Influence of Ceramic Laminate Veneer Thickness on Sorption and Solubility of Light-Cured Resin Cement
Mathias C1*, Vitoria LA2, Gomes RS1, Cavalcanti AN2, Mathias P2
1 Piracicaba Dental School, Department of Restorative Dentistry, University of Campinas, Piracicaba, Brazil.
2 School of Dentistry, Department of Clinical Dentistry, Federal University of Bahia, Salvador, Brazil.
3 Piracicaba Dental School, Department of Prosthodontics and Periodontology, University of Campinas, Piracicaba, Brazil.
*Corresponding Author
Caroline Mathias Carvalho de Souza,
Piracicaba Dental School, Department of Restorative Dentistry,
University of Campinas, Piracicaba, 13414-903, Brazil.
Tel: 55 19 99959-3985
Fax: 55 19 2106-5340
E-mail: caroline.mathias@hotmail.com
Received: January 12, 2017; Accepted: February 24, 2017; Published: February 27, 2017
Citation: Carvalho de Souza CM, Vitória LA, Gomes RS, Cavalcanti AN, Mathias P (2017) Influence of Ceramic Laminate Veneer Thickness on Sorption and Solubility of Light-Cured Resin Cement. Int J Dentistry Oral Sci. 4(2), 422-426. doi: dx.doi.org/10.19070/2377-8075-1700084
Copyright: Carvalho de Souza CM© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: This study evaluated the influence of different thicknesses of ceramic laminate veneers on water sorption and solubility of light-cured resin cement.
Materials and Methods: Twenty-four specimens of light-cured resin cement (8 mm diameter and 1 mm thickness) were divided into four groups according to ceramic thickness interposed during cure: without ceramic laminate veneer; 0.7 mm, 1.0 mm and 1.3 mm. All samples were subject to water sorption and solubility process. The mean water sorption and solubility values were compared by One-way ANOVA/Tukey’s test (α = 0.05). Pearson's correlation was performed to identify correlations between water sorption and solubility as well between ceramic thickness and water sorption and solubility.
Results: Significant differences were found in the sorption values (P < 0.05) and solubility (P < 0.01) for the tested conditions. Water sorption and solubility in the cement light-cured under thicker ceramic were statistically higher than control group. Moreover, there was a positive correlation between veneer thickness and water sorption and solubility of the light-cured resin cement.
Conclusion: The variation in the thickness of the ceramic laminate veneer can alter water sorption and solubility properties of the light-cured resin cement tested
2.Introduction
3.Material and Methods
4.Results
5.Discussion
6.Conclusions
7.References
Keywords
Resin Cements; Solubility; Dental Materials.
Introduction
The use of ceramic laminate veneers for restorative and aesthetic treatment has also increased the use of light-cured resin in clinical practice [1-3]. According to several studies, both clinical success and durability of indirect restorations with ceramic laminate veneer are closely related to its fracture resistance and good marginal adaptation [1, 4], which depends directly on restoration adaptation and use of suitable adhesive system and cementation protocol [5-9].
The light-cured resin cements were development to be used under aesthetic restorations which allow for passage of light required for polymerization reaction [2]. Among the advantages of these cements, one can cite good physical and mechanical properties [10] and color stability, especially if compared to self-cured and dual-cured resin cements, which have tertiary amine – a chemical activator causing color changes over time [8, 9, 11, 12]. Despite their advantages, light-cured resin cements also have some disadvantages such as polymerization problems, especially when placed under thick opaque prosthetic restorations, resulting in a cement with poor mechanical strength and limited adhesion [7].
In clinical practice, it is difficult to determine the thickness limit of a ceramic laminate veneer and/or translucency the material should possess to ensure reliable monomer conversion into polymers which make up the resin cement, especially when this conversion depends exclusively on the light energy deposited in the cement [13]. The resin cements can be light-cured under lithium disilicate ceramic restorations of up to 2mm thickness without impairing adhesion [14]. However, studies show that increase inceramic thickness results in lower transmittance of photo-curing light to the cementing agent [15] and, consequently, the resin material presents decrease in hardness and monomer conversion [7]. Moreover, the literature is not conclusive about which thickness variation limit and ceramic translucency would be optimal for proper transmittance of incident light [7, 11].
Incomplete polymerization and subsequent reduction in the degree of monomer conversion, as well as interaction with oral environment, can consistently reduce the longevity of indirect restorations [16]. One of the consequences of this interaction is the absorption of oral liquids and saliva substances by the resin cement [17, 18]. The water can penetrate into the polymer network via porosity and intermolecular spaces, being mainly absorbed in the resin matrix [17, 19]. After this water sorption, the subsequent mechanism is the loss of some resin components, mainly unreacted monomers and filler particles, known as solubility [19].
The traditional ceramic laminate veneers with dental preparations, located mainly in dental enamel [20], have encouraged the continued use of light-cured cements. These preparations result in veneers with thicknesses ranging from 0.5 mm, in the middle third, to 1.3 to 1.5mm, especially in the incisal third [5]. Therefore, in a same preparation, different material thicknesses can be found [4]. In this way, it becomes important to determine whether those small variations of thicknesses are significant to the physical and mechanical features of light-cured cement under ceramic restoration.
Therefore, recognizing the importance of maintaining the cement properties, the aim of this in vitro study was to evaluate water sorption and solubility of the Nexus Third Generation resin cement (NX3, Kerr, Orange, California, USA), light cured under different thickness of ceramic laminate veneers. The null hypotheses are that different thicknesses of laminate veneers do not interfere with the values of water sorption and solubility of the light-cured resin cement studied.
Material and Methods
Three ceramic laminate veneers of 10mm in diameter and three different thicknesses (i.e. 0.7mm; 1.0mm and 1.3mm) were prepared based on lithium disilicate ingots (IPS e.maxPress, Ivoclar- Vivadent, Schaan, Liechtenstein), all having 2M2 color and high translucency (HT).
A polyvinyl siloxane mold (mA)(Aquasil Ultra Putty, Dentsply, York, Pensilvania, EUA) with 1mm thickness and inner hole of 8mm diameter was used for accommodation and preparation of resin cement specimens. Another polyvinyl siloxane mold (mB) was made in order to adapt the ceramic laminate. The function of this device was to avoid light dissipation at the time of polymerization, as well as any interference from external light, during the light curing procedures [21]. The cement was inserted into the polyvinyl siloxane mold (mA) and a polyester strip was placed on it, whereas the second mold (mB) containing the ceramic laminate was placed on the strip. A glass slide was placed on the resulting set to remove the excess material. Next, the cement was photo-activated by using a LED light device (Radii Plus, SDI, Melbourne, Victoria, Australia) at power intensity of 1.500 mW/cm2 for 60 seconds, with the device’s tip touching a single point on the ceramic laminate veneer (except in the control group).
A total of 24 specimens of Nexus Third Generation light-cured cement (NX3, Kerr) in white color were prepared and divided into four groups (n=6) according to the different thicknesses of ceramic laminate veneer, namely: Group I (control), with the cement being light-cured without ceramic laminate veneer, whereas in the other groups the cement was light-cured under ceramic laminate veneer thicknesses of 0.7mm, 1.0mm and 1.3mm.
The specimens were submitted to evaluation of water sorption and solubility according to the ISO specification 4049:2000. Immediately after their preparation, the 24 specimens were placed in a desiccator containing silica gel and transferred for pre-conditioning at 37°C. The thickness of the specimens were measured by using a digital caliper (500-151 Absolute Digimatic Caliper, Mitutoyo, Kawasaki, Japan), and the resulting values were used to calculate the volume (V) of each specimen (mm3), (V = π x r2 x h). All weight measurements were carried out by using an analytical balance (AUD 220D, Shimadzu Corp., Nakagyo-Ku, Kyoto, Japan) with precision of 0.00001g.
The specimens were weighted repeatedly at 24 hours intervals to obtain a constant weight (m1). After mass stabilization of the specimens, they were stored individually in sealed Eppendorf micro-tubes containing 2 mL of distilled water (pH 7.2) at 37ºC, for 7 days. After this period, the specimens were dried with tissue paper and then weighed to establish the amount of water sorption (m2). The specimens were again stored in a desiccator to eliminate any absorbed water before being weighed daily until a constant mass value was obtained (m3). Water sorption (WS) and solubility (Sol) were calculated by using the following formula below:
WS = (m3-m2)/V
Sol = (m1-m3)/V
After exploratory data analysis to verify the homogeneity of variances, the statistical analysis of water sorption and solubility data were performed by using one-way ANOVA and Tukey’s test for multiple comparisons between the averages (SAS system 9.1, SAS Institute Inc, Cary, North Carolina, USA) at 5% significance level. Pearson’s correlation was performed by using the IBM SPSS Statistics 20 (IBM Corp., Armonk, New York, USA).
Results
Table 1 shows the means and standard deviations of water sorption and solubility for the experimental groups. According to statistical analysis, differences were found both in water sorption (P < 0.05) and solubility (P = 0.01) between the four conditions tested.
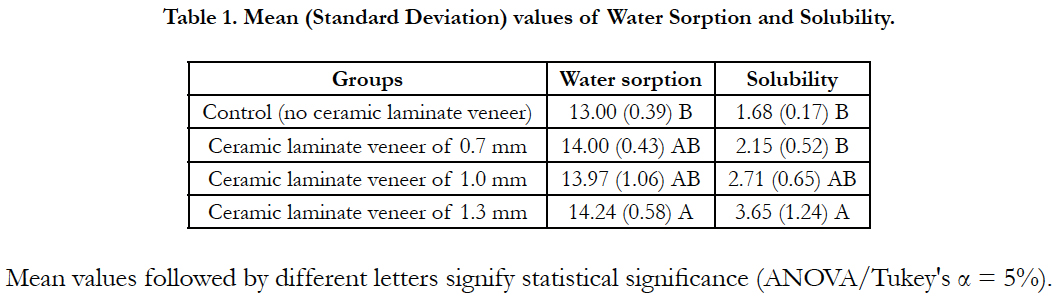

Table 1. Mean (Standard Deviation) values of Water Sorption and Solubility.
For the water sorption data, there were significant differences in the mean values between the group with 1.3mm ceramic laminate veneer and the control group. The other groups showed intermediate values, with no statistically significant differences between them.
For the solubility data, the mean value of the group with 1.3mm ceramic laminate veneer was statistically higher than those of group with 0.7mm ceramic laminate veneer and control group. The group with 1.0mm ceramic laminate veneer presented an intermediate value, which did not differ from the other groups.
Figures 1, 2, and 3 show the Pearson’s correlation analysis, where statistically significant moderate positive correlations between water sorption and solubility (Figure 1) (r = 0.594; P < 0.01), between thickness and water sorption (Figure 2) (r = 0.581; P < 0.01) and between thickness and solubility (Figure 3) (r = 0.678; P < 0.01) were found.
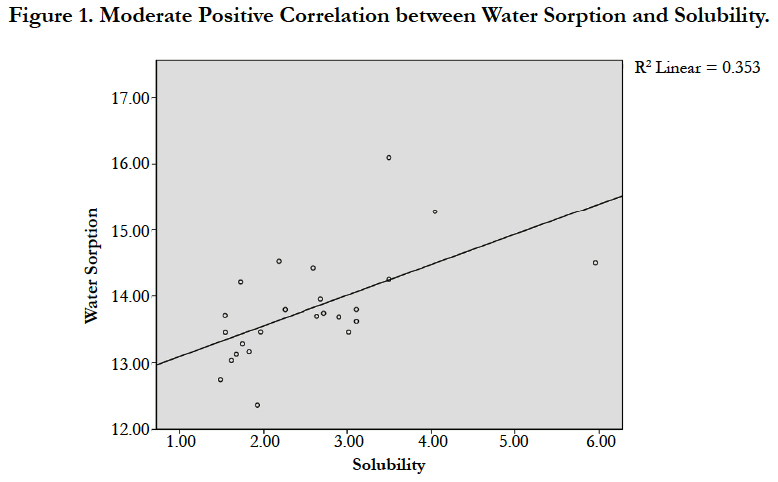
Figure 1. Moderate Positive Correlation between Water Sorption and Solubility.
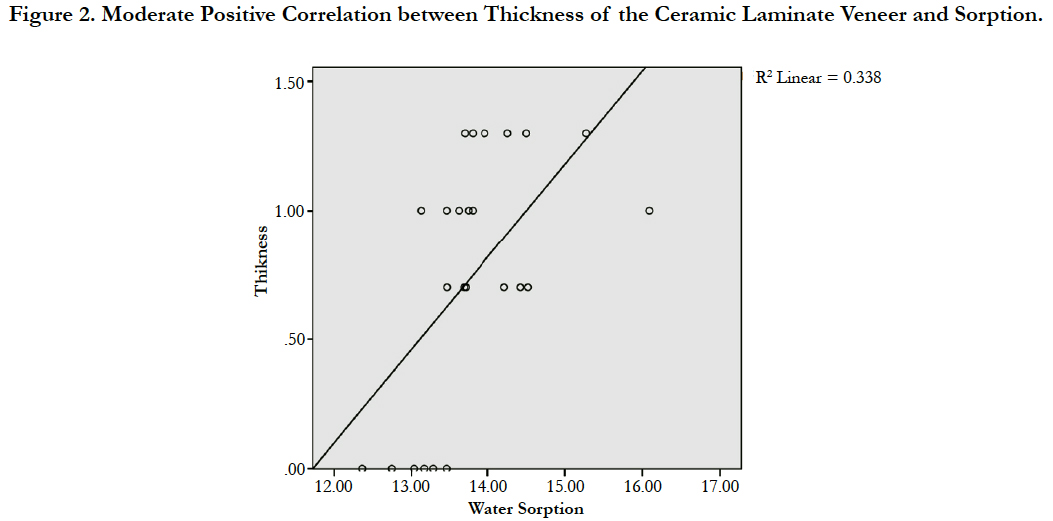
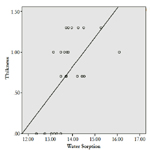
Figure 2. Moderate Positive Correlation between Thickness of the Ceramic Laminate Veneer and Sorption.
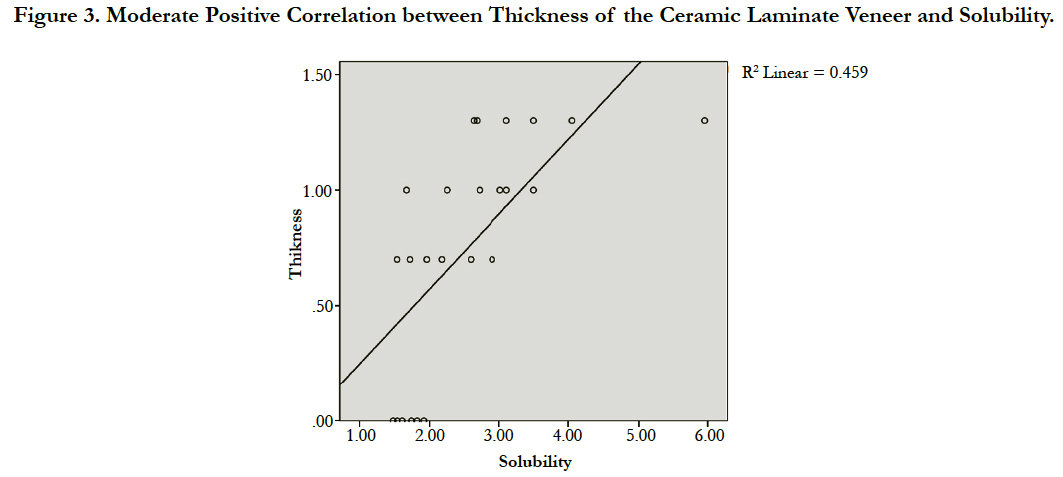
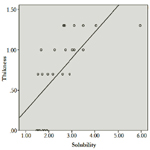
Figure 3. Moderate Positive Correlation between Thickness of the Ceramic Laminate Veneer and Solubility.
Discussion
The null hypothesis has been rejected, since the degree of water sorption and solubility was influenced by the different thicknesses of ceramic laminate veneers. There was a significant difference in water sorption and solubility between the resin cement lightcured under thicker laminate and that light-cured without ceramic laminate positioned between light output and resin material (control group).
When the resin cement was photo-activated under a 1.3mm ceramic laminate veneer thickness, it was found that water sorption was greater compared to the control group. This result can be explained by the fact that the interposition of a ceramic laminate veneer with 1.3mm thickness had reduced the intensity of light energy reaching the resin cement placed under the ceramic piece. The decreased light intensity can reducethe monomer conversion [21], thus increasing the amount of unreacted monomers in the material.
This observation can be confirmed in the control group, where the resin cement was light-cured directly by using an LED device with no ceramic laminate veneer or any other object capable of reducing light transmittance positioned at the tip of the light-curing unit. Lower water sorption was observed in the present study, corroborating the findings by Cho et al., [2], who found a lower degree of conversion when the resin cement was light-cured under a thicker ceramic. The incomplete polymerization of the resin cement results in both low degree of conversion and presence of a larger amount of residual monomers, which may affect physical properties such as water sorption and solubility [2, 22-24]. One of the consequences of water sorption over time is the hydrolytic degradation of the resin cement. This degradation occurs due tothe breakage of the resin cement chemical bonds or softening of the material by the water action [19, 25].
In the groups where the resin cement was light-cured under ceramic laminate veneer thicknesses of 0.7mm and 1.0 mm, intermediate values of water sorption and solubility were observed, probably because the thicknesses of their laminates were insufficient to reduce significantly the light energy available to convert monomers into polymers as in the control group. No change was observed in the dynamic diffusion properties of the resin cement under these different experimental conditions. It is note worthy that the HT ingots tested in this study represents a highly translucent ceramic material. Therefore, the testing of other opaque ceramics should be considered regarding the interference of laminate thickness in each experimental condition.
The incomplete polymerization of the resin cement results in low degree of conversion as well as in large amount of residual monomers (which are leachable) and filler particles, thus increasing the solubility of the material [19, 22]. According to Munksgaard, Peutzfeldt and Asmussen [26], elution of the resin cement components is much higher when the compound is not properly photo-activated, which might explain the significant difference in solubility between 1.3 mm group and control and 0.7 mm groups, since the 1.3mm laminate was configured to be a greater barrier allowing for sufficient transmission of light energy to promote further polymerization of the cement.
The solubility of the light-cured resin cement can influence the dimensional changes, thus compromising its structural stability and biocompatibility. The release of residual monomers into the oral environment can promote restoration misfit [27], bacteria growth at the interface and secondary caries [18, 19], as well as debonding of ceramic laminate veneers [27]. These monomers had not been properly converted because they depend exclusively on light to be polymerized.
According to ADA Standard n° 27 the mean values of water sorption and solubility ranged from 13 to 14.24 mg/mm3 and from 1.68 to 3.65 mg/mm3, respectively, all below the acceptable limits. However, this fact does not mean that the levels of water sorption and solubility found cannot influence the quality and longevity of cementation.
In this study, there was a moderate positive correlation between the values of water sorption and solubility, thus confirming the findings by Cekic-Nagasand and Ergun [23], who evaluated the sorption and solubility of different resin cements photo-activated by several light-curing sources under ceramic disks. Therefore, it can be said that the higher the amount of water absorbed, the greater the amount of components being leached from the resin cement.
The greater the thickness of the ceramic laminate veneer, the lower the degree of monomer conversion in light-cured resin cements, resulting in a larger amount of unreacted monomers [7]. Consequently, there were higher levels of water sorption and solubility in the group where the distance between light-curing source and cementing material was greater, existing a positive correlation of ceramic laminate veneer thickness with both water sorption and solubility.
The chemical structure of the solutions used in in vitro tests is important because it must simulate the oral environment complexity, since the intraoral fluids are probably some of the most aggressive organic solvents [19]. Distilled water is not able to simulate pH variations in oral cavity, so in vitro water sorption and solubility tests are considered static [25]. Thus, the findings in this in vitro study are important, but should be further confirmed by longterm clinical studies [23].
The cementing procedures using ceramic laminate veneers and resin cements include a number of variables which interfere significantly with their results and clinical performance such as type of ceramic, degree of translucency/opacity of the indirect restoration, design of dental preparation and ceramic thickness, adhesive materials and applied cement, type of light-curing source, light application time, dental substrate, among others [1, 2, 7, 12]. All of these variables need to be studied and understood both separately and together to establish protocols for ceramic laminate veneers cementation.
Conclusions
Considering the methodology and results of this study, it can be concluded that variation in the ceramic laminate veneer thickness can influence water sorption and solubility ofthe resin cement. Moreover, there is a positive correlation between thickness of the ceramic laminate veneer and water sorption and solubility of the light-cured resin cement.
References
- Aboushelib MN, Elmahy WA, Ghazy MH (2012) Internal adaptation, marginal accuracy and microleakage of a pressable versus a machinable ceramic laminate veneers. J Dent 40(8): 670-7.
- Cho SH, Lopez A, Berzins DW, Prasad S, Ahn KW (2015) Effect of Different Thicknesses of Pressable Ceramic Veneers on Polymerization of Lightcured and Dual-cured Resin Cements. J Contemp Dent Pract. 16(5): 347-52.
- Sato TP, Anami LC, Melo RM, Valandro LF, Bottino MA (2016) Effects of SurfaceTreatments on the Bond Strength Between Resin Cement and a NewZirconia-reinforced Lithium Silicate Ceramic. Oper Dent. 41(3): 284-92.
- Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G (2010) Porcelain veneers: a review of the literature. J Dent. 28(3): 163-77.
- D'Arcangelo C, De Angelis F, Vadini M, D'Amario M (2012) Clinical evaluation on porcelain laminate veneers bonded with light-cured composite: results upto 7 years. Clin Oral Investig. 16(4): 1071-9.
- Lambade DP, Gundawar SM, Radke UM (2015) Evaluation of adhesive bonding of lithium disilicate ceramic material with duel cured resin luting agents. J Clin Diagn Res. 9(2): ZC01-5.
- Lee JW, Cha HS, Lee JH (2011) Curing efficiency of various resin-based materials polymerized through different ceramic thicknesses and curing time. J Adv Prosthodont. 3(3): 126-31.
- Peumans M, De Munck J, Fieuws S, Lambrechts P, Vanherle G, et al., (2004) A prospective ten-year clinical trial of porcelain veneers. J Adhes Dent. 6(1): 65-76.
- Turgut S, Bagis B (2011) Colour stability of laminate veneers: an in vitro study. J Dent. 39(3): e57-64.
- De Angelis F, Minnoni A, Vitalone LM, Carluccio F, Vadini M, et al., (2011) Bond strength evaluation of three self-adhesive luting systems used for cementing composite and porcelain. Oper Dent. 36(6): 626-34.
- Azer SS, Rosenstiel SF, Seghi RR, Johnston WM (2011) Effect of substrate shades on the color of ceramic laminate veneers. J Prosthet Dent. 106(3):179-83.
- Magalhães AP, Cardoso Pde C, de Souza JB, Fonseca RB, Pires-de-Souza Fde C, et al., (2014) Influence of activation mode of resin cement on the shade of porcelain veneers. J Prosthodont. 23(4): 291-5.
- Lopes LG, Magalhaes AP, Brandao NA, Carvalho AA, Moreira Fdo C, et al., (2012) Effect of light source and solvent on the sorption and solubility of two dual-cured cements photo cured through ceramic. Gen Dent. 60(1): e26-31.
- Akgungor G, Akkayan B, Gaucher H (2005) Influence of ceramic thickness and polymerization mode of a resin luting agent on early bond strength and durability with a lithium disilicate-based ceramic system. J Prosthet Dent. 94(3): 234-41.
- Peixoto RT, Paulinelli VM, Sander HH, Lanza MD, Cury LA, et al., (2007) Light transmission through porcelain. Dent Mater. 23(11): 1363-8.
- Castro FL, Campos BB, Bruno KF, Reges RV (2013) Temperature and curing time affect composite sorption and solubility. J Appl Oral Sci. 21(2): 157-62.
- Anfe TE, Agra CM, Vieira GF (2011) Evaluation of sorption, solubility and staining of universal and silorane resin-based composites. Eur J Prosthodont Restor Dent. 19(4): 151-4.
- Giannini M, Di Francescantonio M, Pacheco RR, Cidreira Boaro LC, Braga RR (2014) Characterization of water sorption, solubility, and roughness of silorane- and methacrylate-based composite resins. Oper Dent. 39(3): 264-72.
- Ferracane JL (2006) Hygroscopic and hydrolytic effects in dental polymer networks. Dent Mater. 22(3): 211-22.
- Öztürk E, Bolay Ş, Hickel R, Ilie N (2013) Shear bond strength of porcelain laminate veneer stoenamel, dentine and enamel- dentine complex bonded with different adhesive luting systems. J Dent. 41(2): 97-105.
- Soares CJ, da Silva NR, Fonseca RB (2006) Influence of the feldspathic ceramic thickness and shade on the microhardness of dual resincement. Oper Dent. 31(3): 384-9.
- Archegas LR, de Menezes Caldas DB, Rached RN, Soares P, Souza EM (2012) Effect of ceramic veneer opacity and exposure time on the polymerization efficiency of resincements. Oper Dent. 37(3): 281-9.
- Cekic-Nagas I, Ergun G (2011) Effect of different light curing methods on mechanical and physical properties of resin-cements polymerized through ceramic discs. J Appl Oral Sci. 19(4): 403-12.
- Di Francescantonio M, Aguiar TR, Arrais CA, Cavalcanti AN, Davanzo CU,et al., (2013) Influence of viscosity and curing mode on degree of conversion of dual-cured resin cements. Eur J Dent. 7(1): 81-5.
- Ortengren U, Andersson F, Elgh U, Terselius B, Karlsson S (2001) Influence of pH and storage time on the sorption and solubility behaviour of three composite resin materials. J Dent. 29(1): 35-41.
- Munksgaard EC, Peutzfeldt A, Asmussen E (2000) Elution of TEGDMA and BisGMA from a resin and a resin composite cured with halogen or plasma light. Eur J Oral Sci. 108(4): 341-5.
- Beier US, Kapferer I, Burtscher D, Dumfahrt H (2012) Clinical performance of porcelain laminate veneers for upto 20 years. Int J Prosthodont. 25(1): 79-85.





