Clinical Management of Maxillary Incisor with Complicated Crown-Root Fracture: A Case Report
Habbad AS1*, Alhazmi SA2, Sadayo TZ2
1 General Dentist, Alnoor Specialist Hospital, Ministry of Health, Makkah, Saudi Arabia.
2 General Dentist, Makkah, Saudi Arabia.
*Corresponding Author
Abdullah Saleh Habbad,
General Dentist, Alnoor Specialist Hospital,
Ministry of Health, Makkah, 23462, Saudi Arabia.
Tel: 00966545457645
Fax: 545457645
E-mail: dent.ash88@gmail.com
Received: November 23, 2017; Accepted: January 17, 2018; Published: January 22, 2018
Citation:Habbad AS, Alhazmi SA, Sadayo TZ. Clinical Management of Maxillary Incisor with Complicated Crown-Root Fracture: A Case Report. Int J Dentistry Oral Sci.
2018;5(1):581-584. doi: dx.doi.org/10.19070/2377-8075-18000113
Copyright: Habbad AS©2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The sequelae of a fractured anterior tooth may have a huge impact on aesthetics and function. A case of a 27-year-old male patient presented clinically with extensively fractured upper right central incisor that extended subgingivally on the palatal side. Non-responding lower right central incisor to thermal tests was observed. Periapical radiographs showed periapical radiolucencies around the roots of the aforementioned teeth. The fractured tooth was managed by surgical crown lengthening, endodontic and prosthetic procedures. A conventional root canal treatment was conducted on the lower right central incisor. The reported case highlights the importance of thorough examination, proper diagnosis and the multidisciplinary approach in managing dental trauma cases.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
Crown-Root Fracture; Multidisciplinary Approach; Subgingival.
Introduction
Traumatic dental injuries are prevalent in primary as well as in permanent dentition with the maxillary anterior teeth being the most commonly affected area [1]. Crown-root fractures account for 5% of all dental injuries affecting the permanent teeth. These injuries involve enamel, dentin and cementum, with or without pulpal involvement [2].
Several factors may affect the management of a fractured tooth such as biologic width violation, endodontic involvement, remaining tooth structure, presence of fractured segment and its condition for use, occlusion, aesthetics, finance, prognosis and patient cooperation [3]. Management of complicated crown-root fracture, especially when the fracture locates in close proximity to or below the crestal bone level, is not an ordinary case for a general dental practitioner. A subgingival fracture further complicates the execution of the treatment due to difficulty in maintaining a proper dry field during endodontic procedures and possible violation of the biologic width while placing the restorative margin [4]. Damage to the periodontium in the form of gingival inflammation, bone resorption and recession may persist as a result of failure to reconstruct the biologic width [5]. To maintain a healthy periodontal-restorative interrelationship, exposure of tooth structure supragingivally becomes necessary which can be achieved bysurgical crown lengthening, orthodontic forced eruption or a combination of both [5].
Complicated crown-root fractures usually require a multidisciplinary approach to deliver predictable esthetics and proper function. The aim of this case report was to present a fractured maxillary right central incisor with biologic width invasion that was successfully managed by surgical crown lengthening, endodontic treatment, cast post-core system and a crown.
Case Report
A healthy 27-year-old male patient attended a private dental clinic in Makkah city, Saudi Arabia, with a chief complaint of broken upper anterior tooth. The patient reported falling on his face accidentally during work about a year ago. Extraoral examination exhibited no abnormalities. Intraoral examination revealed that the upper right central incisor had an obliquely fractured crown taking up to two-thirds of the clinical crown. The remaining crown was discolored, carious, pulpally involved and presented with a mobile palatal fragment that was still attached to the palatal soft tissue (Figure 1A, B, C). The tooth showed no sign of mobility; except for the palatal fragment, no sensitivity to percussion or palpation but did not respond to thermal tests. Caries was removed and the palatal fragment was detached to determine the restorability of the tooth and the extent of the fracture (Figure 1D). Upon clinical evaluation, the fracture line extended subgingivally on the palatal side. The remaining upper and lower anterior teeth were also clinically examined. The lower right central incisor showed a total lack of response to thermal tests indicating a possible pulp necrosis.Intraoral periapical radiographs of maxillary right central incisor and lower right central incisor demonstrated apical radiolucency around their root apices (Figure 1 E, F). No other unusual radiographic findings were noted in the remaining anterior teeth. A multidisciplinary approach was decided for the treatment of the fractured tooth which included surgical crown lengthening for exposure of the subgingival fracture followed by endodontic therapy and prosthetic rehabilitation with cast post-core and complete coverage crown. Root canal therapy was the proposed treatment for the lower right central incisor.
Under local anesthesia, a full thickness palatal flap was elevated in relation to the fractured tooth (Figure 2A). Bone was removed palatally allowing for at least 3mm distance between the bony crest and the initially prepared finish line and a scalloped bony contour was maintained during removal. The surgical site was irrigated with normal saline and sutured with interrupted silk sutures. A provisional crown was temporarily cemented to the fractured tooth and post-surgical instructions were given to the patient. Systemic antibiotic, analgesic and 0.2% chlorohexidine mouthwash were prescribed. Sutures were removed one week after the surgery and adequate exposure of tooth structure was initially achieved (Figure 2B). In the next visit, root canal therapy was initiated in the maxillary right central incisor and the mandibular right central incisor. Access cavity preparation and working length determination were done under rubber dam isolation. Root canals were thoroughly debrided and stepped back. Irrigation with 5.25% sodium hypochlorite solution was used throughout the procedure. Calcium hydroxide paste (Apexcal, IvoclarVivadent, Liechtenstein) was applied in the root canals as an intra canal medicament. Obturation using lateral condensation technique with gutta-percha points (Sure-Endo, Sure Dent Corp., Seoul, Korea) and AH Plus sealer (DentsplyDeTrey GmbH, Konstanz, Germany) was done in a subsequent visit. Post-obturation periapical radiographs were taken for both teeth to verify an acceptable root canal filling (Figure 2C, D).The patient was then referred to the prosthetic clinic for rehabilitation of the fractured tooth.A post space was created by partially removing the guttapercha leaving 4 mm for apical seal.The post space was filled with redself-curing acrylic (Inlay Pattern Resin Duralay, Reliance Dental MFG Co, Worth, IL, USA). After the acrylic had set completely, the post pattern was verified for accuracy and a core was reduced. After complete verification and adjustments of the cast metal post, cementation was done using glass ionomer luting agent (Ketac-Cem, 3MESPE, Seefeld, Germany) (Figure 3A, B). Polyvinyl siloxane impression (Elite HD, Zhermack, BadiaPolesine, Italy) was takenfor laboratory fabrication of ceramo-metal full crown. The marginal fit and occlusion of the crown were evaluated intraorally and cementation was performed using a glass ionomer cement (Ketac-Cem, 3M ESPE, Seefeld, Germany) (Figure 3C, D). The mandibular right central incisor received a bonded composite restoration (Filtek Z350 XT, 3M ESPE, St. Paul, MN, USA) to fill the endodontic access cavity. The patient was satisfied with the final results of the treatment. The clinical and radiographic evaluation at the one-month follow-up visit demonstrated that the restored teeth were in a good status and the neighboring anterior teeth remained stable with no abnormal findings. The patient was scheduled for further follow-up visits and signed an informed consent for the publication of this clinical case report.
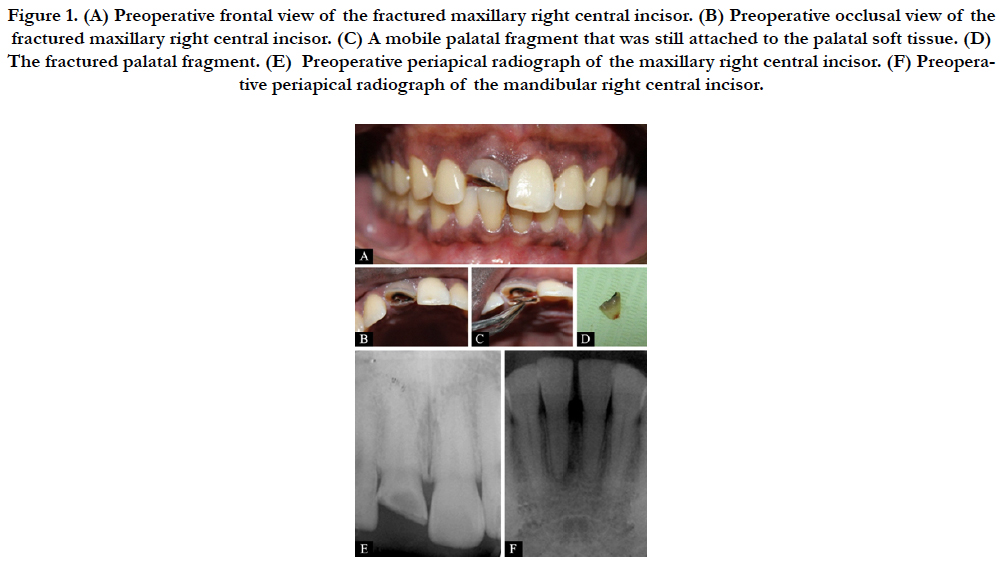

Figure 1. (A) Preoperative frontal view of the fractured maxillary right central incisor. (B) Preoperative occlusal view of the fractured maxillary right central incisor. (C) A mobile palatal fragment that was still attached to the palatal soft tissue. (D) The fractured palatal fragment. (E) Preoperative periapical radiograph of the maxillary right central incisor. (F) Preoperative periapical radiograph of the mandibular right central incisor.
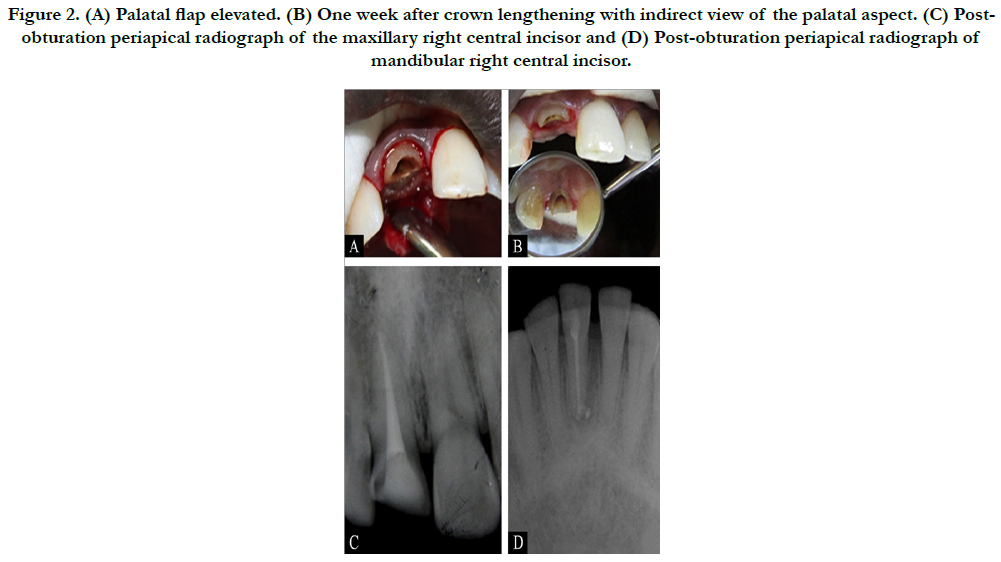
Figure 2. (A) Palatal flap elevated. (B) One week after crown lengthening with indirect view of the palatal aspect. (C) Postobturation periapical radiograph of the maxillary right central incisor and (D) Post-obturation periapical radiograph of mandibular right central incisor.
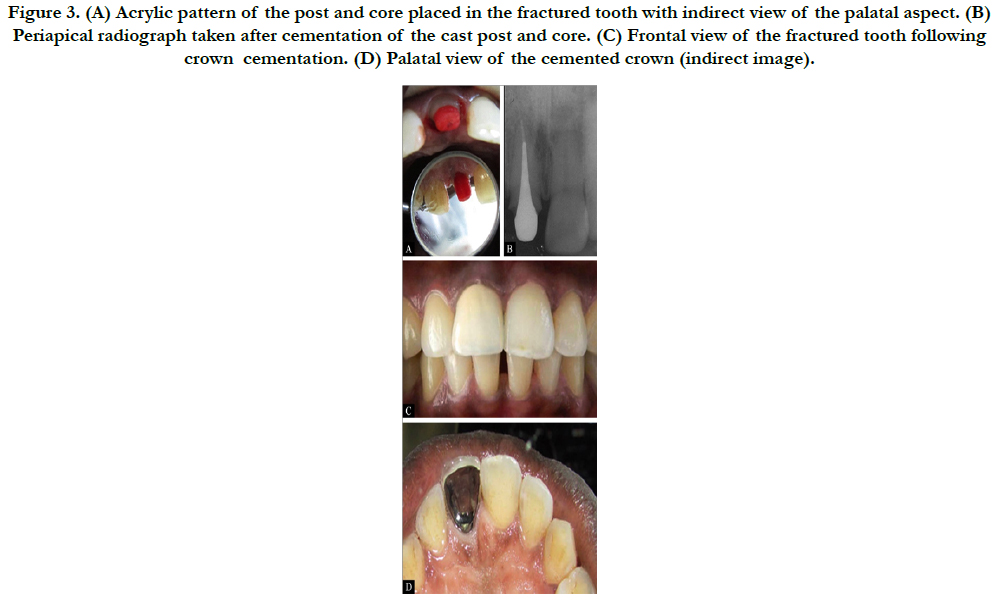
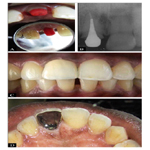
Figure 3. (A) Acrylic pattern of the post and core placed in the fractured tooth with indirect view of the palatal aspect. (B) Periapical radiograph taken after cementation of the cast post and core. (C) Frontal view of the fractured tooth following crown cementation. (D) Palatal view of the cemented crown (indirect image).
Discussion
Management of crown-root fractures presents agreat restorative challenge for the dental clinician. The challenge in the present case was amplified due to the apical extent of the fracture palatally which implied a multidisciplinary approach for treatment.
Treatment modalities for approaching crown-root fractures range from minimally invasive procedure as in fragment reattachment to a more extensive one with the whole fractured tooth being replaced [6]. Fragment reattachment using adhesive materials offers a conservative approach and immediate restoration of aesthetic and function to a traumatized anterior tooth [7, 8]. In the present case, however, the fragment reattachment could not be suggested atreatment option because of significant loss of coronal structure and the palatal fragment had a poor adaptation to the remaining tooth structure as a result of caries removal and thus could not be utilized for restorative purposes. Orthodonitc and surgical methods can be employed to expose a subgingival fracture avoiding the invasion of the biologic width. Orthodontic extrusion restores physiological periodontal attachment and preserves the alveolar bone [9] without compromising the aesthetic appearance [10]. The major limitation of this approach is that it is relatively long, expensive, uncomfortable to the patient and surgical intervention is still necessary [11]. Thus, the technique requires multiple visits and patient cooperation [12]. By contrast, surgical crown lengthening is a faster procedure but involves removing the supporting alveolar bone, produces a high gingival contour, hampering soft tissue aesthetics and decreases the crown-root ratio [11, 13]. The surgical procedure also compromises the periodontium of the adjacent non treated teeth [14]. This approach produces aesthetic problem in the anterior area, however, the palatal location of the subgingival fracture in our case permitted the exposure with a palatal flap elevation and osteotomy with minimal manipulation of the labial and interproximal tissues. In the present case, the patient refused the orthodontic treatment for financial reasons as well as for the prolonged treatment time.
Although crown lengthening procedures are usually carried out after completion of root canal therapy, the sequence is altered in case of subgingival fracture where a crown lengthening procedure can be performed initially to facilitate endodontic and prosthetic procedures [4].
Based on the clinical and the radiographic findings, maxillary and mandibular right central incisors had an endodontic diagnosis of necrotic pulp with asymptomatic apical periodontitis. To improve the outcome of root canal therapy in these teeth, calcium hydroxide was applied as an intra canal medicament. Reduction in the pathogenic species, especially in cases of necrotic pulps and periradicular lesions, was noted when calcium hydroxide was used as intra canal dressing during conventional root canal therapy [15].
The time interval between the surgical crown lengthening and the initiation of the definitive prosthesis was taken into consideration. It was observed that the free gingival margin requires a minimum of three months to establish its final vertical position following surgical crown lengthening procedure [16]. In the present case, commencement of the prosthetic phase was carried out twelve weeks after the periodontal surgery to allow for favorable tissue healing and stability of the marginal gingival.
The utilization of post system is recommended in traumatized teeth where the fracture involves two-third of the crown part [17]. The use of prefabricated post was precluded in the present case because the remaining coronal tooth structure was minimal, therefore, a cast post and core was fabricated and the tooth was restored with porcelain-fused-to-metal crown. The choice of non precious alloy cast post over gold cast post was due to patient's economic reasons.
The present case report showed the importance of cooperation between a periodontist, endodontist and a prosthodontist. The fractured maxillary right central incisor reached a satisfactory condition to meet an acceptable aesthetics and proper function. The case report also illustrated the importance ofre-establishing the biologic width when planning prosthetic restorations of teeth suffered a deep subgingival fracture.
Conclusion
A variety of clinical problems arise during rehabilitation of anterior tooth with crown-root fracture. The presence of subgingival fracture further complicates the clinical condition. Successful outcome of the present case was highly dependent on the knowledge and the skills of the multidisciplinary dental team.
References
- Lam R. Epidemiology and outcomes of traumatic dental injuries: a review of the literature. Aust Dent J.2016 Mar; 61(1):4-20. PubMed PMID: 26923445.
- Turgut MD, Gönül N, Altay N . Multiple complicated crown-root fracture of a permanent incisor. Dent Traumatol. 2004 Oct; 20(5):288-92. PubMed PMID: 15355388.
- Macedo GV, Diaz PI, De O Fernandes CA, Ritter AV. Reattachment of anterior teeth fragments: a conservative approach. J Esthet Restor Dent. 2008 Jan 25; 20(1):5-18. PubMed PMID: 18237334.
- Anand PS, Ashok S, Nandakumar K, Varghese NO, Kamath KP. Surgical exposure and crown lengthening for management of complicated fractures of maxillary anterior teeth. A case report. N Y State Dent J.2013 Nov;79(6):41-6. PubMed PMID:24600764.
- Padbury A Jr, Eber R, Wang HL. Interactions between the gingiva and the margin of restorations. J Clin Periodontol. 2003 May; 30(5):379-85. Pub- Med PMID: 12716328.
- Pavone AF, Ghassemian M, Mancini M, Condò R, Cerroni L, Arcuri C, et al. Autogenous Tooth Fragment Adhesive Reattachment for a Complicated Crown Root Fracture: Two Interdisciplinary Case Reports. Case Rep Dent 2016; 9352129. PubMed PMID: 27965901; PubMed Central PMCID: PMC5124656.
- de Castro JC, Poi WR, Pedrini D, Tiveron AR, Brandini DA, de Castro MA. Multidisciplinary approach for the treatment of a complicated crown-root fracture in a young patient: a case report. Quintessence Int. 2011Oct;42(9):729-35.PubMed PMID: 21909497.
- O'Toole S, Garvey T, Hashem A. The multidisciplinary conservative management of a vital crown root fracture. Dent Update. 2013 Sep;40(7):584-6, 588. PubMed PMID: 24147390.
- de Avila ED, de Molon RS, Cardoso Mde A, CapelozzaFilho L, Campos Velo MM, Mollo Fde A Jr, et al. Aesthetic rehabilitation of a complicated crown-root fracture of the maxillary incisor: combination of orthodontic and implant treatment. Case Rep Dent. 2014;925363. PubMed PMID: 24872900.
- Koyuturk AE, Malkoc S. Orthodontic extrusion of subgingivally fractured incisor before restoration. A case report: 3-years follow-up. Dent Traumatol. 2005 Jun;21(3):174-8. PubMed PMID: 15876331.
- Planciunas L, Puriene A, Mackeviciene G. Surgical lengthening of the clinical tooth crown. Stomatologija.2006; 8(3):88-95. PubMed PMID: 17191065.
- Aggarwal V, Logani A, Shah N. Complicated crown fractures - management and treatment options. Int Endod J. 2009 Aug;42(8):740-53. PubMed PMID: 19548932.
- Jorgensen MG, Nowzari H. Aesthetic crown lengthening. Periodontol 2000. 2001;27:45-58. PubMed PMID: 11551299.
- Nobre CM, de Barros Pascoal AL, Albuquerque Souza E, Machion Shaddox L, Dos Santos Calderon P, de Aquino Martins AR, et al. A systematic review and meta-analysis on the effects of crown lengthening on adjacent and non-adjacent sites. Clin Oral Investig. 2017 Jan; 21(1):7-16. PubMed PMID: 27515522.
- de Souza CA, Teles RP, Souto R, Chaves MA, Colombo AP. Endodontic therapy associated with calcium hydroxide as an intracanal dressing: microbiologic evaluation by the checkerboard DNA-DNA hybridization technique. J Endod.2005 Feb;31(2):79-83. PubMed PMID: 15671813.
- Hempton TJ, Dominici JT. Contemporary crown-lengthening therapy: a review. J Am Dent Assoc. 2010 Jun; 141(6):647-55. PubMed PMID: 20516094.
- Krastl G, Lorch H, Zitzmann NU, Addison O, Dietrich T, Weiger R. (2014) Do oval posts improve fracture resistance of teeth with oval root canals? Dent Traumatol. 2014 Jun;30(3):232-5. PubMed PMID: 23991722.





