study also showed extrusion of contrast media periapically.
Khan et al., (2013) [11], did an in vitro on extracted teeth and examined fluid pressure generated by canal cleansing devices at the apical interface, when tip of the irrigation device was not binding to the canal walls. In the study author found that needle syringe irrigation with flow higher than 1ml/min may lead to extrusion of irrigant periapically. Tay et al., (2010) [12], did an in vitro study to examine the effect of vapor lock on canal debridement efficacy. The author studied this effect by testing the difference between a ‘‘closed’’ and an ‘‘open’’ system design in smear layer and debris removal by using a side-vented needle for irrigant delivery. The study showed a significant score of debris in closed system suggesting presence of vapour lock adversely affecting debridement efficacy. In the present in vivo study we had 27-guage needle placed deep inside the root canal without binding the canal walls and possible care was taken to maintain the irrigation flow at 1ml/ minutes (manually) to ensure the safety of the irrigation. We used radiographic contrast media that allowed us to evaluate the efficacy of irrigant delivery into the canal in real clinical situation. In this study we found needle syringe irrigation may not be efficient in delivery of irrigant to the full working length. This finding of our study is also in accordance with Neilson and Baumgartner [6], Munoz HR [13], Siu and Baumgartner [14], de Gregorio et al., [15], Shin et al., [16], Shen et al., [17], F. Palazzi [18], Mancini et al., [19], Kara tuncer and Unal [20], Thomas et al., [21].
In this study the EndoVac irrigation system which operates on negative pressure technique showed consistently better results in delivering endodontic irrigant to the full working length. Neilson and Baumgartner (2007) [6] in an in vitro study on extracted teeth compared efficiency of EndoVac and needle syringe irrigation by finding debridement efficacy at apical 1mm from working length. The results of their study were on similar line as the present study. Siu and Baumgartner (2010) [14] did an in vivo study in which teeth were instrumented and irrigated with needle syringe irrigation and EndoVac system. These teeth were then extracted, sectioned and evaluated for debris. This can be regarded as the best method so far to evaluate the efficacy of cleaning. However, the findings of their study were similar to this study. Results of our study are in accordance with an in vitro study by F. Palazzi et al., (2012) [18] where teeth were irrigated and evaluated under scanning electron microscope for smear layer, found out that the EndoVac system was better in removal of smear layer at all levels. In the present study Self-adjusting file which acts on no pressure irrigation technique for irrigating the root canals simultaneously along the instrumentation also showed better irrigation at the apical third as compared to needle syringe irrigation. The result of our study matched with the results of experimental set up by Metzger (2014) [22] in which the simulated canal in the transparent block was filled with green liquid, representing irrigant present in the canal. Afterwards this canal was operated with self-adjusting file system with red liquid representing fresh sodium hypochlorite solution and time was calculated. It was found out that 30 seconds were required for the total replacement of the irrigant in the apical part. In our study we have operated self-adjusting file system for irrigation with radiographic dye into the canal after preparation for 30 seconds. The results of our study also showed the penetration till the working length.
Conclusion
Based on the findings of the current study and body of literature discussed so far it can be stated that, in an in vivo cleaning and shaping, the root canals being enclosed by bony socket and periodontal ligament acts as a closed channel system. This closed channel system hinders the conventional needle syringe irrigation efficiency. So to do a better cleaning of the root canals, the delivery systems and techniques which are proven superior and safe, such as EndoVac and Self-adjusting file should be integrated in routine clinical practice. This will not only enhance cleaning but also the quality of the final sealing and ultimately enhance overall success.
References
- Weine FS. Basis for successful endodontics.6th ed. Endodontic therapy. Mosby: Elsevier; 2004. p.1- 23.
- Peters OA, Peters CI. Cleaning and shaping of the root canal system.10th ed. KM Hargeaves, S Cohen, editor. Pathways of the Pulp.Mosby Elsevier, St. Louis, MO; 2011:288–348.
- Gao Y, Haapasalo M, Shen Y, Wu H, Li B, Ruse ND, et al.Development and validation of a three dimensional computational fluid dynamics model of root canal irrigation. J Endod. 2009 Sep;35(9):1282-7. PubMed PMID: 19720232.
- Chow TW. Mechanical effectiveness of root canal irrigation. J Endod.1983 Nov; 9(11):475-9.
- Schoeffel GJ. Apparatus for evacuation of root canal. US8827705B2; 2004.
- Nielsen BA, Baumgartner JC. Comparison of the EndoVac system to needle irrigation of root canals. J Endod. 2007 May;33(5):611-5.
- Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974 Apr;18(2):269-96. PubMed PMID: 4522570.
- Walters MJ, Baumgartner JC, Marshall JG. Efficacy of irrigation with rotary instrumentation. J Endod. 2002 Dec;28(12):837-9.
- Rödig T, Bozkurt M, Konietschke F, Hülsmann M. Comparison of the Vibringe system with syringe and passive ultrasonic irrigation in removing debris from simulated root canal irregularities. J Endod. 2010 Aug;36(8):1410-3. PubMed PMID:20647107.
- Salzgeber RM, Brilliant JD. An in vivo evaluation of the penetration of an irrigant solution in root canals. J Endod 1977;3(10):394-8. PubMed PMID: 270543.
- Khan S, Niu LN, Eid AA, Looney SW, Didato A, Roberts S, et al. Periapical pressures developed by nonbinding irrigation needles at various irrigation delivery rates. J Endod. 2013 Apr;39(4):529-33. PubMed PMID: 23522551.
- Tay FR, Gu LS, Schoeffel GJ, Wimmer C, Susin L, Zhang K, et al. Effect of vapor lock on root canal debridement by using a side-vented needle for positivepressure irrigant delivery. J Endod. 2010 Apr;36(4):745-50. PubMed PMID: 20307757.
- Munoz HR, Camacho-Cuadra K. In vivo efficacy of three different endodontic irrigation systems for irrigant delivery to working length of mesial canals of mandibular molars. J Endod. 2012 Apr;38(4):445-8. PubMed PMID: 22414827.
- Siu C, Baumgartner JC. Comparison of the debridement efficacy of the EndoVac irrigation system and conventional needle root canal irrigation in vivo. J Endod. 2010 Nov;36(11):1782-5. PubMed PMID: 20951287.
- de Gregorio C, Estevez R, Cisneros R, Paranjpe A, Cohenca N. Efficacy of different irrigation and activation systems on the penetration of sodium hypochlorite into simulated lateral canals and up to working length: an in vitro study. J Endod. 2010 Jul;36(7):1216-21. PubMed PMID: 20630302.
- Shin SJ, Kim HK, Jung IY, Lee CY, Lee SJ, Kim E. Comparison of the cleaning efficacy of a new apical negative pressure irrigating system with conventional irrigation needles in the root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Mar;109(3):479-84. PubMed PMID:20219604.
- Shen Y, Gao Y, Qian W, Ruse ND, Zhou X, Wu H, et al. Three-dimensional numeric simulation of root canal irrigant flow with different irrigation needles. J Endod. 2010 May;36(5):884-9. PubMed PMID: 20416439.
- Palazzi F, Giardino L, Mohammadi Z, Rengo S, Riccitiello F. Debridement effectiveness of two different techniques using negative pressure irrigation system. Giornale Italiano di Endodonzia. 2012 Nov 1;26(3):117-27.
- Mancini M, Cerroni L, Iorio L, Armellin E, Conte G, Cianconi L.Smear layer removal and canal cleanliness using different irrigationsystems (Endo- Activator, EndoVac, and passive ultrasonic irrigation): field emission scanning electron microscopic evaluation in an in vitro study. J Endod. 2013 Nov;39(11):1456-60. PubMed PMID: 24139274.
- Tuncer AK, Ünal B. Comparison of Sealer Penetration Using the EndoVac Irrigation System and Conventional Needle Root Canal Irrigation. J Endod 2014;40:613–617. PubMed PMID: 24767552.
- Thomas AR, Velmurugan N2, Smita S2, Jothilatha S2. Comparative evaluation of canal isthmus debridement efficacy of modified Endo- Vac technique with different irrigation systems. J Endod. 2014 Oct;40(10):1676-80. PubMed PMID: 25052146.
- Metzger Z. The self-adjusting file (SAF) system: An evidence-based update. J Conserv Dent. 2014;17(5):401-19. PubMed PMID: 25298639.





