Jaws and Dental Panoramic Radiographic Findings in the Elderly in Kerman, Iran
Navabi N1, Haghani J2, Raaigan R3, Hashemipour MA1*
1 Associate Professor of Oral Medicine, Department of Oral Medicine, Dental School, Kerman University of Medical Science, Kerman, Iran.
2 Associate Professor of Oral Radiology, Department of Oral Radiology, Dental School, Kerman University of Medical Science, Kerman, Iran.
3 Dentist, Dental School, Kerman University of Medical Science, Kerman, Iran.
*Corresponding Author
Maryam Alsadat Hashemipour DDS.MSc,
Associate Professor of Oral Medicine,
Department of Oral Medicine, Dental School,
Kerman University of Medical Science, Kerman, Iran.
Tel: 00989132996183, 00983432118073
Fax: 00983412118073
E-mail: m_s_hashemipour@yahoo.com
Received: April 08, 2017; Accepted: May 24, 2017; Published: May 26, 2017
Citation: Navabi N, Haghani J, Raaigan R, Hashemipour MA (2017) Jaws and Dental Panoramic Radiographic Findings in the Elderly in Kerman, Iran. Int J Dentistry Oral Sci. 4(5), 481-486. doi: dx.doi.org/10.19070/2377-8075-1700094
Copyright: Hashemipour MA©2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background and Aim: A rapid aging of the human population has taken place in recent years. Aging associates with numeral changes in oral and maxillofacial structures. The aim of this study was to quantify the frequency of panoramic radiographic findings in the elderly.
Materials and Methods: Panoramic radiographs from 196 patients aged 60 years and older were evaluated at the private clinic for the presence of items such as alveolar bone loss, dental caries, retained roots, impacted teeth, radiolucencies, and radiopacities.
Results: One or more of these radiographic observations were found in 94.9 % of the examined films. The most frequent findings were alveolar bone loss (79.6 %) and dental caries (79.43%). The total number of natural teeth in men was significantly higher than women (P = 0.047).
Conclusion: These results showed the importance of panoramic examination of elderly patients in detecting potential problems before the treatments such as complete denture and also for assessment of overall oral health in the elderly.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Acknowledgement
7.References
Keywords
Jaws; Dental; Panoramic; Elderly.
Introduction
The proportion of the elderly population is increasing all over the world, which will have drastic effects on the general and oral health of the whole population in future. The population over 65 years of age comprised 40.3 million people of the American population in 2010, with an increase of 5.3 million people compared to that in 2000 and it is expected to reach 72 million people in 2030. It is estimated that the number of such people will increase to 8.5 million people in 2050 [1, 4]. These clear changes in the proportion of the elderly people in the population are attributed to advances in the medical field in treating life-threatening conditions as one of most important reasons, and they have prompted dental practitioners to acquire the knowledge to treat geriatric dental patients and become familiar with the specific oral manifestations during aging processes [5].
Unfortunately, many elderly individuals do not receive proper dental services despite their great need. In a study, 81% of the elderly had oral lesions and 20% needed immediate evaluation of their oral diseases [6]. Less than one-third of geriatric patients have regular annual dental visits and almost half of them are not examined by a dentist in a 5-year period [7]. Therefore, the elderly should receive dental services in a more ideal manner. More than 70% of the elderly in the community are able to refer to a dentist to receive the relevant services [8].
The elderly are affected by various oral disorders, including oral mucosal problems, oral sensory and motor disturbances, xerostomia, dental caries and periodontal diseases, which negatively influence their nutrition, social relations, susceptibility to infection and quality of life [9-14]. The outcomes of these oral disorders for the elderly are so serious that their life might be threatened. Oral mucous lesions are seen in up to 40% of the elderly [6, 9-14]. By considering the oral manifestations of the elderly and evaluation of the relevant reference sources it becomes evident that the osseous manifestations of the jaws in these patients have not received adequate attention and since no similar studies have been carried out in Iran to date, the present study was designed in order to increase the basic epidemiological knowledge on the elderly population of the community for future programming to promote the orodental health status in this group in the community.
Materials and Methods
In this cross-sectional study the archives of digital radiographs of an oral and maxillofacial radiology center in Kerman were used from 2012 to 2015. The digital radiographs of patients over 60 year of age, who lived in Kerman, were evaluated in the present study. All the radiographs evaluated had high quality without any gross distortion. The exclusion criteria consisted of a history of diseases that affected the bones, including diabetes, a history of chemotherapy, a history of radiotherapy for cancer, a history of osteoporosis and use of corticosteroids.
All the radiographs had been taken under standard conditions, based on the guidelines of the x-ray unit manufacturers with Crane XD x-ray machine (Sordex, Finland) under the supervision of an oral and maxillofacial radiologist. The exposure conditions for all the radiographic techniques consisted of kVp=63-81 mA=10 and s=17. The radiographs were visualized on a 19-inch Flatron LG W1952SE monitor with adjustable magnification up to 100% and the possibility to adjust light [15, 16]. Scanora A.3.1 software program was used to this end. All the eligible radiographs were visualized by an experienced oral and maxillofacial radiologist and the following radiographic findings were recorded [15-19]: the number of natural teeth in both arches except for wisdom teeth, the number of residual roots, the number of impacted teeth, presence of fixed prostheses (bridges) and implants, the number of endodontically treated teeth, presence of boney pockets, involvement of the furcal area, presence of calculus, the number of teeth with visible carious lesions, radiolucent lesions involving and not involving bone, radiopaque lesions, findings in relation to the condyle of the TMJ, and resorption of the alveolar bone (localized resorption of bone secondary to etiologic agents such as overhanging restorations).
Data were analyzed with the latest versions of SPSS. Central and distribution parameters were used for descriptive data and chisquared test was used to evaluate the relationship between clinical variables at P<0.05. Z-test was used at Z ≥ 1.96 and independent t-test (sig 2-tailed) was used at CI=95%. The subjects’ personal data were kept confidential throughout the study.
Results
A total of 196 panoramic radiographs of patients, aged over 60 years, were evaluated in the present study in relation to the dental and maxillofacial statuses. Table 1 presents the frequency distributions of the subjects, including age, gender, the number of natural and impacted teeth, the number of endodontically treated teeth and the residual roots. The mean age of the patients was 65.52 ± 5.5 years with a range of 60-90 years. The mean number of natural teeth in the subjects was 11.22 ± 9.38, with a maximum of 30 teeth. In addition, in cases in which residual teeth was detected the range was 2-7 roots. The mean number of carious lesions was 2.13 and a maximum of 18 such lesions were recorded in one subject.
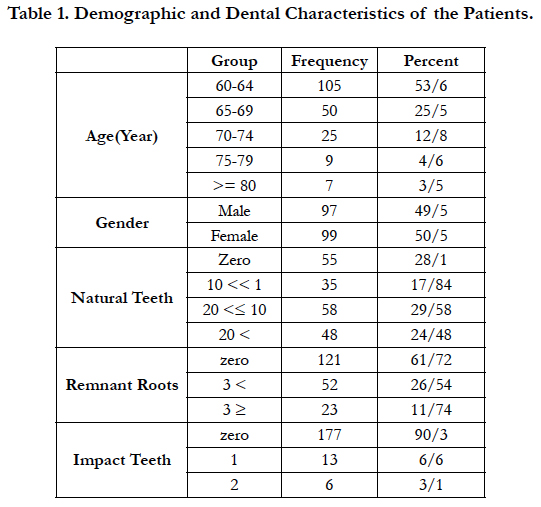

Table 1. Demographic and Dental Characteristics of the Patients.
As shown in Table 1, residual roots were observed in 38.28% of the subjects. The prevalence rate of impacted teeth was 9.7%, and 50% of the subjects (98 patients) had at least one endodontically treated tooth.
Table 2 presents the frequencies and percentages of 11 dentoalveolar items in the subjects. As shown in the table, resorption of bone had the highest prevalence rate (79.6%) among the items evaluated and the least frequency was related to non-tooth-associated radiolucencies with 4.6%.
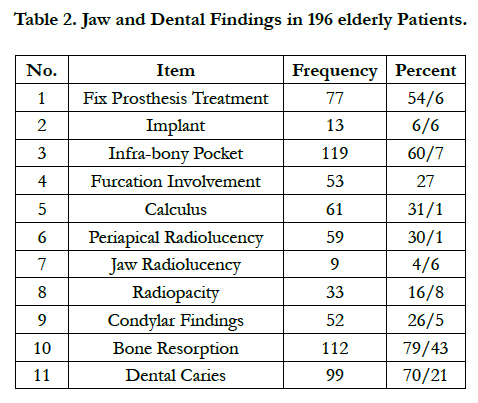
Table 2. Jaw and Dental Findings in 196 elderly Patients.
In order to calculate the frequency of caries in the population under study, edentulous subjects were excluded from the study and the dental caries rate was determined in subjects with at least one natural tooth. In this context, dental caries was the second most prevalent dentoalveolar item in the subjects.
Statistical analysis showed that the number of natural teeth in male subjects was significantly higher than that in female subjects (P=0.47).
By considering all the pathologic dentoalveolar items (10 items in the present study), 94.9% of the radiographs had at least one of these items: residual roots, impacted teeth and items 3 to 11 in Table 2.
Figures 1 to 3 demonstrate three examples with interesting findings in our cases.
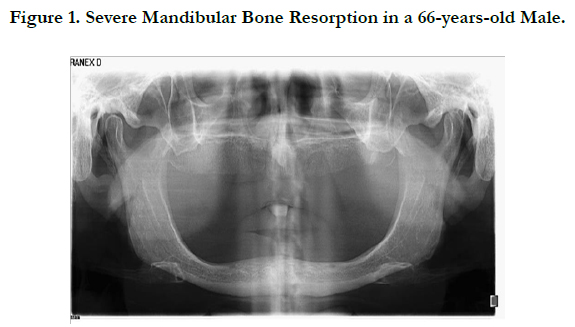

Figure 1. Severe Mandibular Bone Resorption in a 66-years-old Male.
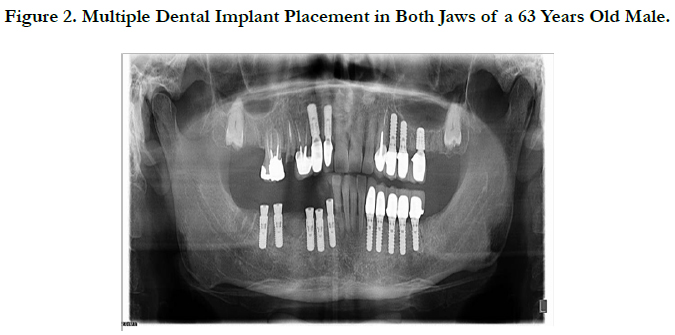

Figure 2. Multiple Dental Implant Placement in Both Jaws of a 63 Years Old Male.
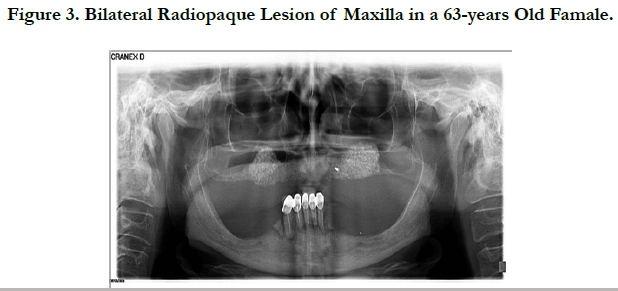
Figure 3. Bilateral Radiopaque Lesion of Maxilla in a 63-years Old Famale.
Discussion
In the present study, evaluation of dentoalveolar findings on the panoramic radiographs of subjects over 60 years of age showed that 94.9% of the subjects had at least one of the 10 pathologic entities evaluated, which was much higher than the values reported by Summer (47.6%), Masood (42.5%), Jindal (32%) and Awad and Al-Dharrab (51.7%) [19-22]. It should be pointed out in relation to these discrepancies that the studies above have not included dental caries as a pathologic entity in their reports on ‘at least one pathologic finding’ and have made no mention of cases such as boney pockets, furcal involvement and condylar findings; however, all the findings in the present study have been included in calculations to determine the presence of at least one pathologic finding in the results.
Another difference between the report of pathologic items between the present study and other similar studies is the frequency of the report of 3 items, including the mental foramen at the residual alveolar ridge in studies by Award, (Al-Dharrab, Jindal), the proximity of the maxillary sinus floor to the maxillary alveolar ridge in the study by Awad and Al-Dahrrab and thickening of the maxillary sinus mucosa in a study by Soikkonen [17, 21, 22]. These 3 items were not included in the present study because the study methodology was based on observation without estimating the distances on the radiographs.
Studies by Sumer, Masood, Soikkonen and Jindal focused on edentulous elderly subjects [17, 19-21], which resulted in the exclusion of items such as dental caries, calculus and furcal involvement from their studies; however, studies such as that by Ainamo, similar to the present study, focused on the elderly, both dentate and edentulous [16].
In a number of studies, the panoramic radiographs of the elderly have been evaluated using quantitative methods, including studies by Joo, Humphries, Sofat and Haster [23-26]. The quantitative evaluations carried out in these studies consisted of changes in the gonial angle and the height of the mandibular bone (vertical resorption) with aging, indexes such as mental index, mandibular cortical index and mandibular index. In some other studies the radiographic evaluations have focused on some special cases. In this context, a study by Mathew evaluated the maxillary sinus findings such as mucous retention cysts on panoramic radiographs of the elderly [27]. N’Guyen evaluated the palate on the radiographs of the elderly [28] and Celia dedicated their specific radiographic evaluation to the prevalence of elongated styloid process in the elderly [29].
Alveolar bone resorption was the most prevalent pathologic entity among the items evaluated in the present study (79.6%). The prevalence of bone resorption was higher in studies by Packota (100%) and Soikkonen (95%) compared to the present study [15, 18]. Other items related to periodontal diseases had significant prevalence rates in the present study and furcal involvement (27%), osseous pockets (60.7%) and calculus (31.1%) were other prevalent entities. Ainamo reported prevalence rates of 51% and 28% for osseous pockets and furcal involvement, respectively, which are similar to those in the present study [16, 18]. It appears it is difficult to compare the results of different studies and to accurately evaluate the factors affecting such resorption, considering the multiplicity of factors that affect it, including systemic predispositions such as diabetes and also use of tobacco [30].
In the present study, the prevalence rates of periapical radiolucencies and non-tooth-associated radiolucencies were 30.1% and 4.6%, respectively. Ainamo reported a prevalence rate of 41% for periapical periodontitis [16]. Soikknonen and Jindal reported prevalence rates of 3% and 2.5% for non-tooth-associated radiolucencies; the values reported in the three studies above were close to the results of the present study [18, 21]. In the differential diagnosis of such radiolucencies attention should be paid to cases such as osteoporotic spaces in bone (especially in the mandible) and widening of periodontal ligaments of teeth due to inflammation. In addition, it should be kept in mind that the definitive diagnosis of some of these entities is not possible without taking a medical history and clinical examination along with it or even taking biopsies.
In the present study, the prevalence rate of radiopacities on panoramic radiographs was 16.8%, with 13% and 9.9% rates being reported by Soikkonen and Jindal, respectively [18, 21]. It should be kept in mind that differential diagnosis is sometimes difficult on panoramic radiographs and entities such as residual roots, salivary gland stones, calcified lymph nodes, foreign bodies, condensing osteitis and calcified tonsillitis, should be considered.
In the present study, there were reports about some dental treatments such as fixed prostheses, root canal treatment and implants on the radiographs of the elderly subjects but no similar report was found in the literature. The relatively high prevalence of endodontically treated teeth in dentate subjects (70.21%) and the high prevalence rate for fixed prostheses (54.6%) and even dental implants (6.6%) in the present study shows that patients are becoming more and more interested in receiving routine and advanced dental therapeutic care in the community.
In the present study, 26.5% of the radiographs revealed signs of the involvement of the articular surfaces of the temporomandibular joint. Soikkonen reported a prevalence rate of 17% for such a condition [17]. Some other studies which have evaluated changes in TMJ in the elderly are studies by Wolf and Hiltunnen [31, 32]; however, definitions used by these two researches for reporting pathologic changes in the TMJ are somewhat different from that used in the present study.
The second most common finding in the present study was dental caries (79.43%). In the study carried out by Packota, too, 87% of patients had at least one carious tooth; in the study by Ainamo, this rate was 75%, which was close to that in the present study [15, 16]. In relation to reporting dental caries rate it should be kept in mind that it is not easy to diagnose different types of caries on panoramic radiographs.
In the present study, 28.1% of patients were completely edentulous and the prevalence rates for residual roots and impacted teeth were 38.28% and 97%, respectively. Packota reported a prevalence rate of 37% for complete edentulism [15]. The prevalence rates of residual roots in studies carried out by Ainamo, Soikkonen and Jindal were 4.8, 4 and 7%, respectively, which are much lower than that in the present study. The rates of impacted teeth in the three studies above were 6.4%, 9% and 15%, respectively with only the percentage reported by Ainamo being a little different from that in the present study [16, 17, 21]. Residual roots and impacted teeth have already been evaluated in patients before removable prosthetic treatments.
In the present study, the number of natural teeth in men was significantly higher than that in women. A more accurate analysis of the results showed that the number of female subjects over 80 years of age was much higher and if aging is considered a factor for the aggregation of reasons for tooth loss, such as periodontal disease and dental caries, this factor might have been responsible for the shifting of this factor toward significance and the presence of more teeth in men compared to women. Forty years ago the majority of adults believed that loss of tooth is a natural component of aging; however, tooth loss during old age occurs due to periodontal diseases and dental caries [7, 11, 31]. Studies show that the number of teeth in the elderly is more than that in the past; in this context, less than 27% of the population over 65 years of age is edentulous while 60 years ago this percentage was more than 50%. Therefore, the elderly are at a higher risk for the serious systemic complications with dental origin and more attention should be directed toward their oral health compared to previous generations [32]. The majority of researchers have reported in the results of studies, which have been very similar to the results of the present study, that panoramic radiography is a very good and cost-effective diagnostic tool to determine dental and jaw bone changes in the elderly, with reliable accuracy for determining possible problems before undertaking some treatments in such patients, including removable prostheses. The following suggestions are made after analysis of the results of the present study:
• Due to differences in the dental and alveolar items detected in the elderly subjects between different studies it is suggested that a comprehensive systematic review be carried out in this respect so that more accurate numeric values can be reported by aggregating the rests of these studies.
• It is suggested that in future studies dental and alveolar items be evaluated in the elderly that have not drawn attention to date, including tooth attrition that was evident on some of the radiographs evaluated in the present study.
• More accurate evaluation of dental and alveolar manifestations of the elderly patients requires recording some cases in their history during clinical examinations; therefore, a more comprehensive study can be carried out in this field and apart from the evaluation of panoramic radiographs of the patients, the above sources, too, can be used for recording of useful data.
• Newer imaging techniques, such as CBCT, too, can be used for more accurate registration of some signs such as condyle findings and radiopaque and radiolucent lesions.
Acknowledgement
This study was financially supported by Kerman University of Medical Sciences (Research No: 93/227). The authors wish to thank sincere cooperation of this center. This paper has been written from thesis number 881 of Kerman dental school.
References
- Fure S (2004) Ten-year cross-sectional and incidence study of coronal and root caries and some related factors in elderly Swedish individuals. Gerodontol. 21(3): 130-40.
- Abdulla A, Adams N, Bone M, Gazffin J, Jones D, et al., (2013) Guidance on the management of pain in older people. Age Age. 42(1): i1-i57.
- Friedman PK (2014) Geriatric Dentistry Caring for Our Aging Population. (1st Edn)., Ames, Iowa, John Wiley & Sons, Inc. USA.
- Anand S, Johansen KL, Kurella Tamura M (2014) Aging and chronic kidney disease: the impact on physical function and cognition. J Gerontol A Biol Sci Med Sci. 69A(3): 315–322.
- López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G (2013) The hallmarks of aging. Cell .153(6): 1193-217.
- Weening-Verbree L, Huisman-de Waal G, van Dusseldorp L, van Aschterberg, Schoonhoven L, et al., (2013) Oral health care in older people in long term care facilities: a systematic review of implementation strategies. Int J Nurs Stud. 50(4): 569–582.
- Lloyd PM (1998) Oral and dental problems. Practical Ambulatory Geriatrics. (2nd Edn), St. Louis, Mosby– 412-422.
- Gluzman R, Katz RV, Frey BJ, McGowan R (2013) Prevention of root caries: a literature review of primary and secondary preventive agents. Spec Care Dent. 33(3): 133–140.
- Glick M (2015) Burket’s Oral Medicine. (12th edn), Shelton, Connecticut, People’s Medical Publishing House-USA.
- Little JW, Falace DA, Miller CS, Rhodus NL (2002) Oral Cancer: Dental Management of the Medically Compromised Patient. (6th edn), St. Louis, Mosby. 387-417.
- Ship JA, Mohammad AR (1999) Clinician’s Guide to Oral Health in Geriatric Patients, (1st Edn), Baltimore, the American Academy of Oral Medicine.
- Shulman JD, Beach MM, Rivera-Hidalgo F (2004) The prevalence of oral mucosal lesions in U.S. adults: Data from the Third National Health and Nutrition Examination Survey, 1988-1994. J Am Dent Assoc. 135(9): 1279-86.
- Weyant RJ, Newman AB, Kritchevsky SB, Bretz WA, Ren D, et al., (2004) Periodontal disease and weight loss in older adults. J Am Geriatr Soc. 52(4): 547-53.
- Promsudthi A, Pimapansri S, Deerochanawong C, Kanchanavasita W (2005) The effect of periodontal therapy on uncontrolled type 2 diabetes mellitus in older subjects. Oral Dis 11(5): 293-8.
- Packota GV, Hoover JN, Bell R (1991) Radiographic findings in a group of elderly patients at a Canadian dental school. J Can Dent Assoc. 57(5): 407-9.
- Ainamo A, Soikkonen K, Wolf J, Siukosaari P, Erkinjuntti T, et al., (1994) Dental radiographic findings in the elderly in Helsinki, Finland. J Acta Odontol Scand. 52(4): 243-9.
- Soikkonen K, Ainamo A, Wolf J, Xie Q, Tilvis R, et al., (1994) Radiographic findings in the jaws of clinically edentulous old people living athome in Helsinki, Finland. Acta Odontol Scand. 52(4): 229-33.
- Soikkonen K, Wolf J, Närhi T, Ainamo A (1998) Radiographic periodontal findings in an elderly Finnish population. J Clin Periodontol. 25(6): 439-45.
- Sumer AP, Sumer M, Güler AU, Biçer I (2007) Panoramic radiographic examination of edentulous mouths. Quintessence Int. 38: e399-403.
- Masood F, Robinson W, Beavers KS, Haney KL (2007) Findings from panoramic radiographs of the edentulous population and review of the literature. Quintessence Int. 38(6): e298-305.
- Jindal SK, Sheikh S, Kulkarni S, Singla A (2011) Significance of pre-treatment panoramic radiographic assessment of edentulous patients--a survey. Med Oral Patol Oral Cir Bucal. 16(4): e600-6.
- Awad EA, Al-Dharrab A (2011) Panoramic radiographic examination: a survey of 271 edentulous patients. Int J Prosthodont. 24(1): 55-7.
- Joo JK, Lim YJ, Kwon HB, Ahn SJ (2013) Panoramic radiographic evaluation of the mandibular morphological changes in elderly dentate and edentulous subjects. Acta Odontol Scand. 71(2): 357-62.
- Humphries S, Devlin H, Worthington H (1989) A radiographic investigation into bone resorption of mandibular alveolar bone in elderly edentulous adults. J Dent. 17(2): 94-6.
- Sofat A, Galhotra V, Gambhir RS, Garg SK (2013) An Analysis of the Vertical Bone Loss in Edentulous Mandibles by Using the Mental Foramen as a Reference: A Radiographic Study. J Clin Diagn Res. 7(7): 1508-10.
- Hastar E, Yilmaz HH, Orhan H (2011) Evaluation of mental index, mandibular cortical index and panoramic mandibular index on dental panoramic radiographs in the elderly. Eur J Dent. 5(1): 60-7.
- Mathew AL, Pai KM, Sholapurkar AA (2009) Maxillary sinus findings in the elderly: a panoramic radiographic study. JCDP. 10(6): E041-8.
- N’Guyen T, Ayral X, Vacher C (2008) Radiographic and microscopic anatomy of the mid-palatal suture in the elderly. Surg Radiol Anat. 30(1): 65–8.
- Rizzatti-Barbosa CM, Ribeiro MC, Silva-Concilio LR, Hipolito OD, Ambrosano GM (2005) Is an elongated stylohyoid process prevalent in the elderly? A radiographic study in a Brazilian population. Gerodontol. 22(2): 112–5.
- Soikkonen K, Ainamo A, Xie Q (1996) Height of the residual ridge and radiographic appearance of bony structure in the jaws of clinically edentulous elderly people. J Oral Rehabil. 23(7): 470-5.
- Hiltunen K, Peltola JS, Vehkalahti MM, Närhi T, Ainamo A (2003) A 5-Year Follow-up of Signs and Symptoms of TMD and Radiographic Findings in the Elderly. Int J Prosthodont 16 (6): 631-4.
- Wolf J, Kononen M, Makila E (1995) Radiographic signs in the TMJ and finger joints in elderly people. J Oral Rehabil. 22(4): 269-74.





