Novel Approaches for Class II Malocclusion Treatment using Myofunctional Orthodontics Therapy: A Systematic Review
Ferreira FG*
Associate Professor of Specialization in Orthodontics, Pós-Odonto SUPREMA, Faculdade de Ciências Médicas e da Saúde de Juiz de Fora, Juiz de Fora, MG, Brazil.
*Corresponding Author
Fabiano Guerra Ferreira, DDS, MS, PhD,
Associate Professor of Specialization in Orthodontics,
Pós-Odonto SUPREMA, Faculdade de Ciências Médicas e da Saúde de Juiz de Fora, Juiz de Fora, MG, Brazil.
Tel: +55 32 984551816
E-mail: drfabianoguerra@ig.com.br
Received: June 12, 2017; Accepted: July 19, 2017; Published: July 20, 2017
Citation: Ferreira FG (2017) Novel Approaches for Class II Malocclusion Treatment using Myofunctional Orthodontics Therapy: A Systematic Review. Int J Dentistry Oral Sci. 4(7), 503-507. doi: dx.doi.org/10.19070/2377-8075-1700099
Copyright: Ferreira FG©2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The aim of this review was to undertake a detailed analysis of the literature concerning the use of a prefabricated functional appliance for Class II malocclusion treatment. From June 2016 to May 2017, a comprehensive and systematic search was performed on the Medline (PubMed) and Google Scholar databases for works published since January 2002, using the following search terms: pre-orthodontic trainer; pre-orthodontic trainer appliance; class II malocclusion; class II malocclusiontreatment; prefabricated functional appliance. A supplementary manual searching of other sources was also performed. Only scientific articles in the English language were considered for this review. The electronic and manual searches resulted in the identification of 71 articles. Based on the inclusion criteria, the full-text copies of 26 articles were selected for analysis. A specific analysis was then made of 15 articles that described the effects produced by using the appliance for the treatment of dentoskeletal Class II malocclusion and masticatory muscles disfunction. The Literature findings show that the prefabricated functional appliance enables the treatment of several problems associated with the development of Class II malocclusion. Although the therapy induces mainly dentoalveolar changes resulting in significant reduction of overjet, it also shows a positive influence on the masticatory and perioral musculature. The method was demonstrated to be effective to obtain significant Class II malocclusion correction.
2.Introduction
3.Material and Methods
3.1 Search Methodology
3.2 Literature Review
4.Dentoalveolar Effects Produced by POT Treatment
5.Mandible Posture and Growth and Transverse Maxillary Dimensions
6.Effects of Myofunctional Correction
7.Discussion
8.References
Keywords
Class II Malocclusion Treatment; Pre-Orthodontic Trainer; Prefabricated Functional Appliance.
Introduction
Pre-Orthodontic Trainer (POT, Myofunctional Research Co., Queensland, Australia) is a literary nomenclature commonly used to define a prefabricated functional appliance made of non-thermoplastic silicone or polyurethane which is designed to act on muscular dysfunction, providing malocclusion corrections even at an early age [1-3].
The POT appliance is fabricated with the mandible positioned anteriorly for Class II patients [4]. Its structure has components constructed to stimulate positively the facial, masticatory and tongue muscles activity [2], altering the posture of the mandible to a forward position [4] and also encouraging transverse development [5].
In previous studies, different methods have been used to evaluate the effectivity of POT therapy for Class II malocclusion treatment, such as Lateral Cephalometry, Plaster Model, and Clinical analysis [2-4]. In addition, masticatory muscles activity before and after treatment has been also examined by using, mainly, Electromyography [2, 6-8]. This technique enables the recording of the electrical activity of the muscles, allowing detection of possible muscular malfunctions, putting corrective treatment into place and verifying whether soft tissue disfunctions or parafunctions could be corrected [2].
Several benefits have been attributed to the use of the POT treatment for Class II malocclusion correction. It has been postulated that POT treatment induces muscular relaxation and it could protect teeth and articulations from bruxism, by avoiding the clenching effect [2]. The Class II correction is claimed to occur by an active mandibular force. The POT treatment is also regarded to prevent a malposition of the tongue and lower lip during swallowing, besides preventing oral breathing, factors related to the cause and maintenance of dental open bite [4]. It has been described that abnormal lip and tongue function that would directly affect dentofacial growth could be improved with POT treatment, thus promoting normal growth and treatment stability [9].
It has been also reported that the treatment beginning at the mixed dentition stage could improve its effectiveness, minimizing the need for orthodontic treatment involving permanent tooth extraction or orthognathic surgery [10].
Despite the many advantages credited to the use of POT for the treatment of Class II malocclusion, only a few scientific articles were published on this issue until now.
In this way, the aim of this Systematic Review was to undertake a detailed analysis of the Literature concerning the effects produced by the use of the pre-orthodontic trainer appliance (POT) for the treatment of dentoskeletal Class II malocclusion and masticatory muscles disfunction.
Between June 2016 and April 2017, a comprehensive electronic search in the Medline (PubMed) and Google Scholar databases was undertaken to select scientific academic articles with fulltext in English language published since January 2002, using the search terms: pre-orthodontic trainer; pre-orthodontic trainer appliance; class II malocclusion; class II malocclusion treatment; prefabricated functional appliance. A supplementary manual searching of other sources was also performed. It was applied a prespecified search strategy: The terms “pre-orthodontic trainer” AND “class II malocclusion” were used in PubMed advanced articles searches whereas for Google Scholar, the joint terms “pre-orthodontic trainer appliance and class II malocclusion treatment” found in any part of the manuscripts text were considered for articles selection. For supplementary manual searches, the term “prefabricated functional appliance” was used. According to the inclusion criteria, the articles were required to describe the effects produced by the functional appliance on the treatment of Class II malocclusion and on the masticatory muscles.
The electronic and manual searches resulted in the identification of 71 articles. The abstracts were first screened to eliminate duplicates and articles that clearly failed to meet the search criteria. Full-text copies of the remaining articles were then methodically examined to establish whether the inclusion criteria were met (Figure 1). Retrospective, controlled clinical trials and case studies were considered in this Review.
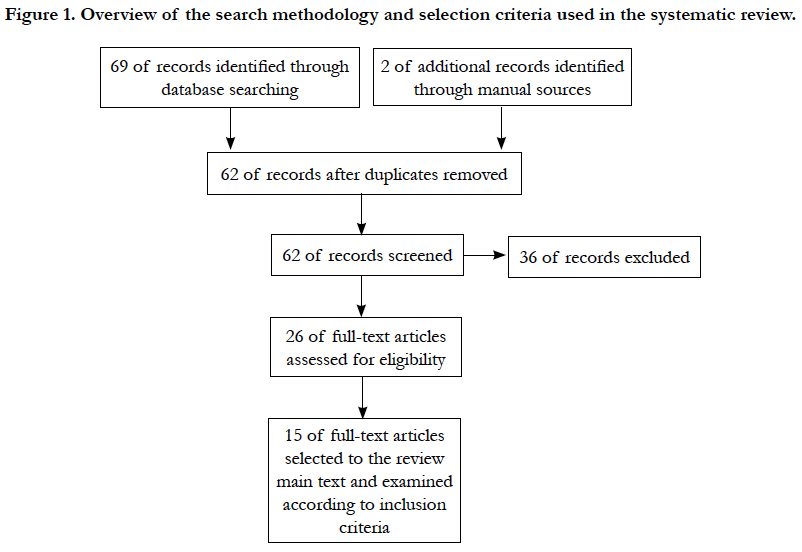
Figure 1. Overview of the search methodology and selection criteria used in the systematic review.
The literature review was organized into three sections: (i) dentoalveolar effects produced by POT treatment; (ii) mandible posture and growth and transverse maxillary dimensions; and, (iii) effects of myofunctional correction. The study design and the treatment protocol used in the studies are shown in Table 1.
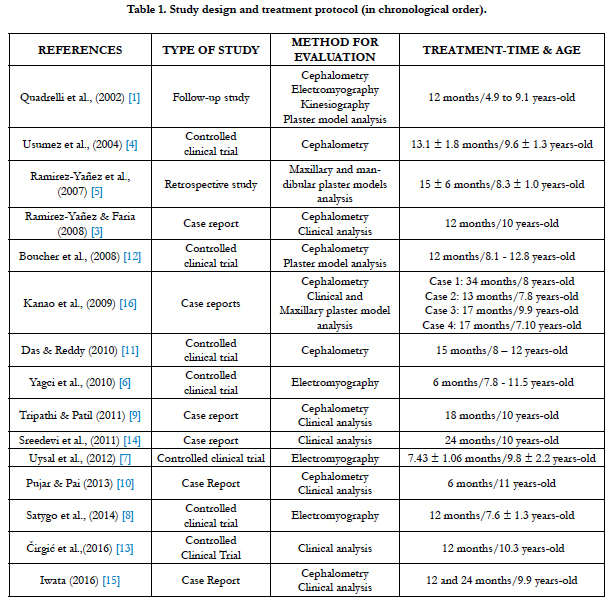

Table 1. Study design and treatment protocol (in chronological order)..
Dentoalveolar Effects Produced by POT Treatment
A variety of studies has compared groups of Class II malocclusion patients treated by POT appliance with control groups composed of untreated Class II malocclusion patients [4, 11, 12].
Using lateral cephalometry analysis, Usumez et al., (2004) [4] reported significant alterations in dentoalveolar patterns in subjects after treatment with POT including a higher increase in the total facial height, lower incisor proclination, and overjet reduction. Likewise, improvements in overjet, inclination of mandibular incisor and vertical dimensions of the face were observed by Das and Reddy (2010) [11]. Although the authors reported that the dentoalveolar effects appeared to be more relevant, they concluded that small significant skeletal effects could be achieved with this therapy.
Otherwise, when comparing the clinical effectiveness in reducing large overjet between a Prefabricated Functional Appliance (PFA) and a modified Andresen Activator (AA), Čirgić et al., (2016) [13] reported a low rate of clinical success with the use of both appliances.
After investigating and comparing the effects of the treatment with POT in Class II malocclusion late mixed dentition patients after rapid palatal expansion with a control group composed of patients treated merely with palatal expansion, Boucher et al., (2008) [12] noted a significant decrease in overjet due to dentoalveolar effects produced by the myofunctional therapy. Even though both groups had similar maxillary and mandibular expansion, the POT appliance treatment improved anteroposterior dental relationships between the upper and lower jaw.
Under a pilot study, Quadrelli et al., (2002) [2] described the efficiency of early treatment of malocclusion in skeletal Class II patients. The results showed reductions in overjet and overbite and an improvement in jaw relationship. A reduction of a deep bite was also found by Sreedevi et al., (2011) [14] when reporting the findings of a clinical case study.
In addition, after analyzing a Class II division 1 patient treated with POT, Ramirez-Yãnez & Paulo Faria (2008) [3] revealed an improvement in the intermaxillary relationship with a deepbite correction and a molar and canine Class I relationship. The cephalometric evaluation showed better values for SNA, SNB and ANB angles compared to normal. In the same way, the anteriorposterior growth of maxilla and mandible by the analysis of Co-Gn, Co-A and ANS-Me distances were positively modified producing higher numbers than those expected from natural growth. Similarly, Triphati et al., (2011) [9] and Pujar & Pai (2013) [10] observed that a Class I molar and a skeletal relationship was obtained after a Class II division 1 treatment with the POT appliance in a case study.
By the outcomes of a case study, Iwata (2016) [15] reported a reduction in upper incisors proclination after the POT treatment of a Class II malocclusion.
Mandible Posture and Growth and Transverse Maxillary Dimensions
Changes in the mandible posture and growth as well as in the transverse maxillary dimensions were described in some studies [4, 11, 12, 16].
After evaluating Class II malocclusion patients treated with the pre-orthodontic trainer and comparing them to a control group composed of untreated subjects, Das & Reddy (2010) [11] observed a forward rotation of mandible with a significant increase in the vertical dimensions of the face in general in groups of patients using POT. A previous case report study revealed a mandibular growth and an inferior anterior facial height increase in a patient treated with POT. These characteristics were attributed to a forward mandibular repositioning (Ramirez-Yãnez&Faria, 2008) [3]. A significant mandibular growth produced by POT treatment was also observed by Boucher et al., (2008) [12].
Under a retrospective study, Ramirez-Yanez et al., (2007) [5] reported a clinically significant increase of both maxillary and mandibular dental arches in Class II malocclusion patients treated with the T4K. The authors claimed that T4K is an effective tool for transverse expansion of dental arches when it is an essential goal for the treatment. Similar results had been showed by other studies when evaluating patients treated with POT [2, 15].
Effects of Myofunctional Correction
Myofunctional effects generated by the POT treatment have been outlined in the Literature [2, 6-8].
The POT treatment effects on the anterior temporal, mental, orbicularis, and masseter muscles were noted by Uysal et al., (2012) [7]. The electromyography (EMG) analysis in Class II division after treatment showed a decrease of anterior temporal, mental, and masseter muscles with an increasing activity of orbicularis muscles when the patients were in clenching teeth. The outcomes pointed out a favorable impact of the treatment to the masticatory and perioral musculature. These results were corroborated by the study of Yagci et al., (2010) [6]. Similarly, the authors described a significant improvement in the perioral and masticatory muscles after POT treatment.
Likewise, the muscular activity the Masseter and Temporalis muscles in Class II division 1 patients treated with POT was also examined by Satygo et al., (2014) [8]. The examination was conducted with patients clenching their teeth. The outcomes demonstrated that the POT treatment significantly increased the EMG muscular activity in the Temporalis and Masseter muscles. A decrease in masseter muscle activity provided by the Trainer treatment was also cited by Quadrelli et al. (2002) [2] after analyzing two clinical follow-up studies.
Discussion
The disfunction of masticatory muscles is reported to be behind of causing and maintaining dental and skeletal Class II malocclusion. At the same time, according to the manufacturer, the preorthodontic trainer appliance (POT) incorporates myofunctional characteristics that can treat dysfunctional habits, reducing excessive mentalis muscle activity and tongue thrusting, besides inducing nasal breathing. Furthermore, the appliance has components to guide dentition to developing into correct alignment and to provide improvements to the transversal maxillary growth while repositioning the mandible in an adequate relationship with the upper jaw [1].
A wide range of study findings has pointed out that the treatment with the POT appliance influences positively on the masticatory and perioral musculature. It is claimed to be effective for Class II malocclusion and masticatory muscles and facial soft tissues treatment beyond having an impact on bone growth, which would influence the process and stability of orthodontic treatment [6]. Studies have shown that the appliance can stimulate mandibular growth and increase the vertical face dimension [3].
Anyway, further studies are required to determine how significant the activity of the masticatory muscles may affect the growth and development of the maxillaries.
Nonetheless, the POT appliance may be as effective to treat Class II, division 2 malocclusion at an early age as well as it has been demonstrated to be for Class II, division 1 malocclusion [3]. Furthermore, the method is claimed to be a valuable tool for improving dental arch development when a lack of transverse development is diagnosed at an early age [5].
The Literature findings show that the pre-orthodontic trainer application induces mainly dentoalveolar changes that result in significant reduction of overjet [4] and thus being effective for Class II malocclusion treatment.
By the outcomes of this Review, it can be concluded that, although case selection must be done with utmost care, the POT appliance enables the treatment of several problems associated with the development of Class II malocclusion, thus permitting to deal with them at different aspects. Significant Class II malocclusion correction can be achieved by using the pre-orthodontic rainer appliance therapy.
Nevertheless, further long-term follow-up studies should be carried out to verify the positive influence of POT treatment on large groups of skeletal class II division 1 and 2 malocclusion subjects at a time by using new investigation methods in order to compare and corroborate the outcomes obtained by the technique used so far.
References
- Myofunctional Research Co. (2017)
- Quadrelli C, Gheorgiu M, Marchetti C, Ghiglione V (2002) Early myofunctional approach to skeletal Class II. Mondo Ortod. 27(2): 109-22.
- Ramirez-Yañez GO, Faria P (2008) Early treatment of a Class II, division 2 malocclusion with the Trainer for Kids (T4K): a case report. J Clin Pediatr Dent. 32(4): 325-9.
- Usumez S, Uysal T, Sari Z, Basciftci FA, Karaman AI, et al., (2004) The effects of early preorthodontic trainer treatment on Class II, division 1 patients. Angle Orthod. 74(5): 605-9.
- Ramirez-Yañez G, Sidlauskas A, Junior E, Fluter J (2007) Dimensional changes in dental arches after treatment with a prefabricated functional appliance. J ClinPediatr Dent. 31(4): 279-83.
- Yagci A, Uysal T, Kara S, Okkesim S (2010) The effects of myofunctional appliance treatment on the perioral and masticatory muscles in Class II, Division 1 patients. World J Orthod. 11(2): 117-122.
- Uysal T, Yagci A, Kara S, Okkesim S (2012) Influence of pre-orthodontic trainer treatment on the perioral and masticatory muscles in patients with Class II division 1 malocclusion. Eur J Orthod. 34(1): 96-101.
- Satygo EA, Silin AV, Ramirez-Yañez GO (2014) Electromyographic Muscular Activity Improvement in Class II Patients Treated With the Pre-Orthodontic Trainer. J ClinPediatr Dent. 38(4): 380-4.
- Tripathi NB, Patil SN (2011) Treatment of Class II Division 1 Malocclusion With Myofunctional Trainer System in Early Mixed Dentition Period. J Contemp Dent Pract. 12(6): 497-500.
- Pujar P, Pai SM (2013) Effect of Preorthodontic Trainer in Mixed Dentition. Case Rep Dent. 2013: 717435, 6.http://dxdoi.org/10.1155/2013/717435.
- Das UM, Reddy D (2010) Treatment effects produced by preorthodontic trainer appliance in patients with class II division I malocclusion. J Indian Soc Pedod Prev Dent. 28(1): 30-33.
- Boucher C, Charezinski M, Balon-Perin A, Janssens F, Vanmuylder N, et al., (2008) Benefits of using a Trainer T4K® myofunctional appliance after rapid palatal expansion: a prospective study on thirteen patients. J Dentofacial Anom Orthod. 11(1): 30-44.
- Čirgić E, Kjellberg H, Hansen K (2016) Treatment of large overjet in Angle Class II: division 1 malocclusion with Andresen activators versus prefabricated functional appliances-a multicenter, randomized, controlled trial. Eur J Orthod. 38(5): 516-24.
- Sreedevi D, Rajesh RNG, Sanjay N, Rekha P (2011) Correction of Deep Bite with a Functional Trainer. World J Dent. 2(4): 360-362.
- Iwata T (2016) Effects of a Prefabricated Functional Appliance in the Early Mixed Dentition Period. Pediatr Dent Care. 1: 104. doi:10.4172/ pdc.1000104.
- Kanao A, Mashiko M, Kanao K (2009) Application of functional orthodontic appliances to treatment of Mandibular Retrusion Syndrome. Japanese J Clin Dent Child. 14(4): 45–62.





