Prevalence of Developmental Enamel Defects of Primary Incisors in Preterm Infants delivered with Extremely Low Birth Weight
Merglova V1*, Dort J2, Koberova-Ivancakova R3
1 Dentistry Department, Faculty of Medicine Charles Univ. and Univ. Hospital in Pilsen, Alej Svobody Pilsen, Czech Republic.
2 Department of Neonatology, Faculty Hospital in Pilsen, Alej Svobody Pilsen, Czech Republic.
3 Dentistry Department, Faculty of Medicine Charles Univ. and Univ. Hospital in Hradec Kralove, Sokolská Hradec Kralove, Czech Republic.
*Corresponding Author
Vlasta Merglova, PhD,
Associate Professor, Department of Dentistry, Faculty Hospital,
Alej Svobody 80, 323 00 Pilsen, Czech Republic.
Tel: +420377104763
Fax: +420377104720
E-mail: merglovav@fnplzen.cz
Received: April 10, 2019; Accepted: May 08, 2019; Published: May 10, 2019
Citation:Merglova V, Dort J, Koberova-Ivancakova R. Prevalence of Developmental Enamel Defects of Primary Incisors in Preterm Infants delivered with Extremely Low Birth Weight. Int J Dentistry Oral Sci. 2019;6(4):691-696. doi: dx.doi.org/10.19070/2377-8075-190000136
Copyright: Merglova V©2019. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Preterm infants with extremely low birthweights (ELBW) suffer from neonatal complications and morbidity that may affect mineralization of primary teeth and occurrence of developmental enamel defects (DDE). The purpose of the study was to determine and compare the prevalence of DDE in primary incisors of infants delivered with ELBW and full–term normal birthweight (NBW) infants.
Methods: Infants were enrolled in the study at birth and follow–up visits were conducted at 12 months of chronological and corrected age. Personal and anamnestic data were obtained through interviews with parents and from medical hospital records. DDE were recorded on primary incisors according to the Modified developmental defects of enamel index. The data were statistically analyzed using descriptive statistical analysis, chi – square test, odd ratio and 95% CI. A statistical significance level of p < 0.05 was established.
Results: The case cohort included 50 infants with mean gestational age 26, 95 weeks and with mean birthweight 775.74 g. The control cohort comprised 58 infants with mean gestational age 39.6 weeks and with mean birthweight 3418.62 g. DDE of primary incisors were diagnosed in 54% of the ELBW infants and in 6.9% of the NBW infants. DDE were found in 11.25% of 400 teeth examined in the case group, while in the control group only in 1.7% of 464 incisors. Most of the teeth with DDE in the case group was situated in the upper jaw.
Conclusion: ELBW infants presented a significantly higher prevalence of DDE in the primary incisors than NBW infants.
2.Abbreviations
3.Introduction
4.Materials and Methods
4.1 Study design and subjects
4.2 Dental examination
4.3 Statistical methods
4.4 Ethical considerations
5.Results
5.1 Characteristics of subjects
5.2 Prevalence of DDE
6.Discussion
7.Conclusion
8.Acknowledgements
9.References
Keywords
Developmental Enamel Defect; Enamel Hypomineralization; Enamel Hypoplasia; Extremely Low Birthweight; Preterm Infant.
Abbreviations
ELBW: Extremely Low Birth Weights; NBW: Normal Birth Weight; LBW: Low Birth Weight; VLBW: Very Low Birth Weight; ILBW: Incredibly Low Birth Weight; DDE: Developmental Defects of Enamel.
Introduction
Developmental enamel defects (DDE) may be defined as aberration in the quality and quantity of dental enamel [1]. The clinical appearance and severity of DDE are usually dependent on the stage of tooth development during which the insult occurs as well as the extent and duration of the insult. Based on the quality and quantity of affected enamel, DDE can be classified into three main types: hypoplasia, demarcated opacities and diffuse opacities. Enamel hypoplasia is a quantitative defect and presents as a loss of enamel and a decreased enamel thickness such as pits, grooves or lack of superficial layer [2]. Enamel hypomineralization or opacity is a qualitative enamel deficiency presenting as alteration in the translucency of the enamel which may be diffuse or demarcated and colored white, yellow or brown. If a tooth showed both enamel hypoplasia and opacity, it was categorized as combined defect [3]. The etiology of DDE is not yet fully understood. Defects in the enamel structure can only occur during formation of this hard dental tissue. The etiology of enamel hypoplasia is probably a disturbance of short duration caused by incomplete deposition of immature enamel produced by ameloblasts during the secretory stage [4, 5]. Trauma or systemic diseases can be responsible for enamel hypoplasia. Prolongated disturbances play an important role in the etiology of enamel opacities. The enamel hypomineralization occurs as a result of incomplete mineralization or maturation of the enamel [5]. Excessive intake of fluorides, effect of antibiotics, malnutrition or chronic diseases may be responsible for diffuse opacities. The demarcated opacities may be connected with trauma or general diseases over a longer period.
DDE may cause esthetic problem, tooth sensitivity, risk of attrition, plaque accumulation in cases of hypoplasia, increased caries susceptibility and in severe cases even space loss and malocclusion [6-8]. Hypoplastic porous enamel constitutes a pathway for bacteria and other stimuli that may affect the pulp [9, 10]. DDE in primary dentition may be predictive of enamel distribution in the permanent dentition [11].
DDE in primary teeth are the best studied and most noticeable complications of prematurity and low birthweight. Prematurity can be classified as mild when the infant is born between the 32nd and 36th weeks of gestation; moderate, if the birth occurs between the 31st and 28th weeks; or extreme, if the gestational age is less than or equal to 27 weeks. A low birthweight (LBW) is established as weighing less than 2500g, regardless of the gestational age. Low birthweight neonates are subdivided into very low birthweight (VLBW) infants with birthweights <1500g, extremely low birthweight (ELBW) infants with birthweights <1000g and incredibly low birthweight (ILBW) infants [12].
Preterm infants with VLBW and ELBW are very susceptible to all the complications of premature birth both in the immediate neonatal period and during childhood [13]. They have a short prenatal period and are at great risk for early and late morbidity involving, for example, neonatal hypocalcemia, hyperbilirubinemia, perinatal asphyxia, respiratory, cardiovascular, gastrointestinal, neurological problems and nutritional deficiencies, as well as possible disabilities and impediments affecting physical growth and mental development.
The preterm and VLBW or ELBW delivery may affect development and growth of the orofacial region, including primary and permanent teeth. The primary teeth have a long prenatal and postnatal process because the primary incisors start developing at around 6-7 intrauterine weeks and continue for a few months after birth [14]. The onset of the calcification process in primary teeth starts at 14 intrauterine weeks and continues up to the first year of postnatal life. The critical period of primary teeth development and growth occurs very early prenatally. Dental enamel of primary teeth in preterm infants is abnormal in surface quality and significantly thinner compared to enamel of full-term infants. The thinner enamel is due mainly to reduced prenatal growth and results in smaller dimensions of the primary dentition [15].
The aim of the present study was to determine the prevalence of DDE in primary incisors of preterm infants delivered with ELBW and to compare the findings with one-year old full-term infants delivered with NBW. We hypothesized that prevalence of DDE in primary incisors would be significantly higher in preterm infants with ELBW than in full-term NBW infants.
All infants were enrolled in the present case-control study at birth by the Department of Obstetrics, Faculty Hospital in Pilsen, Czech Republic. Preterm ELBW Caucasian infants of both genders were recruited during a three-year study period (2014-2016). All preterm ELBW neonates were treated according the same principles during their hospitalization in the intensive care unit. Follow-up visits were conducted at 12 months of chronological and corrected age. Corrected age was considered, i.e. chronological age reduced by the number of weeks before 40 weeks of gestation. Personal information including gender, gestational age, birthweight, general health status, antibiotic use and self-reported socio-economic status of the family were obtained through interviews with parents and from medical hospital records. The gestational age was estimated from the result of sonography examination.
Infants were eligible for the study if they met the following inclusion criteria for case group: (1) gestational age <37 weeks; (2) birthweight <1000 g; (3) corrected age 12 months; (4) the presence of all primary incisors in the oral cavity; (4) self-reported middle class socioeconomic status of family. During the neonatal period, all ELBW infants received antibiotic treatment consisting of intravenous ampicillin and gentamicin. When intubation had been indicated during the hospitalization in the intensive care unit, the nasal intubation had always been used. Infants with genetic syndromes and malformations diagnosed in the neonatal period were excluded from the study. Of the 77 examined ELBW infants, 50 were selected based on the inclusion and exclusion criteria (Figure 1).
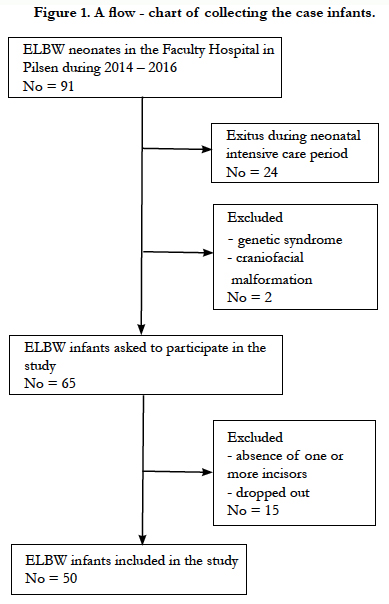
Figure 1. A flow - chart of collecting the case infants.
The inclusion criteria for control group of infants were: (1) chronological age 12 months; (2) gestational age >37 weeks; (3) birthweight >2500g; (4) the presence of all primary incisors in the oral cavity; (5) self-reported middle class socio-economic status of the family. Infants with genetic syndromes, congenital malformations, antibiotic treatment and morbidity in neonatal period were excluded. Of the 70 one-year old full-term infants, 58 were selected for the control group.
All participants of the study were residents of communities with low natural fluoride content (< 0.3 ppm) in drinking water.
Dental examination of ELBW and NBW infants was performed by one previously trained calibrated examiner at the Paediatric Dentistry Department of the Medical Faculty and Faculty Hospital in Pilsen, Czech Republic. The dental examiner was blinded to the groups of infants. The infants were examined using a sterile dental mirror, dental probe and artificial light. The teeth were dried with gauze, then dental mirror and probe were used to detect developmental defects of enamel (DDE). DDE were recorded on the labial surface of each primary incisor. The defects measuring less than one millimeter were excluded and where any doubt exists concerning the presence of DDE, the tooth was scored as without enamel defect. The number and type of teeth with enamel defects was registered. The alteration of enamel was classified according to the Modified developmental defects of enamel index, suggested by the Commission on Oral Health, Research and Epidemiology[1]. The color photographs showing typical examples of different types of DDE were used as a tool in scoring the teeth for the enamel defects. Qualitative changes in enamel translucency without loss of enamel surface were categorized as demarcated or diffuse opacities. The demarcated opacities were described when enamel with normal thickness and intact surface displayed alteration in enamel translucency of variable degree. It is demarcated from the adjacent normal enamel with clear boundaries, and may present a white, creamy, yellow, or brown color. The diffuse opacities comprise alteration in enamel translucency of variable degree and white color. There is no clear demarcation between the adjacent normal enamel and the opacity. The opacities were differentiated from the white spot carious lesions based on color, texture, demarcation and relationship to gingival margin. Hypoplasia is a defect affecting the enamel surface, presenting reduction in enamel thickness and can manifest itself in the form of pits, grooves or other quantitative surface loss. If both enamel defects existed in one tooth they were recorded as combined defect.
To evaluate the reproducibility of the examination used, 19 (10%) of the infants were randomly selected for re-examination. Kappa values were calculated 0.6 for enamel opacities and 0.9 for hypoplasias.
The obtained data were statistically analyzed using Statgraphics software distributed by Stat Point Technologies, Inc. of Warrenton, Virginia, USA. Descriptive statistical analysis (percentage, means, standard deviation) were calculated. Chi-square test was used in order to compare mean birthweight, mean gestational age and prevalence of DDE in case and control group of infants. The relationship between prevalence of DDE in case and control group was evaluating using chi – square test. A statistical significance level of p<0.05 was established Odd ratio and 95% confidence interval were calculated using the online tool Med Calc.[online://www.medcalc.org/calc/odds_ratio.php].
Ethical approval for the investigation was obtained from the Research Ethics Committee Faculty of Medicine in Pilsen, Charles University in Prague, Czech Republic. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 1983. All infants were recruited from the Department of Neonatology of the Faculty Hospital in Pilsen, Czech Republic. Before the study, the legal guardians of all infants provided informed consent for their children to participate in the study.
A definitive case group was composed of 50 one-year old preterm infants delivered with ELBW (27 boys i.e. 54% and 23 girls i.e. 46%). A control cohort comprised 58 one-year old full term infants with NBW (34 boys i.e. 65.5% and 24 girls i.e. 34.5%). Table 1 presents the characteristics of both groups of infants concerning gestational age and birth weight.
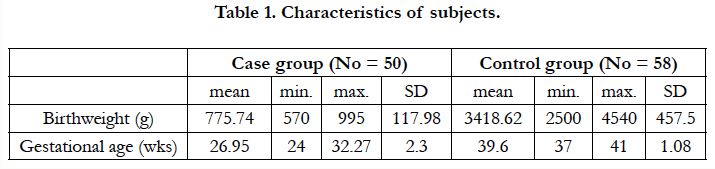

Table 1. Characteristics of subjects.
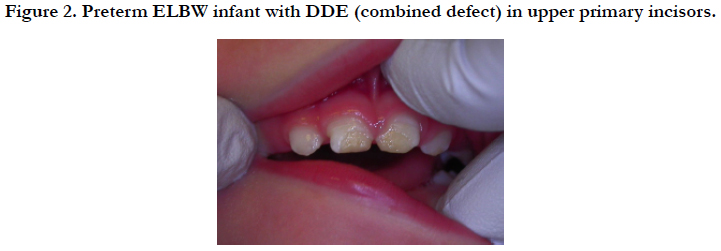

Figure 2. Preterm ELBW infant with DDE (combined defect) in upper primary incisors.
DDE (hypoplasia, hypomineralization and combined defect) of primary incisors was diagnosed in 27 (54.0%) of the preterm ELBW infants and in four (6.9%) of the full-term NBW infants. The difference between the case and control cohort was statistically significant (chi-square test, p < 0.001). In the present study, the main defect found was enamel hypoplasia (Figure 2). The hypoplastic changes of primary incisors were present in 17 (34.0%) of ELBW infants and in two (3.45%) of the control group. The difference concerning prevalence of enamel hypoplasia between case and control group was statistically significant (chi-square test, p <= 0.001, OR = 14.42, 95% CI: 3,113 - 66.41). The preterm ELBW were 14.42 times more likely than infants of control group to develop hypoplasia of enamel. The hypomineralization (diffuse or demarcated opacities) of enamel in primary incisors was found in eight (16.0%) of the case group infants and in two (3.45%) of control group. The higher prevalence of opacities in the case group was statistically significant (chi-square test, p = 0.024, OR = 5.33, 95% CI: 1.08 - 26.43) (Table 3). The case group of infants had 5.33 times more likely to occur hypomineralization of enamel. The combined defect of enamel was diagnosed only in wo preterm ELBW infants (4 %) (Table 2).
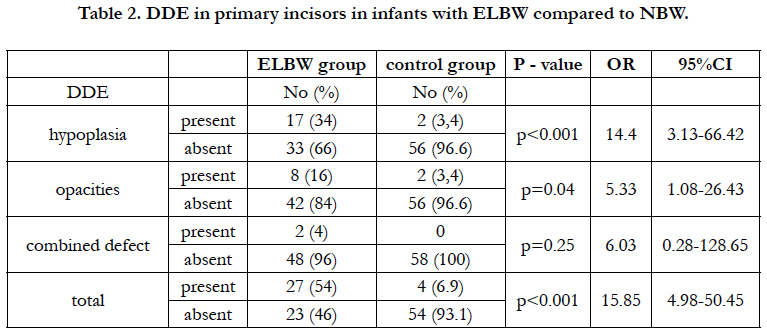
Table 2. DDE in primary incisors in infants with ELBW compared to NBW.
DDE were found in 45 (11.25 %) of 400 teeth examined in the case group, while in the control group only in eight (1.7%) of 464 teeth. The hypoplasias of enamel were detected in 22 teeth (5.5%) of case group and in four teeth (0.9%) of control cohort. The hypomineralizations of enamel were found in 19 teeth (4.8 %) of research group and in four teeth (0.8 %) of control infants. The combined defects of enamel were detected only in four teeth (1%) of case group. The distribution of DDE in primary incisors of premature ELBW infants is shown in Table 3. Most of the teeth with DDE in the case group were situated in the upper jaw (42 i.e. 93.3%) compared to just three instances (6.7 %) in the lower jaw. In the control group of infants all teeth with DDE were localized in the upper jaw. 24 (57.1%) of all primary incisors with DDE were situated in the left part of upper jaw and 18 (42.9%) incisors were in the right side.
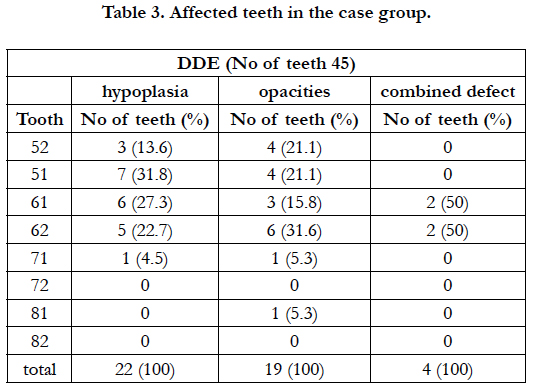
Table 3. Affected teeth in the case group.
Discussion
DDE in primary and permanent dentition, delayed tooth eruption and oral defects associated with endotracheal intubation are a well-researched complication of prematurity and low birthweight [3, 16-18]. Other oral disturbances in preterm infants include notching of the alveolar ridge, palatal grooving, high arch palate, crossbite, palatal asymmetry and smaller dimensions of primary and permanent clinical crowns [19]. The best studied and most noticeable complications of prematurity and low birthweight are developmental disturbances of primary teeth enamel [20]. The best time for diagnosis of DDE is soon after tooth eruption because DDE in primary or permanent teeth can be lost by traumatic dental injuries, attrition or caries [21]. Therefore, the infants in the present study were only 12 months old in terms of chronological or corrected age at the moment of dental examination. On the other hand, the examination of very young uncooperative infants is difficult, especially so as regards the diagnosis of diffuse opacities.
DDE in primary dentition in healthy children of various age groups has been evaluated to occur at rates ranging between 4 - 75% [11, 22, 23] depending on the population studied and the criteria used for scoring. The prevalence of DDE in primary dentition described by Correa-Faria P. et al., [22] has been 29.9% and demarcated opacities were the most frequent type of enamel defects. In contrast, in some studies diffuse opacities were the most common defect of primary teeth enamel [23, 24]. The reported prevalence of DDE in primary incisors in the control group of the present study was 6.9%.
The prevalence of DDE in primary dentition has been reported to be higher in preterm infants delivered with LBW or VLBW and may vary between studies from 16% of cases to as many as 96% [6, 22, 25-28]. In the present study the prevalence of DDE in oneyear old ELBW infants was 54% and in the control group 6.9%. In the literature [27-30] the prevalence of opacities in the primary dentition of preterm children is higher than the prevalence of hypoplasia. In the current study the prevalence of opacities was only 18.0% and prevalence of hypoplasia 36.0%. An explanation of these differences could be considerable methodological differences between studies focusing on preterm children, e.g. design, choice of outcomes, study size and diagnostic criteria [5]. It is not possible to compare the prevalence of DDE in primary incisors of ELBW infants in present study with the results of other research because data concerning the ELBW group of children are unavailable in recent literature. Earlier studies were carried out on a higher birthweight and more mature infants than the present research. The reason for the differences in the prevalence of DDE in full-term NBW infants and premature ELBW infants is most likely related to both systemic and local factors. Infants with the most premature birth and lowest birthweight have the highest tendency to suffer from systemic diseases, which can affect dental development [6].
In accordance with other studies [3, 27, 31-33] the occurrence of DDE in present case group was more frequent in the upper than in the lower primary incisors. DDE were predominantly located in the maxillary left (57.1%) over the right (42.9%) part of the dental arch. This situation is in agreement with other studies [33-35] and can be related to trauma from laryngoscopy and endotracheal intubation at the critical period of amelogenesis and may be complicated by derangement of calcium metabolism and other systemic factors. The intubation trauma to oral tissues can occur during elevation of the laryngoscope blade in order to displace tongue back to expose the pharyngeal region. The pressure on the alveolar ridge can affect the upper primary incisors germs [36].
The authors are aware of certain limitations of the present study. The prevalence of DDE was determined only in upper and lower primary incisors in very young uncooperative infants and the sample size was relatively small. Despite this limitation, the present investigation has strength. All infants were born in the same hospital and all case group infants were treated according the same principles during their perinatal hospital care and only one previously trained calibrated examiner performed the evaluation of primary incisors. This study may be the first of its kind, related to DDE in primary incisors of preterm ELBW infants.
Conclusion
One-year old preterm ELBW infants presented a significantly higher prevalence of DDE in the primary incisors than full-term NBW infants. The enamel hypoplasia was the most frequent disturbance in one-year old preterm infants delivered with ELBW. The primary incisors most affected by DDE were situated in the left part of upper jaw.
Acknowledgements
This research was supported by a grant from the Ministry of Health of the Czech Republic – Conceptual Development of Research Organization Faculty Hospital in Pilsen – FNPI, 00669806.
References
- [1]. Commission on Oral Health, Research & Epidemiology. Report of an FDI Working Group. A review of the developmental defects of enamel index (DDE Index). Int Dent J. 1992 Dec;42(6):411-26. PubMed PMID: 1286924.
- Wong HM. Aetiological factors for developmental defects of enamel. Austin J Anat. 2014;1(1):1003.
- Aine L, Backström MC, Mäki R, Kuusela AL, Koivisto AM, Ikonen RS, et al. Enamel defects in primary and permanent teeth of children born prematurely. J Oral Pathol Med. 2000 Sep;29(8):403-9. PubMed PMID: 10972349.
- Crombie F, Manton D, Kilpatrick N. Aetiology of molar–incisor hypomineralization: a critical review. Int J Paediatr Dent. 2009 Mar;19(2):73-83. doi: 10.1111/j.1365-263X.2008.00966.x. PubMed PMID: 19250392.
- Jacobsen PE, Haubek D, Henriksen TB, Østergaard JR, Poulsen S. Developmental enamel defects in children born preterm: a systematic review. Eur J Oral Sci. 2014 Feb;122(1):7-14. doi: 10.1111/eos.12094. PubMed PMID: 24164573.
- Seow WK, Humphrys C, Tudehope DI. Increased prevalence of developmental dental defects in low birth-weight, prematurely born children: a controlled study. Pediatr Dent. 1987 Sep;9(3):221-5. PubMed PMID: 3507638.
- Nelson S, Albert JM, Geng C, Curtan S, Lang K, Miadich S, et al. Increased enamel hypoplasia and very low birthweight infants. J Dent Res. 2013 Sep;92(9):788-94. doi: 10.1177/0022034513497751. PubMed PMID: 23857641.
- Salanitri S, Seow WK. Developmental enamel defects in the primary dentition: aetiology and clinical management. Aust Dent J. 2013 Jun;58(2):133- 40; quiz 266. doi: 10.1111/adj.12039. PubMed PMID: 23713631.
- Sabel N, Klinberg G, Dietz W, Nietzsche S, Norén JG. Polarized light and scanning electron microscopic investigation of enamel hypoplasia in primary teeth. Int J Paediatr Dent. 2010 Jan;20(1):31-6. doi: 10.1111/j.1365-263X.2009.01006.x. PubMed PMID: 20059591.
- Rythén M, Norén JG, Sabel N, Steiniger F, Niklasson A, Hellström A, et al. Morphological aspects of dental hard tissues in primary teeth from preterm infants. Int J Paediatr Dent. 2008 Nov;18(6):397-406. doi: 10.1111/j.1365-263X.2008.00928.x. PubMed PMID: 18637047.
- Casanova-Rosado AJ, Medina-Solis CE, Casanova-Rosado JF, Vallejos – Sánchez AA, Martinez – Mier EA, Loyola – Rodriquez JP, et al. Association between developmental enamel defects in the primary and permanent dentitions. Eur J Paediatr Dent. 2011 Sep;12(3):155-8. PubMed PMID: 22077681.
- World Health Organization. International statistical classification of diseases and related health problems. World Health Organization; 2004.
- Hack M, Fanaroff AA. Outcomes of children of extremely low birthweight and gestational age in the 1990s. Semin Neonatol. 2000 May;5(2):89-106. PubMed PMID: 10859704.
- Avery JK, Chiego DJ. Essentials of oral histology and embryology: a clinical approach. 3rd ed. Elsevier; 2006.
- Seow WK, Young WG, Tsang AKL, Daley T. A study of primary dental enamel from preterm and full-term children using light and scanning electron microscopy. Pediatr Dent. 2005 Sep-Oct;27(5):374-9. PubMed PMID: 16435636.
- Eastman DL. Dental outcomes of preterm infants. Newborn Infant Nurs Rev. 2003 Sep 1;3(3):93-8.
- Al–Rawi BA, Qasim AA, Al–Sayagh GD. The effect of premature birth on the primary dentition. Al-Rafidain Dent J. 2008(7):18-22.
- Bodh M, Jain M, Dutta S, Namdev R, Kumar A. Preterm Birth Complications On Oro-Dental Structures: An Updated Review. J Oral Health Comm Dent. 2015 9(2):85-9. DOI: 10.5005/johcd-9-2-85.
- Angelos GM, Smith DR, Jorgenson R, Sweeney FA. Oral complications associated with neonatal oral tracheal intubation: a critical review. Pediatr Dent. 1989 Jun;11(2):133-40. PubMed PMID: 2668901.
- Zaidi I, Thayath MN, Singh S, Sinha A. Preterm Birth: A Primary Etiological Factor for Delayed Oral Growth and Development. Int J Clin Pediatr Dent. 2015 Sep-Dec;8(3):215-9. doi: 10.5005/jp-journals-10005-1316. PubMed PMID: 26628856.
- Seow WK. Clinical diagnosis of enamel defects: pitfalls and practical guidelines. Int Dent J. 1997 Jun;47(3):173-82. PubMed PMID: 9448804.
- Correa-Faria P, Martins-Júnior PA, Vieira-Andrade RG, Oliveira-Ferreira F, Marques LS, Ramos-Jorge ML. Dental defects of enamel in primary teeth: prevalence and associated factors. Int J Paediatr Dent. 2013 May;23(3):173-9. doi: 10.1111/j.1365-263X.2012.01241.x. PubMed PMID: 22548676.
- Masumo R, Bärdsen A, Ästrøm AN. Developmental defects of enamel in primary teeth and association with early life course evnts: a study of 6-36 month old children in Manyara, Tanzania. BMC Oral Health. 2013 May 14;13:21. doi: 10.1186/1472-6831-13-21. PubMed PMID: 23672512.
- Lunardelli SE, Peres MA. Prevalence ad distribution of developmental enamel defects in the primary dentition of preschool children. Braz Oral Res. 2005 Apr-Jun;19(2):144-9. PubMed PMID: 16292449.
- Velló MA, Martínez-Costa C, Catalá M, Fons J, Brines J, Guijarro-Martínez R. Prenatal and neonatal risk factors for the development of enamel defects in low birth weight children. Oral Dis. 2010 Apr;16(3):257-62. doi: 10.1111/j.1601-0825.2009.01629.x. PubMed PMID: 19849806.
- Lai PY, Seow WK, Tudehope DI, Rogers Y. Enamel Hypoplasia and dental caries in very-low birthweight children.: a case-controlled, longitudinal study. Pediatr Dent. 1997 Jan-Feb;19(1):42-9. PubMed PMID: 9048413.
- Cruvinel VRN, Gravina DBL, Azevedo TDPL, de Rezende CS, Bezerra ACB, Toledo OA. Prevalence of enamel defects and associated risk factors in both dentitions in preterm and full term born children. J Appl Oral Sci. 2012 May-Jun;20(3):310-7. PubMed PMID: 22858696.
- Funakoshi Y, Kushida Y, Heida T. Dental observations of low birth weight infants. Pediatr Dent. 1981 Mar;3(1):21-5. PubMed PMID: 6951147.
- Franco KMD, Line SR, de Moura-Ribeiro MV. Prenatal and neoanatal variables associated with enamel hypoplasia in deciduous teeth in low birth weight preterm infants. J Appl Oral Sci. 2007 Dec;15(6):518-23. PubMed PMID: 19089191.
- Johnsen D, Krejci C, Hack M, Fanaroff A. Distribution of Enamel Defects and the Association with Respiratory Distress in Very Low Birthweight Infants. J Dent Res. 1984 Jan;63(1):59-64. PubMed PMID: 6582082.
- Pimlott JF, Howley TP, Nikiforuk G, Fitzhardinge PM. Enamel defects in prematurely born, low birth-weight infants. Pediatr Dent. 1985 Sep;7(3):218-23. PubMed PMID: 3865161.
- Lin X, Wu W, Zhang CH, Lo ECM, Chu CHH, Dissanayka WL. Prevalence and distribution of developmental enamel defects in children with cerebral palsy in Beijing, China. Int J Paediatr Dent. 2011 Jan;21(1):23-8. doi: 10.1111/j.1365-263X.2010.01075.x. PubMed PMID: 20659182.
- de Oliveira Melo NSF, da Silva RPGVC, de Lima AAS. The neonatal intubation causes defects in primary teeth of premature infants. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2014 Dec;158(4):605-12. doi: 10.5507/bp.2013.004. PubMed PMID: 23446261.
- Cortines AAO, Corrêa-Faria P, Paulsson L, Costa PS, Costa LR. Developmental defects of enamel in the deciduous incisors of infants born preterm: Prospective cohort. Oral Dis. 2019 Mar;25(2):543-549. doi: 10.1111/odi.13011. PubMed PMID: 30537164.
- Seow WK, Brown JP, Tudehope DA, O’Callaghan M. Dental defects in the eciduous dentition of premature infants with low birth weight and neonatal rickets. Pediatr Dent. 1984 Jun;6(2):88-92. PubMed PMID: 6592551.
- Matsumoto T, de Carvelho WB. Tracheal intubation. J Pediatr (Rio J). 2007 May;83(2 Suppl):S83-90. PubMed PMID: 17530140.





