Cloverleaf Skull Syndrome (Kleeblattschädel Deformity): Findings on Cone Beam Computed Tomography
Maryanchik I1*, Nair MK2
1 Former Oral and Maxillofacial Radiology Resident, Division of Oral and Maxillofacial Radiology, Colleges of Dentistry and Medicine, University of
Florida, Gainesville, Florida, USA.
2 Professor and Director, Division of Oral and Maxillofacial Radiology, Diagnostic Sciences, Texas A&M University College of Dentistry, Dallas,
Texas, USA.
*Corresponding Author
Igor Maryanchik, DDS, MS,
Former Oral and Maxillofacial Radiology Resident, Division of Oral and Maxillofacial Radiology,
Colleges of Dentistry and Medicine, University of Florida, Gainesville, Florida, USA.
Tel: 703-599-6416
E-mail: docigorm@gmail.com
Received: May 10, 2018; Accepted: May 25, 2018; Published: May 28, 2018
Citation:Maryanchik I, Nair MK. Cloverleaf Skull Syndrome (Kleeblattschädel Deformity): Findings on Cone Beam Computed Tomography. Int J Dentistry Oral Sci. 2018;5(5):637-640. doi: dx.doi.org/10.19070/2377-8075-18000125
Copyright: Maryanchik I©2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Cloverleaf skull syndrome or Kleeblattschädel Abnormality involves an abnormal configuration of the calvarium, a rare presentation of craniosynostosis consisting of premature ossification of cranial sutures. Craniofacial dysostosis is encountered in different congenital malformations as well. Clinically and radiographically enlarged and trilobed cranium resulting from cranial and basal synostosis associated with hydrocephalus is the hallmark feature. A slew of other clinical and radiographic features is noted including upper airway compromise.
Clinical and Radiographic Findings: The present report is aimed at describing radiographic features of this syndrome carried by a 12 year-old female, as visualized on maxillofacial cone-beam computed tomography (CBCT) study. In addition to the patient’s clinical presentation of dysmorphic facial features, multiple cranial deformities status post craniotomies are reported.
Conclusion: The relevance of imaging diagnosis and characterization of this syndrome must be emphasized in order to allow for proper planning and implementation of treatment as early as possible. The need for repeated surgical corrective maxillofacial procedures in a pediatric patient is to be noted as well.
Statement of Clinical Relevance: Cloverleaf skull syndrome, the most severe form of craniosynostosis often associated with other abnormalities in the calvaria as well as in the skull base and face, is requiring the most complex multidisciplinary approach. A thorough radiographical evaluation is required to characterize the craniofacial bone deformities and guide the corrective treatment planning surgical procedures in a timely fashion in order to facilitate improvement in the prognosis of the affected children.
2.Introduction
3.Purpose
4.Case Report
5.Findings
6.Discussion
7.Conclusion
8.Acknowledgement
9.References
Keywords
Cloverleaf Skull Syndrome; Kleeblattschädel Abnormality; Craniofacial Dysostosis; Cone Beam Computed Tomography.
Introduction
Cloverleaf skull syndrome or Kleeblattschädel abnormality (Holtermüllerand Wiedermann, 1960 [1]) is an abnormal configuration of the calvaria, a rare presentation of craniosynostosis, consisting of premature ossification of cranial sutures.
Craniofacial dysostosis is encountered in different congenital malformations such as Kleeblattschädel deformity, Crouzon's disease, as well as Apert's, Chotzen's, Pfeiffer's, and Carpenter's syndromes [2].
The main feature of the cloverleaf skull syndrome/deformity is a clinically and radiologically enlarged and trilobed cranium resulting from cranial and basal synostosis associated with hydrocephalus [3]. Its additional clinical and radiographic features are comprised of a very grotesque facial appearance, maxillary and orbital hypoplasia with exorbitism and retrusion of the midface, flattened nose, downwardly displaced ears, skeletal abnormalities, and upper airway obstruction [2, 4, 5].
Systemically, when it is associated with chondrodystrophy, rigidity of elbow joints, which results from maldevelopment of the limb bones, particularly the humerus, radius and ulna, may be often observed (Angle et al., 1967 [6]). Extreme forms of this condition result in poor neurological outcome and high mortality in infancy [7].
Purpose
The present report is aimed at describing radiographic representations of this syndrome carried by a 12-year-old female, as visualized on maxillofacial cone beam computed tomography (CBCT) study.
Case Report
This patient was born prematurely, delivered at 32 weeks by Csection. At 24 weeks, cloverleaf skull with pan suture synostosis was diagnosed by ultrasound. She spent two weeks in the NICU and had an extensive craniectomy performed at three weeks of age. She additionally had orbital advancement at 18 months. This was complicated by infected hydroxy implant, which had to be removed. Being 3.5 years old, she underwent mid face advancement and repeated orbital advancement.
She had numerous surgical procedures including ventriculoperitoneal shunt placement, tracheostomy, gastrostomy, tonsillectomy and adenoidectomy, tracheal surgery, and LeFort I osteotomies. The patient is now tracheostomy and gastrostomy-tube dependent. Her family history is unremarkable.
Findings
Clinical presentation includes: dysmorphic facial features, ocular hypertelorism, downward slanting palpebral fissures, low nasal bridge, and downwardly displaced ears.
Numerous radiographic findings, associated with this syndrome, include: multiple cranial deformities status post craniotomies for hydrocephalus (Figure 1), severe skeletal and occlusal abnormalities (Figure 1), deficiency of the mid-maxilla with rotation of the maxillary alveolus superiorly (Figure 2), prominent apertognathia (Figure 2), hypoplastic maxillary, ethmoid and sphenoid sinuses (Figure 3), significant nasal congestion extending into the ethmoid sinuses (Figure 4), deformed and diminutive temporomandibular joints (Figure5), and maxillary left cleft palate that extends into the floor of the nasal fossa (Figure 6).
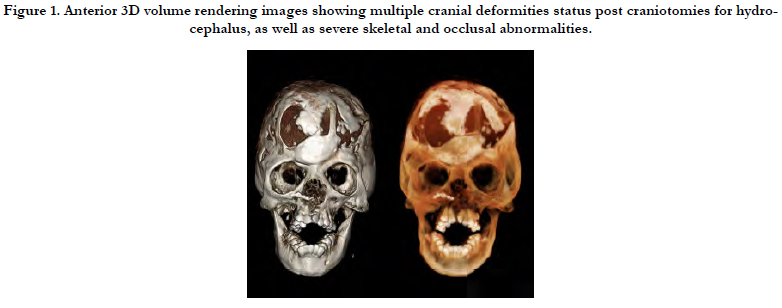
Figure 1. Anterior 3D volume rendering images showing multiple cranial deformities status post craniotomies for hydrocephalus, as well as severe skeletal and occlusal abnormalities.
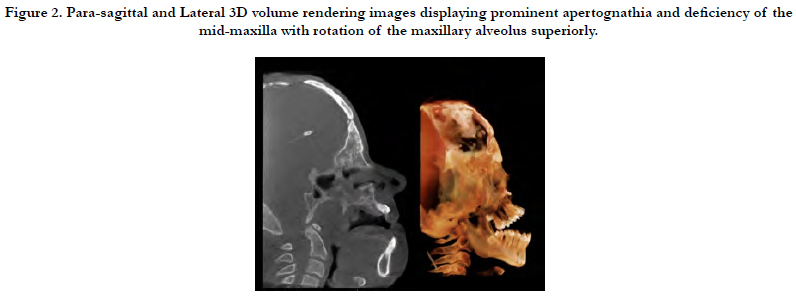
Figure 2. Para-sagittal and Lateral 3D volume rendering images displaying prominent apertognathia and deficiency of the mid-maxilla with rotation of the maxillary alveolus superiorly.
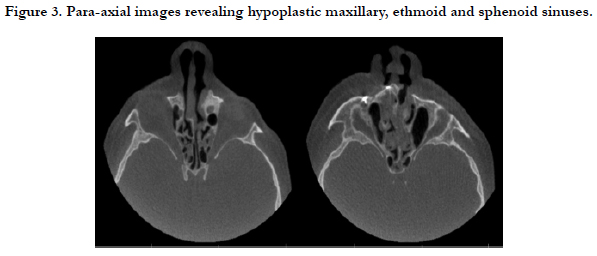
Figure 3. Para-axial images revealing hypoplastic maxillary, ethmoid and sphenoid sinuses.
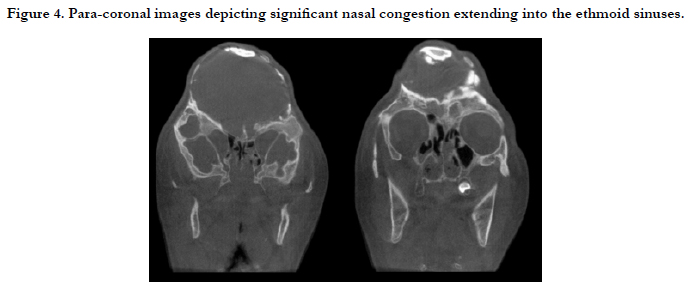
Figure 4. Para-coronal images depicting significant nasal congestion extending into the ethmoid sinuses.
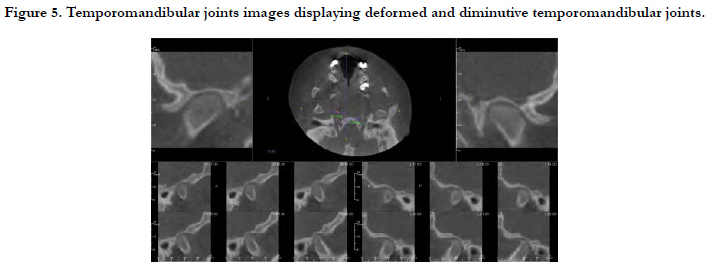

Figure 5. Temporomandibular joints images displaying deformed and diminutive temporomandibular joints.
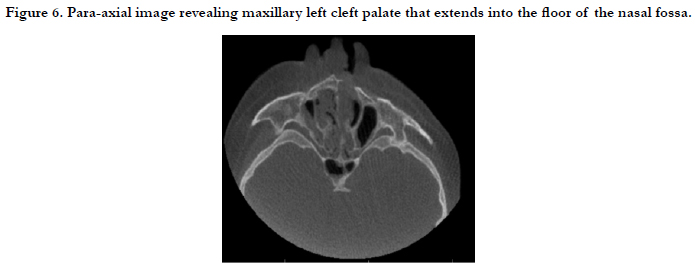
Figure 6. Para-axial image revealing maxillary left cleft palate that extends into the floor of the nasal fossa.
Signs of closure of sagittal, coronal and lambdoid sutures were also observed. The posterior fossa was also narrow, especially the foramen magnum, which did not spread on both sides and was shaped into an oval with both ends pointed.
Discussion
Cloverleaf skull syndrome is the most severe form of craniosynostosis and is often associated with other abnormalities. Because of the anomalies both in the calvaria and in the skull base and face, this is one of the craniosynostosis currently requiring the most complex multidisciplinary approach [8, 9].
The formation of the trilobed cranial shape occurs as a result from a severe alteration in the development of the cranium: it is strongly retarded in the anteroposterior direction due to premature ossification of some cranial sutures, most commonly the coronal and lambdoid sutures. Also, the accompanying hydrocephalus forces brain tissue to protrude through the openings of the sagittal and squamal sutures, and grow bilateral and upward. This is leading to a marked bulging of the head in the region of the anterior fontanel and laterally in the temporal regions, with the typical appearance of a “cloverleaf ” [3].
Premature synostosis/closure of cranial and facial sutures leads to characteristic disfigurement of the skull with orbital and maxillary hypoplasia. Cranial and facial growth then consecutively leads toward patent suture lines. Often, cranial synostoses extend downward to the cranial base affecting facial growth. Maxillary and orbital hypoplasia with exorbitism and retrusion of the midface are then present [4, 5].
All the clinical manifestations and radiographic findings as noted in our patient were consistent with features described in patients associated with cloverleaf skull syndrome in the literature [2-4, 6-8].
Conclusion
The relevance of the imaging diagnosis and characterization of this syndrome is highlighted in order to allow for planning and execution of treatment as early as possible. The diagnosis of such a syndrome can be made in the prenatal period by means of ultrasonography, which detects the altered cranial morphology and hydrocephalus.
After birth, as an abnormal configuration of the calvaria is detected, a radiographical evaluation is required to characterize the deformity and guide the corrective surgical procedure. There is a significant improvement in the prognosis of affected children in cases where the diagnosis and the surgical intervention occur as early as possible [8, 9]. Computed tomography with three-dimensional reconstruction contributes to the assessment of craniofacial bone deformities and associated intracranial alterations, demonstrating to be a useful tool to define the prognosis and for the surgical planning.
Despite the unfavorable outcome of many cases, advances in surgical, anesthetic and intensive care techniques have transformed a condition previously considered untreatable into a potentially treatable condition, with acceptable neurological and aesthetic results [7].
Abstract/Poster presentation was submitted to the American Society of Head and Neck Radiology (ASHNR) annual meeting 2015 and was accepted as an electronic exhibit Power Point presentation.
Acknowledgement
Oral and Maxillofacial Surgery, Orthodontics, College of Dentistry, University of Florida.
References
- Holtermüller K, Wiedermann HR. The clover-leaf skull syndrome. Med Monatsschr. 1960 Jul;14:439-46. PubMed PMID: 13715562.
- Hennekam RC, Krantz ID, Allanson JE. Gorlin’s syndromes of the head and neck. 5thed. New York, NY: Oxford University Press; 2010. p. 732-748.
- Comings DE. The Kleeblattschdel syndrome--agrotesque form of hydrocephalus. J Pediatr. 1965 Jul;67:126-9. PubMed PMID: 14302138.
- Wollin DG, Binnington VI, Partington MW. Cloverleaf skull. J Can Assoc Radiol. 1968 Sep;19(3):148-54. PubMed PMID: 4972434.
- Trad CS, Rosique RG. Primary craniosynostoses: iconographic essay. Radiol Bras. 2005; 38 (5): 377-80.
- Angle CR, McIntire MS, Moore RC. Cloverleaf skull: Kleeblattschädeldeformity syndrome. Am J Dis Child. 1967 Aug;114(2):198-202. PubMed PMID: 4951548.
- Manjila S, Chim H, Eisele S, Chowdhry SA, Gosain AK, Cohen AR. History of the Kleeblattschädel deformity: origin of concepts and evolution of management in the past 50 years. Neurosurg Focus. 2010 Dec;29(6):E7. PubMed PMID: 21121721.
- Iannaccone G, Gerlini G. The so-calle "Cloverleaf Skull Syndrome". A report of three cases with a discussion of its relationships with thanatophoric dwarfism and the craniostenoses. Pediatr Radiol. 1974;2(3):175-84. PubMed PMID: 4424221.
- Muller PJ, Hoffman HJ. Cloverleaf skull syndrome: Case report. J Neurosurg. 1975 Jul;43(1):86-91. PubMed PMID: 1141987.





