Cleidocranial Dysplasia: Keys to Diagnosis
Marwa Trifi W1*, Triki H2, Mansour L2, Trabelsi M2
1 Resident fellow in removable partial dentures, faculty of dental medicine, University of Monastir, Tunisia.
2 Professor in removable partial dentures, faculty of dental medicine, University of Monastir, Tunisia.
*Corresponding Author
Wijdene Marwa Trifi,
DDS, Resident Fellow in Removable Partial Dentures, Laboratory of Dento-Facial,
Clinical and Biological Approach (ABCDF), LR12ES10, Faculty of Dental Medicine,
University of Monastir, Avicenna Avenue, 5000, Monastir, Tunisia.
Tel: +21620562733
Fax: +21620562733
E-mail: trifiwijdene@yahoo.fr
Received: October 17, 2017; Accepted: January 07, 2018; Published: January 23, 2018
Citation:Marwa Trifi W, Triki H, Mansour L, Trabelsi M. Cleidocranial Dysplasia: Keys to Diagnosis. Int J Dentistry Oral Sci. 2018;5(1):585-588. doi: dx.doi.org/10.19070/2377-8075-18000114
Copyright: Marwa Trifi W©2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Cleido-cranial dysplasia (CCD) is a rare congenital disorder with an autosomal dominant inheritance. This disease is caused by mutations in the C10fa1, also called RUNX2. This gene mutation affects bones undergoing intramembranous ossification inducing hypoplasia/aplasia of clavicles, patent fontanels and short stature. Common features are bulky forehead, hypertelorism, midfacial hypoplasia and supernumerary teeth presence.
Case Presentation: An 18-year-old male was referred to the removable partial denture department with a chief complaint of an ill-fitting upper and lower removable partial dentures. Dental anomalies included retention of temporary dentition, eruption delay of permanent teeth and supernumerary teeth genesis. Hereby, we report an accurate examination of a CCD case with an emphasis on the clinical and radiological features.
Conclusion: Bony malformations, aplasia or hypoplasia of one or both clavicles and the presence of supernumerary teeth are the main features of cleidocranial dysplasia. Early diagnosis is essential for initiating the appropriate management.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.Acknowledgments
7.References
Keywords
Cleidocranial Dyplasia; Clavicles Hypoplasia; Patent Fontanels; Teeth Impaction; Supernumerary Teeth; Delayed Eruption.
Background
Cleidocranial dysplasia (CCD, OMIM 119600), also known as Marie and Santon disease or cleidocranial dysostosis [1], is a very rare congenital disorder with an incidence of 1 per million [2]. CCD is usually inherited and transmitted as dominant in both sex [3]. This condition is usually caused by a mutation of the Core Binding Factor- α1 gene (CBFA1) located at chromosome 6p21 [4], although 40% of the cases appear spontaneously with no apparent genetic cause [5]. The CBFA1 gene controls the differentiation of precursor cells into osteoblasts, which is essential for osteoblast and dental cell differentiation, membranous as well as endochondral ossification and tooth formation [4, 6]. Consequently, the main three symptoms of CCD are the pathognomonic deformity of the skull (persistently open skull sutures resulting in wormien bones) [7], aplasia or hypoplasia of one or both clavicles (resulting in hypermobility of the shoulders) and prolonged retention of deciduous, permanent and supernumerary teeth [8]. If this triad is not complete, it is necessary to consider the possibility of other entities in a differential diagnosis such as congenital pseudoarthrosis (characterized by the absence of one of the clavicles usually the right one) and pyknodysostosis (characterized by malformed bones, osteosclerosis, delayed suture closures, dysplasia of distal phalanges, anodontias, and delayed eruption of permanent teeth) [5]. Hypodontia might be a common finding in several specific syndromes, for instance, Gardner syndrome (OMIM 175100), Hallermann Streiff syndrome (OMIM 234100) and orofacial digital syndrome type 1 (OMIM 311200) [9].
This article advances an accurate examination of a CCD adult with an emphasis on the clinical and radiological features.
Case Report
An 18-year-old male was referred to the removable partial denture department with the chief complaint of an ill-fitting upper and lower removable partial dentures (RPD). The patient was born via normal spontaneous vaginal delivery without asphyxia or rescue history. His parents were healthy and his mother reported no exposure to drugs, medication or alcohol during pregnancy. There were no other family members with bony abnormalities, delayed teeth eruption or short stature.
On physical examination, the patient had a thin built, a short stature and frontal bossing. The most striking feature was the slight approximation of both shoulders near midline suggestive of shoulders hypermobility. Hypertelorism, mid facial hypoplasia resulting in a concave facial profile, depressed nasal bridge and a wide nose base were also noticed [Figure 1].
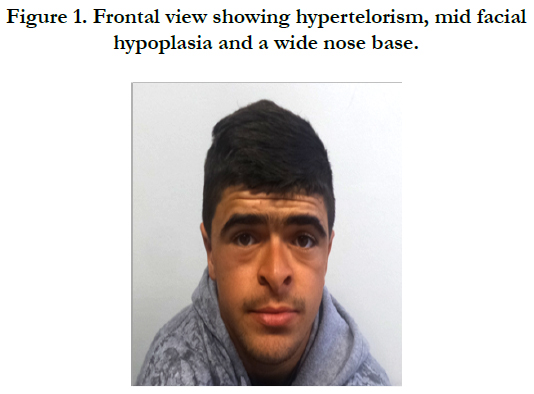

Figure 1. Frontal view showing hypertelorism, mid facial hypoplasia and a wide nose base.
The examination of the oral cavity revealed a partial edentulism on both arches, a dental class III malocclusion, anterior and posterior crossbite, multiple decays and several missing permanent teeth particularly in anterior sectors [Figure 2].
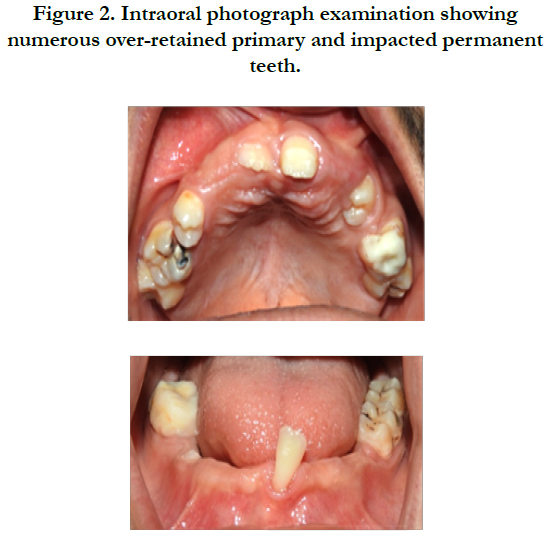

Figure 2. Intraoral photograph examination showing numerous over-retained primary and impacted permanent teeth.
The examination of 2-year-old orthopantomogram (OPG) and maxillary and mandibular cone computed tomography images revealed multiple impacted permanent teeth, and multiple supernumerary teeth. Maxillary canines were highly impacted which did not repress neither the maxillary sinuses nor the nasal fossae [Figure 3].
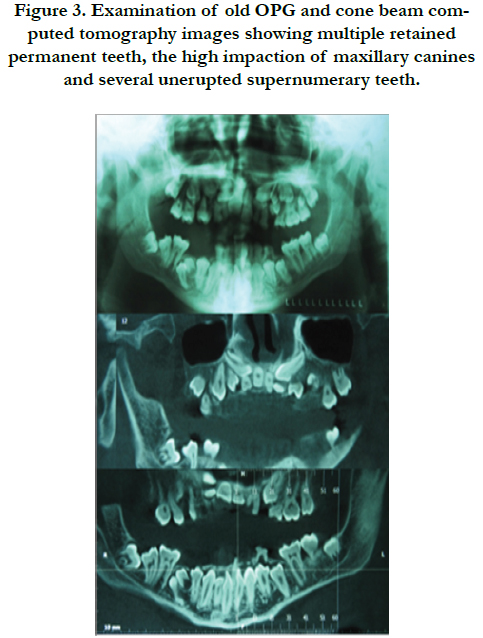

Figure 3. Examination of old OPG and cone beam computed tomography images showing multiple retained permanent teeth, the high impaction of maxillary canines and several unerupted supernumerary teeth.
The classical signs of cleidocranial dysplasia were immediately recognized. A recent OPG was required to evaluate the patient’s overall dentition after several deciduous and supernumerary teeth removal and after wearing RPD for 2 years. A mild occlusal migration of both upper and lower teeth resulting from effect of occlusal forces was noticed.
OPG examination also revealed the existence of residual supernumerary teeth and confirmed the absence of any complication due to the high impaction of maxillary canines [Figure 4].
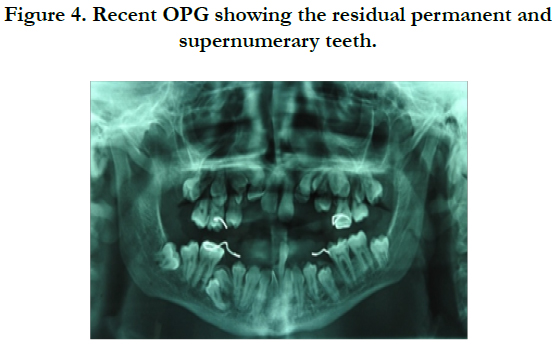
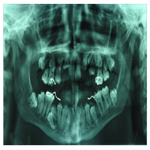
Figure 4. Recent OPG showing the residual permanent and supernumerary teeth.
The lateral cephalometric radiograph observation revealed mandibular prognathism, mandibular ascending ramus borders parallelism. Maxillary sinuses and nasal bones underdevelopment, frontal bossing, cranial sutures unossofication resulting in numerous wormian bones in parietal-occipital region, absence of aeration in the mastoid sclerotic cells and a narrow external acoustic meatus were revealed upon examination [Figure 5A].
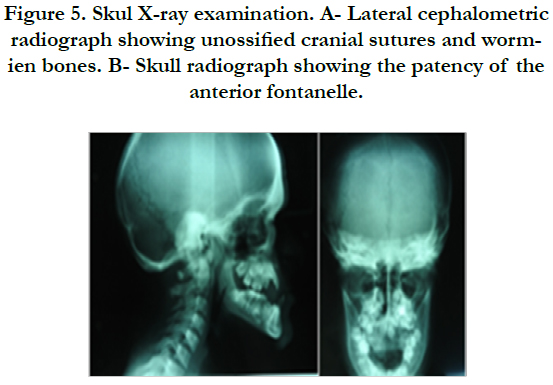
Figure 5. Skul X-ray examination. A- Lateral cephalometric radiograph showing unossified cranial sutures and wormien bones. B- Skull radiograph showing the patency of the anterior fontanelle.
Skull radiograph showed the patency of the anterior fontanelle resulting in frontal bossing and poorly formed paranasal sinuses and zygomatic complex [Figure 5B].
Chest radiograph revealed a narrow thorax with tapered width superiorly, mild hypoplastic clavicles over bilateral region and absence of connection with sternoclavicular and acromioclavicular joints. Hand wrist X-ray revealed the definite calcification of sesamoid bone [Figure 6].
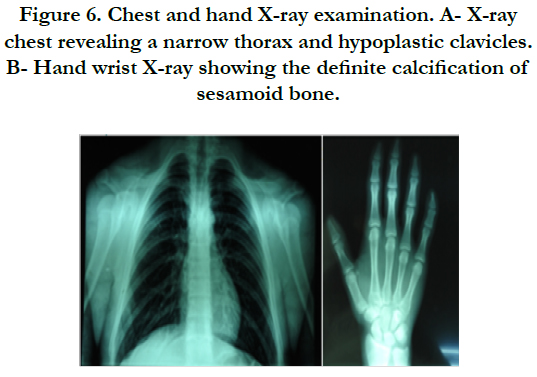
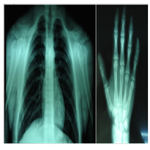
Figure 6. Chest and hand X-ray examination. A- X-ray chest revealing a narrow thorax and hypoplastic clavicles. B- Hand wrist X-ray showing the definite calcification of sesamoid bone.
Based on clinical and radiographic findings, the diagnosis of CCD was confirmed. A holistic approach involved surgery, endodontics and fixed and removable partial dentures.
Discussion
Cleidocranial dysplasia is an autosomal dominant disorder mapped to RUNX2 gene mutation. Researchers have shown that this gene is involved in the osteoblastic and chondrocyte differentiation during endochondral ossification [10].
Hence, Runx2 mutation is incriminated in the early developmental disorder of mesenchyme or connective tissue, causing retarded ossification of bone precursors, especially at junctions, which can lead to defective ossification or even failure of ossification of portions of skeletal structures [11]. Skeletal anomalies may include a wide pubic symphisis, dysplastic scapulae, coxa vara, and several vertebral anomalies [9]. The affection of the syndesmosis between cranial bones affects the skull base. The dysplasia and reduction in growth of the skull base results in the increase of the skull width which leads to brachycephaly and hypertelorism [11]. The defective ossification of medial and lateral centers of the clavicles which are separated by a fibro-cellular structure [12] permits undue mobility to the shoulders. This ability to approach the shoulders anteriorly is a major feature of cleidocranial dysplasia.
These clinical manifestations are usually innocuous. The general health and the intellect are unimpaired [13] but affected persons may suffer of recurrent infections of the upper respiratory tract and hear loss due to the underdevelopment of the sinuses and chronic otitis media [14]. The cosmetic appearance of the dentition is often unsightly and mastication is compromised by thepresence of supernumerary teeth and the impaction of permanent dentition.
The causes of unerupted teeth were attributed to the disturbance of bone resorption, the early loss of the gubernacular cord or canal, the absence of cellular cementum the increase of acellular cementum on affected teeth’s roots [15], lack of union between the dental follicle and the mucosa due to interposed fibrous tissue acting as a barrier to eruption, an an increased percentage of the gap type of cementum enamel junctions and decreased alkaline phosphatase levels [16].
Excessive number of supernumerary teeth, usually mimicking a premolar [3], is another striking feature in the diagnosis of CCD. This increase in the odontogenesis [17] particularly in mandibular premolar and maxillary anterior regions [1] may affect the normal eruption of permanent dentition and induce the resorption of their roots [18].
Conclusion
The diagnosis of CCD may be difficult if the common features are not prominent. The earlier this diagnosis is established, the more appropriate management will be carried out to manage these clinical manifestations.
Acknowledgments
The authors thank the radiology department of Monastir’s faculty of dental medicine for their cooperation and assistance.
References
- Kalliala E, Taskinen PJ. Cleidocranial dysostosis: report of six typical cases and one atypical case. Oral Surg Oral Med Oral Pathol.1962 July;15(7):808-22. PubMed PMID:14453327.
- Shen Z, Zou CC, Yang RW, Zhao ZY. Cleidocranial dysplasia: report of 3 cases and literature review.Clin Pediatr (Phila). 2009 Mar;48(2):194-8. PubMed PMID: 18832541.
- Garg RK, Agrawal P. Clinical spectrum of cleidocranial dysplasia: a case report. Cases J. 2008 Dec 8;1(1):377. PubMed PMID: 19063717. PubMed Central PMCID: PMC2614945.
- Mundlos S. Cleidocranial dysplasia: clinical and molecular genetics. J Med Genet. 1999 Mar;36(3):177-82. PubMed PMID: 10204840.
- Tanaka JL, Ono E, Filho EM, Castilho JC, Moraes LC, Moraes ME. Cleidocranial dysplasia: importance of radiographic images in diagnosis of the condition. J Oral Sci. 2006 Sep;48(3):161-6. PubMed PMID: 17023750.
- Chen S, Santos L, Wu Y, Vuong R, Gay I, Schulze J, et al. Altered gene expression in human cleidocranial dysplasia dental pulp cells. Arch Oral Biol. 2005 Feb;50(2):227-36. PubMed PMID: 15721154.
- Nagarathna C, Shakuntala BS, Mathew S, Krishnamurthy NH, Yumkham R. Cleidocranial dysplasia presenting with retained deciduous teeth in a 15-year-old girl: a case report. J Med Case Rep. 2012 Jan 19;6:25. PubMed PMID: 22260259. PubMed Central PMCID: PMC3292823.
- Sekerci AE, Balta B, Sisman Y, Dundar M, Tokmak TT, Mundlos S. Cleidocranial dysplasia with a rare mutation: Study of a family with review of literature. Open Journal of Stomatology. 2013 Jan ;3(08):402.
- Roberts T, Stephen L, Beighton P. Cleidocranial dysplasia: a review of the dental, historical, and practical implications with an overview of the South African experience. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013 Jan;115(1):46-55. PubMed PMID: 23102800.
- Li Y, Pan W, Xu W, He N, Chen X, Liu H, et al. RUNX2 mutations in Chinese patients with cleidocranial dysplasia. Mutagenesis. 2009 Jun;24(5):425- 31.
- Golan I, Baumert U, Hrala B, Müßig D. Dentomaxillofacial variability of cleidocranial dysplasia: clinicoradiological presentation and systematic review. Dentomaxillofac Radiol. 2003 Nov;32(6):347-54. PubMed PMID: 15070835.
- Hemalatha R, Balasubramaniam M. Cleidocranial dysplasia: A case report. J Indian Soc Pedod Prev Dent. 2008 Jan ;26(1):40.
- Cooper SC, Flaitz CM, Johnston DA, Lee B, Hecht JT. A natural history of cleidocranial dysplasia. Am J Med Genet. 2001 Nov 15;104(1):1-6. PubMed PMID: 11746020.
- Segal N, Puterman M. Cleidocranial dysplasia-review with an emphasis on otological and audiological manifestations. Int J Pediatr Otorhinolaryngol. 2007 Apr;71(4):523-6. PubMed PMID: 17239447.
- Counts AL, Rohrer MD, Prasad H, Bolen P. An assessment of root cementum in cleidocranial dysplasia. Angle Orthod. 2001 Aug;71(4):293-8. Pub- Med PMID: 11510638.
- Manjunath K, Kavitha B, Saraswathi T, Sivapathasundharam B, Manikandhan R. Cementum analysis in cleidocranial dysostosis. Indian J Dent Res. 2008 Jul-Sep;19(3):253-6.
- Dard M. Histology of alveolar bone and primary tooth roots in a case of cleidocranial dysplasia. Bull Group Int Rech Sci Stomatol Odontol. 1993 Jul-Sep;36(3-4):101-7. PubMed PMID: 8219688.
- Golan I, Baumert U, Hrala B, Müßig D. Early craniofacial signs of cleidocranial dysplasia. Int J Paediatr Dent. 2004 Jan;14(1):49-53. PubMed PMID: 14706028.





