Vertical Facial Height and its Correlation with Skeletal Pattern Among Young Nigerian Orthodontic Patients
Yemitan TA1*, Oludare YS2, Ogunbanjo BO1
1 Faculty of Dentistry, Department of Child Dental Health, Orthodontics Unit, Lagos State University College of Medicine, Lagos, Nigeria.
2 Department of Child Dental Health, Orthodontics Unit, Lagos State University Teaching Hospital, Lagos, Nigeria.
*Corresponding Author
Yemitan T.A,
Faculty of Dentistry, Department of Child Dental Health,
Orthodontics Unit, Lagos State University College of Medicine, Lagos, 2315, Nigeria.
Tel: 2348023056044
E-mail: tolulaseyemitan@yahoo.com
Received: July 30, 2018; Accepted: August 28, 2018; Published: August 29, 2018
Citation:Yemitan TA, Oludare YS, Ogunbanjo BO. Vertical Facial Height and its Correlation with Skeletal Pattern Among Young Nigerian Orthodontic Patients. Int J Dentistry Oral Sci. 2018;5(8):661-666. doi: dx.doi.org/10.19070/2377-8075-18000130
Copyright: Yemitan TA©2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objectives: To compare the anterior facial height parameters among the sexes and to find facial height variations among Class I, II and III skeletal pattern groups.
Methods: The sample comprised of 60 (26 females and 34 males) lateral cephalometric radiographs traced and grouped into Class I, II and III skeletal relationships based on their ANB values. The age of the sample subjects was 10-19 years. The upper, lower and total anterior facial heights and the ratio of upper and lower to the total facial heights were measured and calculated for all radiographs in the three skeletal groups.
Results: The anterior facial heights showed no significant differences between both sexes in the skeletal groups. The anterior facial height parameters studied showed no significant difference among the skeletal groups. None of the facial height variables correlate significantly with skeletal pattern.
Conclusion: The anterior facial heights and its ratios showed no significant sex variation and revealed no significant difference among the skeletal groups.
2.Abbreviations
3.Introduction
4.Materials and Methods
5.Results
6.Discussion
7.Conclusions
8.References
Keywords
Facial Height; Skeletal Pattern; Cephalometrics; Sex Variation.
Abbreviations
AFH: Anterior Facial Height; PFH: Posterior Facial Height; ANS: Anterior Nasal Spine; LAFH: Lower Anterior Facial Height; UAFH: Upper Anterior Facial Height; Me: Menton; N: Nasion; FHP: Frankfort Horizontal Plane; TAFH: Total Anterior Facial Height.
Introduction
In orthodontics, facial forms are classified into long, average and short faces according to the vertical facial dimensions [1]. Generally, vertical dimension includes anterior facial height (AFH) and posterior facial height (PFH). In cephalometry. the lower anterior facial height (LAFH) is defined as the vertical distance between the anterior nasal spine (ANS) and the menton (Me) points, while the upper anterior facial height (UAFH) is the distance between the Nasion(N) and the ANS [2, 3].
The optimal facial aesthetics is closely linked to the vertical facial dimensions, therefore, achieving the ideal vertical facial profile for patients is an important primary objective of orthodontic treatment [4].
Previous researchers based on their findings had emphasized that individuals with malocclusion should not be treated by generic cephalometric analysis, but rather by the individual norm of cephalometric analysis [5-8]. A large variation in the skeletal relationship has been reported in normal occlusion samples [5, 6], thereby suggesting that significant anatomical variations exist in those with normal occlusion and to a greater degree in a malocclusion. Therefore, orthodontic treatment based on cephalometric analysis for a patient using the numerical standards derived from other persons with an average skeletal relationship may not give optimal result.
Many studies on dentoalveolar compensatory mechanism reported have been in favor of a more individualized treatment approach according to the individual’s skeletal type [1, 9-12]. However, they analyzed the skeletal pattern separately as either antero-posteriorly or vertically. To describe all facial types as prognathic or retrognathic may not be adequate [9] and significant variations were identified in classifying facial types in the vertical dimensions. Therefore, it is important to define the multidimensional combinations in order to make a more accurate identification of the facial types because the interrelation of the anteroposterior and vertical relationship is responsible for the various facial types [1, 8, 13]. This would lead to a more precise diagnosis from which a more specific treatment could be planned.
Studies have primarily investigated the distribution of different antero-posterior skeletal pattern, and the vertical facial pattern in some population groups [14-18]. They reported that the same cephalometric norms do not apply to all patients because of racial characteristics, therefore various ethnic groups required their own cephalometric norms.
However, few studies have investigated the relationship between the antero-posterior skeletal jaw relationships and the vertical skeletal facial height. An earlier study of cephalo-facio-dental relationship revealed a high correlation between facial patterns and anterior vertical proportions [19].
The aim of this study was to evaluate the variation of the AFH and its components among the different types of antero-posterior skeletal jaw relationships in Nigerian young patients who live in Lagos, Nigeria.
Materials and Methods
This retrospective study was performed through an examination f lateral cephalograms of 60 consecutive patients (26 females and 34 males) at the Lagos State University Teaching Hospital, Lagos, Nigeria. Ethical clearance was obtained from the institutional ethical review committee prior to the data collection.
The study sample comprised of subjects, aged 10-19 years, who visited the dental clinic for orthodontic treatment. The lateral cephalograms of subjects fulfilling the following inclusion criteria were included in this study: subjects of Nigerian origin, no previous orthodontic or prosthodontic treatment, and no history of trauma or surgery of facial structures.
The lateral cephalograms used in this study were taken on Planmeca ProMax (Planmeca USA Inc, IL, USA) at an exposure of 68KV, 13.0mA and 15.8s. The following measures were taken for each subject to ensure a high degree of precision in obtaining cephalograms: head was fixed in a way that the sagittal plane was at the right angle to the path of the x-rays and the Frankfort Horizontal Plane (FHP) was parallel to the horizontal plane. Teeth were occluded in centric occlusion and lips were maintained in relaxed position.
All radiographs were traced manually by an experienced investigator on acetate paper in a dark room using an x-ray viewer (Slim-Line™ View Box, Select Dental Manufacturing Inc, NY, USA).
The linear and angular measurements were made with the help of a millimeter ruler and protractor, respectively. Corrected values of linear measurements were recorded to eliminate magnification error of 10% (Figure 1). Table 1 shows definitions of abbreviations for cephalometric variables.
Sagittal skeletal pattern was identified using ANB angle (Figure 1), and subjects were divided into three facial groups according to the following criteria [13]:
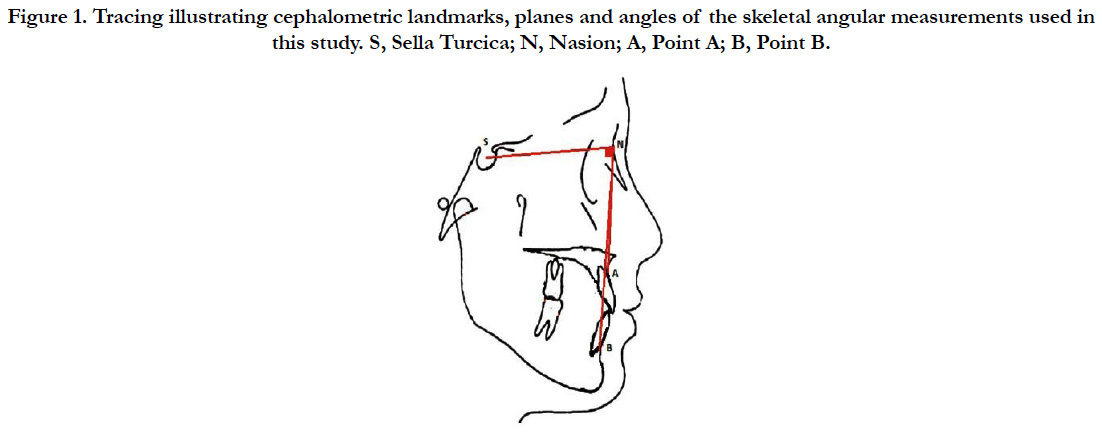
Figure 1. Tracing illustrating cephalometric landmarks, planes and angles of the skeletal angular measurements used in this study. S, Sella Turcica; N, Nasion; A, Point A; B, Point B.
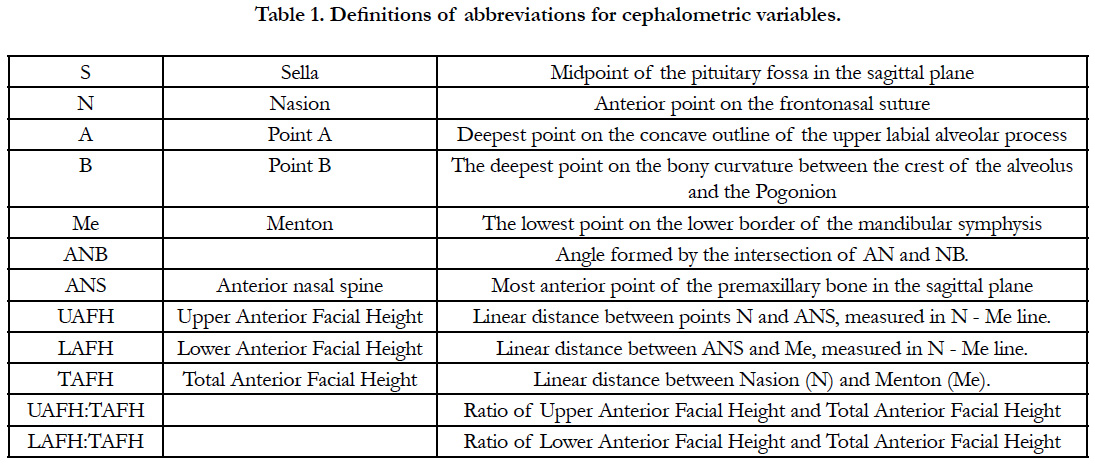

Table 1. Definitions of abbreviations for cephalometric variables.
• Skeletal pattern I: Subjects with ANB value between 2° – 4° (14 subjects)
• Skeletal pattern II: Subjects with ANB value >4° (33 subjects)
• Skeletal pattern III: Subjects with ANB value <2° (13 subjects)
Linear measurements in millimeters were taken (Figure 2) as described below for the UAFH, LAFH, total anterior facial height (TAFH), and the ratios of UAFH and LAFH to TAFH was calculated for all the three groups [14, 20]:
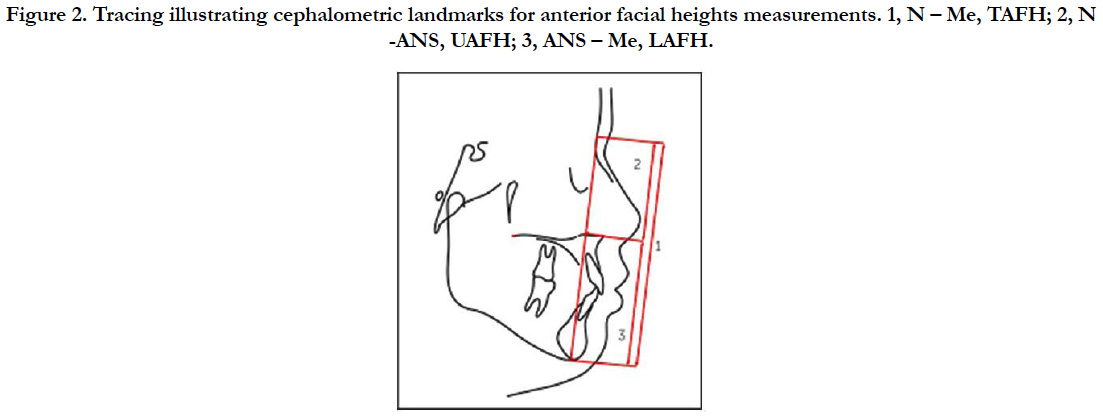
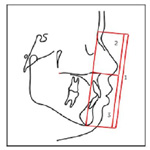
Figure 2. Tracing illustrating cephalometric landmarks for anterior facial heights measurements. 1, N – Me, TAFH; 2, N -ANS, UAFH; 3, ANS – Me, LAFH.
• UAFH (N- ANS) This was measured in millimeters as the distance between points N and the tip of the ANS.
• LAFH (ANS-Me) this was the measured distance from the ANS to the point Me.
• TAFH (N-Me) This was the measured distance in millimeters from the point N to the Me. It also corresponds to the sum of the UAFH and the LAFH.
Ratio of UAFH to TAFH (UAFH: TAFH) and LAFH to TAFH (LAFH: TAFH) were calculated in percentage from the measured values of the parameters.
Data were analysed in SPSS for Windows (version 21, SPSS Inc. Chicago). Baseline information on demographics was analysed using descriptive statistics. Mean values and standard deviations were calculated for linear measurements. The comparison of various facial height parameters between males and females was made using student t-test. Analysis of variance test was used to compare the studied parameters among the three skeletal pattern groups. To determine the correlation between facial height variables and the underlying skeletal pattern, Pearson’s correlation coefficients were applied. A p-value of <0.05 was taken as statistically significant.
To assess the measurement error, 10 lateral cephalograms were randomly selected and steps of tracing, landmarks identification and measurement were repeated by the investigator after three weeks of initial examination, thus generating a new set of measurements. Intra-class correlation coefficients were performed to assess the reliability for the measurements.
Results
Distribution of sample according to sex, ANB skeletal class, and age was presented in Table 2.
The values of correlation coefficients measuring intraobserver reliability were found to be greater than 0.94 for all the variables (Table 3).
Students t-test to test the gender difference in facial height parameters indifferent ANB skeletal classes, showed no statistically significant difference in all the skeletal classes (Table 4).
One-way between-groups ANOVA, to test the difference of mean facial height parameters among different ANB skeletal classes, showed no statistically significant difference (Figure 3).
Table 5 showed that none of the facial height variables correlate significantly with the skeletal pattern.
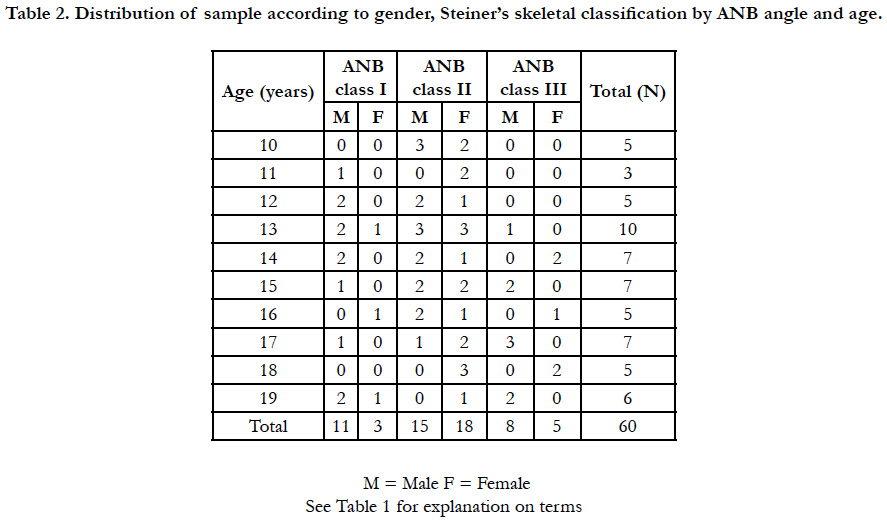
Table 2. Distribution of sample according to gender, Steiner’s skeletal classification by ANB angle and age.
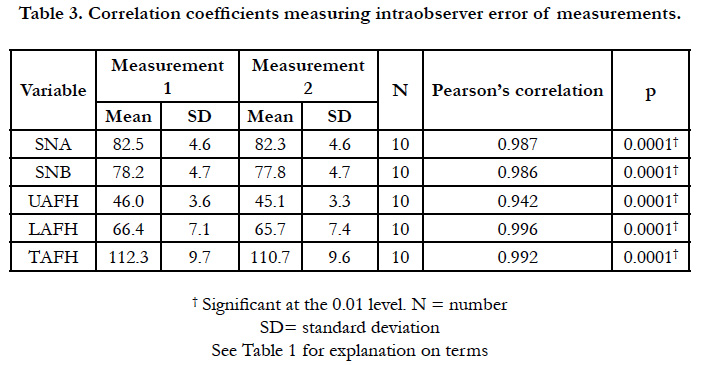
Table 3. Correlation coefficients measuring intraobserver error of measurements.
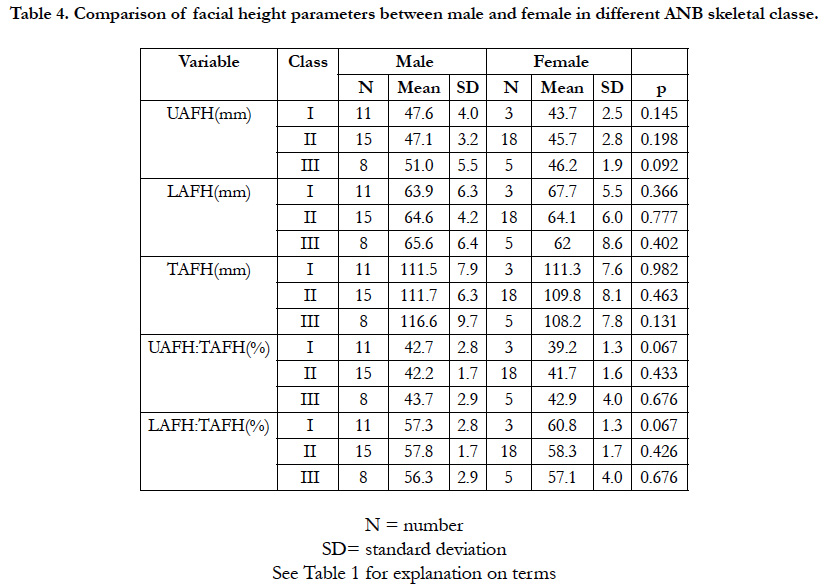
Table 4. Comparison of facial height parameters between male and female in different ANB skeletal classe.
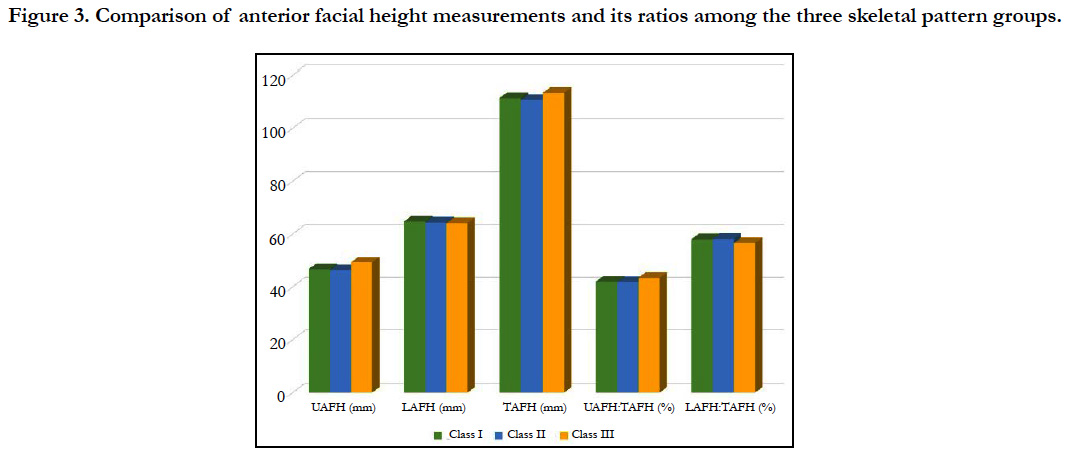
Figure 3. Comparison of anterior facial height measurements and its ratios among the three skeletal pattern groups.
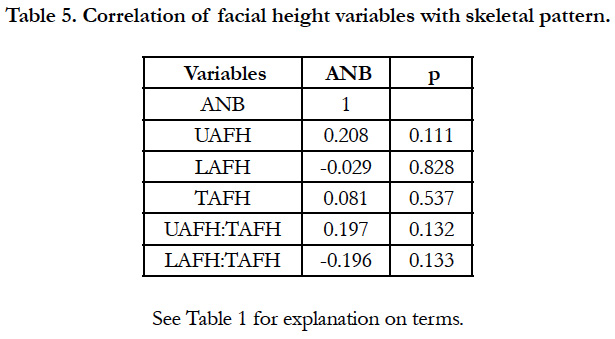
Table 5. Correlation of facial height variables with skeletal pattern.
Discussion
The present study found the mean values of the facial height parameters in male and female in each skeletal group did not show any significant difference (Table 4). This is in agreement with previous studies among different ethnic population in Nigeria [14, 21] and other populations [22]. However, sexual dimorphism was reported in LAFH and TAFH among young Japanese-Brazilian descendants [16]. Some populations also found males to have higher upper and lower anterior facial height as well as nose dimensions than females [17, 23, 24].
The mean values of the facial height parameters among the different skeletal groups did not show any significant difference (Figure 3). This differs from previous studies that reported variations in anterior facial height parameters among different skeletal pattern groups citing various reasons responsible. These include variation in anterior cranial base [25], characterization of skeletal pattern II by increased TAFH [26], a more acute cranial base angle in skeletal III group [27], cranial base bend and forward rotation of the mandible in Class III group [22].
An accurate assessment of a patient's facial skeletal pattern in vertical, sagittal and transverse direction is essential during orthodontic diagnosis and treatment planning. The vertical pattern of face defines the variability in orthodontic mechanics, as well as in the facial proportions [28, 29]. The stability of lower incisors after treatment was related to the vertical growth pattern [30]. The diagnosis of vertical facial discrepancy is not only important for an adequate diagnosis and an efficient treatment plan, it is of utmost significance for retaining the corrected malocclusion, as continuation of vertical growth in later phases of life may result in relapse.
Cephalometric standards from different ethnic and racial have been determined and compared, and the need for individualization for each specific group has been demonstrated [31, 32], in order to better understand the cephalometric characteristics of different groups during orthodontic diagnosis and planning. Thus, the present study provides the clinician with a more specific reference in the vertical direction of the face, particularly for young Nigerian descendants with different skeletal malocclusion.
Due to the ethnic differences observed in previous vertical facial heights studies among Nigerian population samples [14, 21, 33, 34], our findings may not be applied on Nigerian population in general. Further studies in this field are necessary, especially in selecting a reliable sample, defining the ethnic group, and considering the regional differences.
Conclusions
Based on the sample and methods employed in this study, values are presented to establish a cephalometric pattern of anterior facial heights and its ratios, for young Nigerian descendants with different sagittal skeletal jaw relationships. The anterior facial heights and its ratios showed no significant sex variation and revealed no significant difference among the skeletal groups.
References
- Sassouni V. A classification of skeletal facial types. Am J Orthod. 1969 Feb;55(2):109-23. PubMed PMID: 5249177.
- Wylie WL. The assessment of anteroposterior dysplasia. Angle Orthod. 1947 Jul;17(3):97-109.
- Björk A. Cranial base development: a follow-up x-ray study of the individual variation in growth occurring between the ages of 12 and 20 years and its relation to brain case and face development. Am J Orthod. 1955 Mar 1;41(3):198-225.
- Johnston DJ, Hunt O, Johnston CD, Burden DJ, Stevenson M, Hepper P. The influence of lower face vertical proportion on facial attractiveness. Eur J Orthod. 2005 Aug;27(4):349-54. PubMed PMID: 15961569.
- Casko JS, Shepherd WB. Dental and skeletal variation within the range of normal. Angle Orthod. 1984 Jan;54(1):5-17. PubMed PMID: 6584051.
- Fishman LS. Individualized evaluation of facial form. Am J Orthod Dentofacial Orthop. 1997 May;111(5):510-7. PubMed PMID: 9155810.
- Solow B. The dentoalveolar compensatory mechanism: background and clinical implications. Br J Orthod. 1980 Jul;7(3):145-61. PubMed PMID: 6934010.
- Ku SJ, Lee SJ, Chang YI. Dentoalveolar compensation according to skeletal patterns of normal occlusion. Korea J Orthod. 2002 Apr 1;32(2):91-105.
- Schudy FF. Vertical growth versus anteroposterior growth as related to function and treatment. Angle Orthod. 1964 Apr;34(2):75-93.
- Downs WB. Variations in facial relationships: their significance in treatment and prognosis. Am J Orthod. 1948 Oct;34(10):812-40. PubMed PMID: 18882558.
- Jensen E, Palling M. The gonial angle: A survey. Am J Orthod. 1954 Feb 1;40(2):120-33.
- Fields HW, Proffit WR, Nixon WL, Phillips C, Stanek ED. Facial pattern differences in long-faced children and adults. Am J Orthod. 1984 Mar;85(3):217-23. PubMed PMID: 6608274.
- Steiner CC. Cephalometrics in clinical practice. Angle Orthod. 1959 Jan;29(1):8-29.
- Folaranmi N, Isiekwe M. Anterior face height values in a Nigerian population. Ann Med Health Sci Res. 2013 Oct;3(4):583-7. doi: 10.4103/2141- 9248.122121. PubMed PMID: 24380013.
- Isiekwe MC, Sowemimo GO. Cephalometric findings in a normal Nigerian population sample and adult Nigerians with unrepaired clefts. Cleft Palate J. 1984 Oct;21(4):323-8. PubMed PMID: 6595089.
- Vieira FP, Pinzan A, Janson G, Fernandes TM, Sathler RC, Henriques RP. Facial height in Japanese-Brazilian descendants with normal occlusion. Dental Press J Orthod. 2014 Sep-Oct;19(5):54-66. doi: 10.1590/2176- 9451.19.5.054-066.oar. PubMed PMID: 25715717.
- Hatwal P, Atal DK, Das S. Correlation of Upper Facial and Lower Facial Height in Garhwali Population of Uttarakhand. J Indian Acad Forensic Med. 2015;37(3):281-2.
- Dandajena TC, Nanda RS. Bialveolar protrusion in a Zimbabwean sample. Am J Orthod Dentofacial Orthop. 2003 Feb 1;123(2):133-7.
- Sassouni V. A roentgenographic cephalometric analysis of cephalo-faciodental relationships. Am J Orthod. 1955 Oct 1;41(10):735-64.
- Wylie WL, Johnson EL. Rapid evaluation of facial dysplasia in the vertical plane. Angle Orthod. 1952 Jul;22(3):165-82.
- Utomi IL. Vertical facial height and proportions of face in Hausa-Fulani children in Northern Nigeria. Niger Postgrad Med J. 2004 Mar;11(1):32-6. PubMed PMID: 15254569.
- Obaidi HA. Variation of facial heights among the Class I, II and III dentoskeletal relationships (Cephalometric study). Al–Rafidain Dent J. 2006(4):98-105.
- Salama EI, Abuaffan AH. Cephalometric Hard and Soft Tissue Norms for Sudanese Adults. Orthod J Nepal. 2015;5(2):28-32.
- Omotoso DR, Oludiran OO, Sakpa CL. Nasofacial anthropometry of adult Bini tribe in Nigeria. Afr J Biomed Res. 2011;14(3):219-21.
- Kasai K, Moro T, Kanazawa E, Iwasawa T. Relationship between cranial base and maxillofacial morphology. Eur J Orthod. 1995 Oct;17(5):403-10. Pub- Med PMID: 8529753.
- Klocke A, Nanda RS, Kahl-Nieke B. Role of cranial base flexure in developing sagittal jaw discrepancies. Am J Orthod Dentofacial Orthop. 2002 Oct;122(4):386-91. PubMed PMID: 12411884.
- Mouakeh M. Cephalometric evaluation of craniofacial pattern of Syrian children with Class III malocclusion. Am J Orthod Dentofacial Orthop. 2001 Jun;119(6):640-9. PubMed PMID: 11395709.
- Opdebeeck H, Bell WH. The short face syndrome. Am J Orthod. 1978 May;73(5):499-511. PubMed PMID: 277066.
- Schendel SA, Eisenfeld J, Bell WH, Epker BN, Mishelevich DJ. The long face syndrome: vertical maxillary excess. Am J Orthod. 1976 Oct;70(4):398- 408. PubMed PMID: 1067758.
- Tweed CH. The diagnostic facial triangle in the control of treatment objectives. Am J Orthod. 1969 Jun;55(6):651-7. PubMed PMID: 5253959.
- de Freitas LM, Pinzan A, Janson G, Freitas KM, de Freitas MR, Henriques JF. Facial height comparison in young white and black Brazilian subjects with normal occlusion. Am J Orthod Dentofacial Orthop. 2007 Jun;131(6):706. e1-6. PubMed PMID: 17561045.
- Miyajima K, Mcnamara Jr JA, Kimura T, Murata S, Iizuka T. Craniofacial structure of Japanese and European-American adults with normal occlusions and well-balanced faces. Am J Orthod Dentofacial Orthop. 1996 Oct;110(4):431-8. PubMed PMID: 8876496.
- Akinlolu AA, Atoyebi M, Akinola OB, Fatunke I, Jimoh R, Ajao MS. Sex and Tribal differences in Facial measurements of Nigerians of Yoruba, Hausa and Igbo origin. Res J Forensic Sci. 2016;4(1):5-11.
- Gabriels O, Eberechi UD, Josiah SH, Michael AA, Favour NJ. A study on some oro-facial variables of adults of bonny ethnic group in Nigeria. Int J Curr Microbiol App Sci. 2014;3(7):926-37.





