Why is the Aetiology of Facial Bone Fractures in West of Libya is Diffrent
Elarbi M1*, Benjreed I2, Valmores J3
1 Senior Consultant, Chairman of Department Oral & Maxillofacial Surgery, AOA Neurosurgery University hospital, Esbea, Tripoli, Libya.
2 Resident, Department, Oral & Maxillofacial Surgery, AOA Neurosurgery University hospital, Esbea, Tripoli, Libya.
3 Dental Surgeon, Dental Department Service Clinic, Esbea Neurosurgery Hospital, Tripoli, Libya.
*Corresponding Author
Dr. Mohamed Elarbi BDS, M.medSC, FFDRCSI, FICS,
Professor, Senior Consultant,
Chairman of Department Oral & Maxillofacial Surgery,
AOA Neurosurgery University hospital, Esbea, Tripoli, Libya.
Tel: 218913163322
E-mail: mselarbi@hotmail.com
Received: December 24, 2016; Accepted: January 19, 2017; Published: January 23, 2017
Citation: Elarbi M, Benjreed I, Valmores J (2017) Why is the Aetiology of Facial Bone Fractures in West of Libya is Diffrent. Int J Dentistry Oral Sci. 4(1), 405-412.doi: dx.doi.org/10.19070/2377-8075-1700081
Copyright: Elarbi M© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A maxillofacial fracture is a serious clinical problem because of its functional and aesthetic significance. If these injuries are treated improperly may ultimately result in a patient’s low quality of life. Diagnosis and treatment of these fractures remain a challenge for oral and maxillofacial surgeons, demanding a high level of proficiency. Objective: This study aims to analyze the epidemiology of maxillofacial fractures treated in ministry hospital, Ali Omar Askar Neuro Center in Sbea Tripoli, Libya, to identify the causative factors, and to help in planning
programs to control the incident in a population.
Study Design: A retrospective review of all patients with maxillofacial fracture presented to Oral & Maxillofacial Surgery Department of Ali Omar Askar Neuro Center Sbea, Tripoli between January 2010 and December 2015 was performed.
Result: Total of 437 patients obtained 752 maxillofacial fractures. Male were mostly affected comprising 83%, with the majority occurring in individuals 21-30 year age range. Road traffic accident was the most common cause of maxillofacial fractures with a total of 63.84%. Mandible fracture was mostly affected consisting 59.18% of all maxillofacial fractures. The most fractured anatomical part of the mandible is parasymphysis containing 23% of all mandible fractures. Open reduction and internal fixation was the most common treatment modality. Thirteen percent of patients had associated injuries, and four percent had complications.
Conclusion: According to the World Health Organization established in May 2014, Libya is the leading country of traffic deaths per capita. This retrospective study of maxillofacial fracture is congruent to the research that road traffic accident in the country was the most common incident. It is capturing to both government officials to implement legislation and healthcare providers to develop programs to educate the public and reduce such injuries.
2.Materials and Methods
3.Results
4.Discussion
5.Conclusion
6.References
Introduction
Maxillofacial fracture is referred to as any physical trauma to the face involving the soft tissue injuries and fracture to the facial bones as well as eye injuries. Facial injuries may severely affect the essential functions of one’s daily life in breathing, eating, talking, sight, and smell. Thus, surgical expertise is required to treat complicated cases to make use of these significant senses.
Maxillofacial injuries in isolation or in combination with other injuries account for a significant percentage of emergency room and hospital admissions [1,2]. Apparently, regional variation in the incidence, age and gender distributions, cause, site of maxillofacial fractures, and distribution of treatment modalities is influenced by the geographic conditions, cultural characteristics, and socioeconomic trends [2-4]. It has been shown in several studies of maxillofacial trauma that injuries of the maxillofacial region are less common in children than in adults. Also, studies have shown that injuries tend to be, in general, less severe in young children than in older children [5, 6].
Various factors cause maxillofacial fractures such as road traffic accidents, physical assault, accidental falls, gunshot wounds, sports injuries, animal-related injuries and other cause of injuries. Therefore, the mechanism of injury is inconsistent in the literature. Road traffic accidents cause 15% of facial injuries in developed countries, while greater than 50%of injuries to developing nations with a more chaotic system of road use [1,7].
For some authors the introduction of safety devices, including compulsory use of seat belts, air bags and side protection bars begin to reduce if not the rates, at least the complexity of facial fractures [8]. Convington et al., (1994) show that seat belt adoption in the USA reduced the incidence of multiple facial fractures, particularly zygomatic bone fractures, from 46.3% and 80.6% to 20.1% and 50% [8-10].
Literature shows that the most commonly fractured facial bones are mandible, nasal, and maxilla or zygoma. Nasal and maxillary fractures are more common among infants, and mandible fractures are more common among teenagers [11].
The diagnosis of facial fractures often includes conventional radiographs of the face usually followed by a CT scan to assess possible neurological complications and to diagnose complex fractures of the face and skull [12]. It has been generally accepted that stable, undisplaced or asymptomatic fractures are indications for non-operative treatment, but there is no evidence in peer reviewed journals to show whether long-term follow-up supports this view [13].
The aim of this study is to analyze retrospectively the age and gender distribution, mechanism of injury, distribution of anatomical site of maxillofacial fractures, treatment procedures done, associated injuries, and presence of complication among patients treated in Ali Omar Askar Neuro Center in Sbea, Tripoli during January 2010 to December 2015. We therefore provide statistical analysis with necessary figures and data that may eventually influence legislative changes to reduce such injuries.
Materials and Methods
This is a retrospective study on 437 male and female patients admitted in Oral & Maxillofacial Surgery Department at Ali Omar Askar Neuro Center in Sbea, Tripoli from January 2010 to December 2015 treated for maxillofacial fractures whose medical histories were recorded in official hospital charts. The study includes the retrieval of different patient’s data using Microsoft Excel in terms of their age, gender, date of injury, cause, anatomical regions of fracture, treatment modalities, associated injuries and complication if present on each maxillofacial case. The department is still in the process of acquiring suitable software hence all calculations and tabulations have been done manually.
The study was divided into eight age groups: 10 years below, 11-20, 21-30, 31-40, 41-50, 51-60, 61-70, and 71 and above. The youngest patient was 7 months old and eldest 84 years old.
The cause of injury was distributed into the following: road traffic accident, assault, falls, gunshot injury, sports, animal-related injury, and other cause of injuries, like post tooth extraction and occupational.
Maxillofacial fractures were classified according to specific anatomical sites: mandible, maxilla, zygomatic-orbital complex, isolated zygomatic bone, isolated orbital bone, nasoethmoidal complex, isolated nasal bone, frontal bone, and fronto-orbital bone. The mandible fractures were documented into eight anatomical sub sites: symphysis, parasymphysis, body, angle, ramus, condyle, coronoid process and dentoalveolar. Maxillary fractures were distributed into Le Fort I, Le Fort II, Le Fort III, dentoalveolar, and maxillary sinus and split palate. Each fracture line was counted separately. The number of fractures per site according to mechanism of injury was tabulated.
Treatment modalities were categorized into open reduction and internal fixation, intermaxillary fixation, conservative treatment, and left against medical advice (patients would refer to go other country, or private clinics). Facial fractures with associated injuries were recorded as well as complications if any.
Results
A total of 437 patients were treated for maxillofacial fractures during the study period. The patient’s age ranged from 7-month to 84 years old with mean age of 26.3 years. There were 362 male (83%) and 75 female (17%), corresponding to 4.8:1 male-to-female ratio. The highest incidence of maxillofacial fractures for both male and female patients occurred between 21-30 years old. See Figure 1.
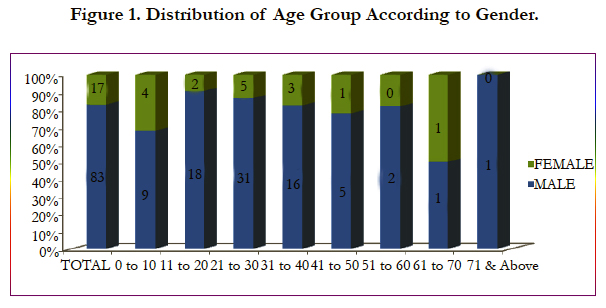
Figure 1. Distribution of Age Group According to Gender.
Road traffic accident was the main cause of maxillofacial fractures for both men and women accounting for 63.84% as shown in Figure 2. Secondary cause of fractures in this study obtained equal rate of incidence both physical assault and accidental falls acquiring 12% (54 patients each cause of injury). Only they vary in some other factor, likeage group in which assault mostly occurred in 21-30 years (mainly 24 male patients) while falls occurred most in 0-10 age group (17 patients), as presented in Table 1. Besides accidental falls, children at age range of 0-10 were mostly affected by kick of horse/camel acquired 0.92% (4 patients) compared to 21-30 and 31-40 with 0.46% (2 patients) in each age group. Gunshot wounds were the third most frequent cause of fractures in 7.09% (31 patients), followed by animal-related injuries like kick by horse/camel 2.06% (9 patients), other cause of injury such as post extraction of molar tooth and occupational were 1.60% (7 patients) and sports injuries 1% (3 patients).
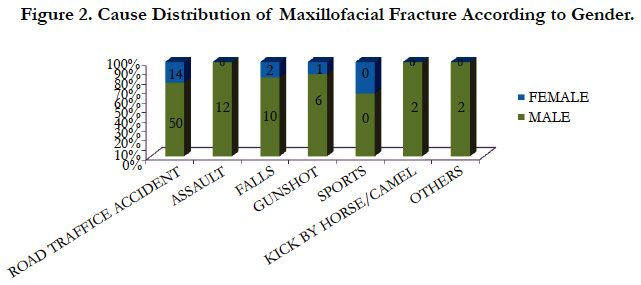

Figure 2. Cause Distribution of Maxillofacial Fracture According to Gender.
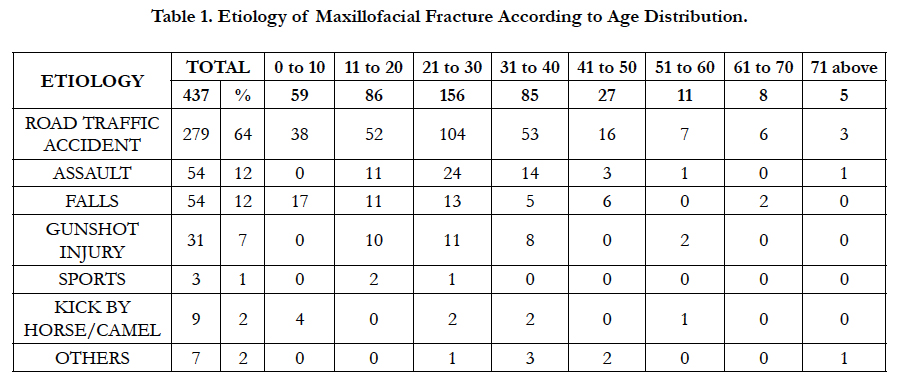

Table 1. Etiology of Maxillofacial Fracture According to Age Distribution.
Overall, a total of 752 maxillofacial fractures were noted, shown in Figure 3. The most commonly fractured anatomical site was mandible 59.18% (445 fractures), followed by zygomatic-orbital complex 15.69% (118 fractures), maxilla 10.90 % (82 fractures), isolated orbital bone 3.46% (26 fractures), isolated zygomatic bone 2.93% (22 fractures), nasoethmoidal complex 2.79% (21 fractures), isolated frontal bone 2.53% (19 fractures), isolated nasal bone 1.99% (15 fractures) and fronto-orbital complex 0.53% (4 fractures).
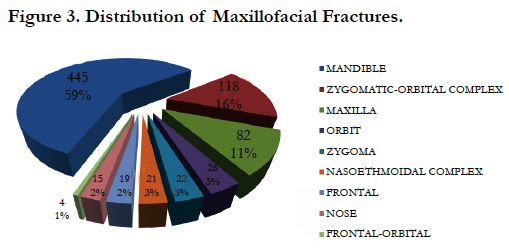
Figure 3. Distribution of Maxillofacial Fractures.
The total of 445 mandible fractures was found amongst 282 patients, almost 1.6 fractures per mandible. See Figure 4. The most commonly involved site of mandible fracture was parasymphysis (103, 23%), followed by angle (96, 22%); condyle (94, 21%), symphysis (67, 15%), body (46, 10%), dentoalveolar (17, 4%), and the least common were ramus and coronoid process with equal distribution (11, 2%) for both. This study revealed that mandible is primarily affected in all mechanisms of injury, as shown in Table 2.
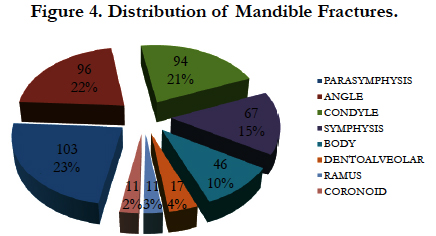
Figure 4. Distribution of Mandible Fractures.
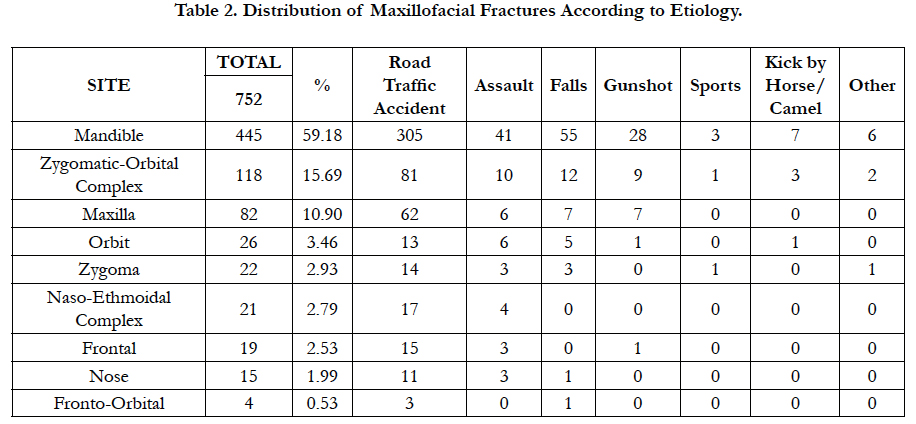
Table 2. Distribution of Maxillofacial Fractures According to Etiology.
There were 57 patients obtaining 82 maxillary fractures, as shown in Figure 5. The most common site of maxillary fracture was found to be Le Fort II (36, 44%). The maxillary dentoalveolar, Le Fort I, and Le Fort III had frequency distributions of 23%, 16%, and 12% respectively. The least commonly affected sites revealed in this study were maxillary sinus and split palate being seen in 2 patients on every site.
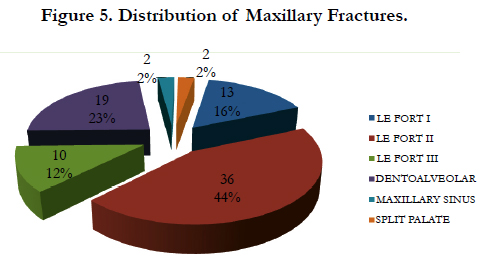
Figure 5. Distribution of Maxillary Fractures.
Of the total number of maxillofacial fractures, 223 patients (51.03%) had only simple fracture, while 140 patients (32.04%) had double fractures and 74 patients (16.93%) had multiple facial fractures. Road traffic accident was the most common mechanism of injury that causes simple, double or multiple fractures in 56%, 64%, and 88% respectively. See Figure 6.
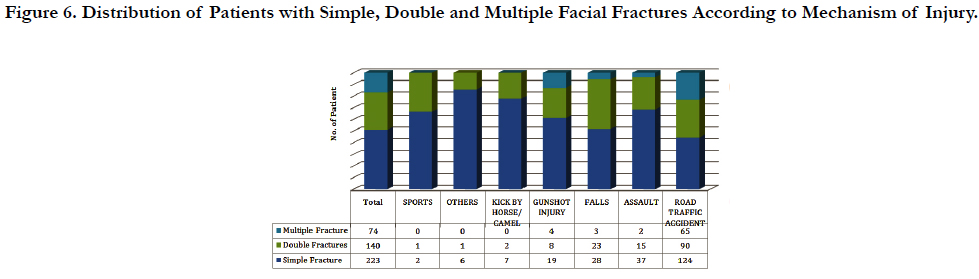
Figure 6. Distribution of Patients with Simple, Double and Multiple Facial Fractures According to Mechanism of Injury.
The annual distribution of maxillofacial fracture peaked in 2013, as shown in Figure 7. On that year appeared the terrorist attacks in several incidents by the violent extremist groups, undermining the fragile democratic transition government of the country. Table 3 below displays the annual injuries in various mechanism of injury. The peak of gunshot injuries showed 19 patients (61.29%) on 2011, the beginning of Libya civil war. Annual incidence of gunshot was presented since 2011 to 2015 because of the availability of firearms to almost every Libyan household in spite the gun control policy has been enforced. No recorded incident on 2010 where civilian gun ownership was rare since decades.
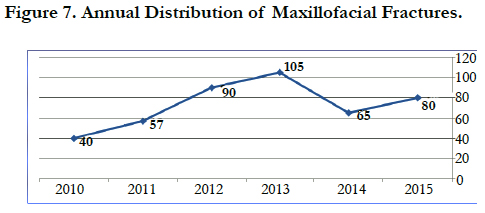

Figure 7. Annual Distribution of Maxillofacial Fractures.
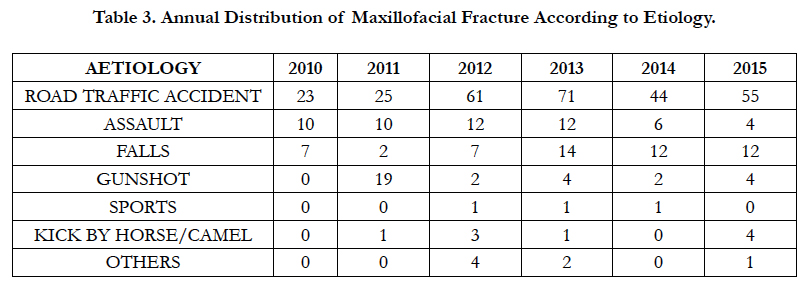
Table 3. Annual Distribution of Maxillofacial Fracture According to Etiology.
Regarding treatment modalities in this study, Open Reduction and Internal Fixation treated most of the patientsin 309 patients (71%). Seventy eight patients (18%) were treated conservatively, thirty three patients (8%) left against medical advice that would refer to seek treatment in private clinic or to another country, and seventeen patients (4%) were managed by intermaxillary fixation, shown in Figure 8.
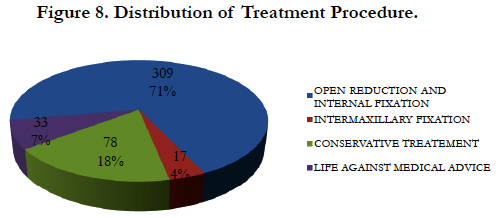

Figure 8. Distribution of Treatment Procedure.
Associated injuries were present in 46 patients (11%) of all maxillofacial fractures, given in Figure 9. Of these cases, 20 patients (4.58%) had skull injuries (brain edema, contusion, skull fracture), followed by fracture of lower extremity in 12 patients (2.75%), chest injury 11 patients (2.52%), fracture of upper extremity 10 patients (2.29%), and spine injury 2 patients (0.46%).
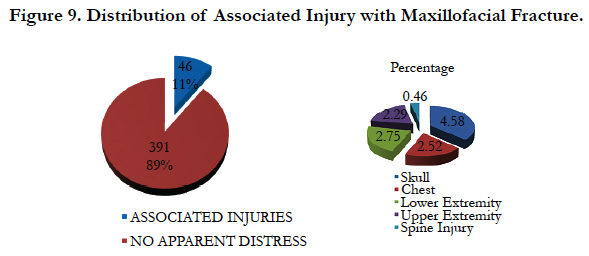
Figure 9. Distribution of Associated Injury with Maxillofacial Fracture.
Complications were noticed in 4% (19 patients) of the total maxillofacial fractures in the form of transient facial weaknessin 10 patients (2.29%); wound dehiscence in 4 patients (0.92%), malocclusion in 3 patients (0.69%) and defect of palate in 2 patients (0.46%), which were managed satisfactorily. See Figure 10.
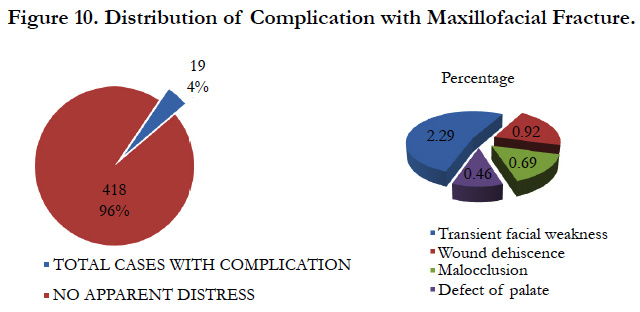

Figure 10. Distribution of Complication with Maxillofacial Fracture.
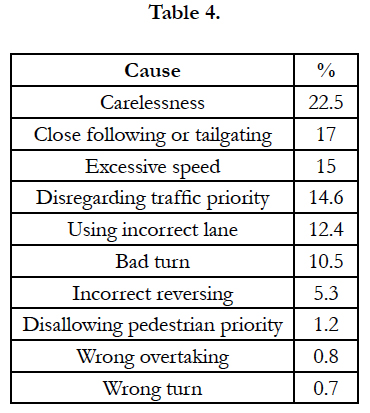


Image A. Shows Clinical presentation of maxillofacial injuries.
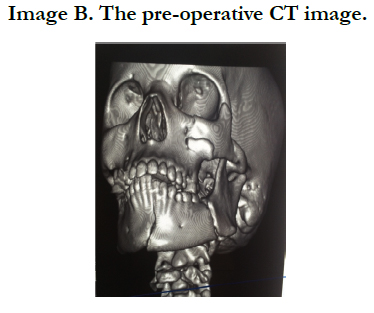

Image B. The pre-operative CT image.
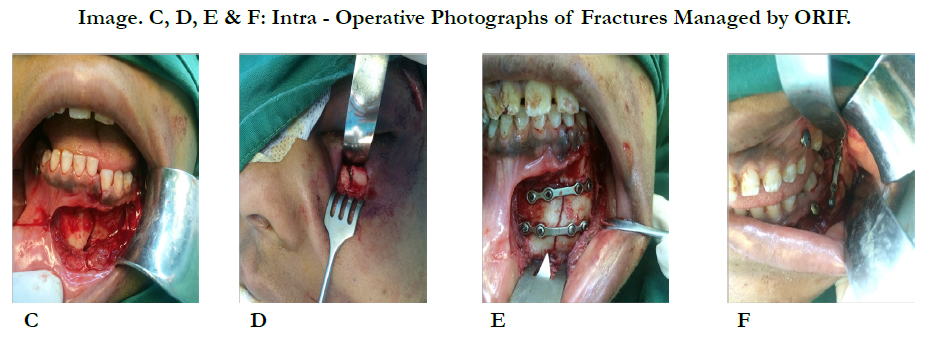

Image. C, D, E & F: Intra - Operative Photographs of Fractures Managed by ORIF.

Image G. Shows post-operative CT image..
Discussion
Maxillofacial injury remains a challenge for oral and maxillofacial surgeons demanding both skill and high level of proficiency. In our institution, a total of 437 patients constituted 752 maxillofacial fractures were treated from 2010 to 2015.
The study of maxillofacial fractures has been reported in literature and they differ from country to country and the statistics is clear that some of the inconsistencies can be attributed by social, cultural, and environmental factors [2-4].
The predominance of facial injuries of the male population is a relatively consistent finding in other studies. This study found 83% male and 17% female giving a male-to-female ratio of 4.8:1 which is similar to those reported literature [7, 8, 14]. Men in the country actively participated during the state of conflict and mostly involved in other outdoor activities. Furthermore, men are actually more risky in driving practices, like not using safety belts, driving at high speed and frequently under alcohol consumption. On a contrary, recent literature shows a trend toward a more equal male-to-female ratio due to social engagements of women [14]. Maxillofacial fractures are more common in young adults particularly in age range 21 to 30 (31%) which is similar to other studies [8, 15,16]. The people in these age group are the most active, making them vulnerable to trauma.
World Health Organization in 2013 has reported that Libya is the leading country of fatality rate as a result of road traffic accident. Recent data support the difference in the etiology of maxillofacial injuries in various nations. The developing countries found road traffic accident as the leading cause of facial fractures. However, in developed countries, interpersonal violence is the major cause of injuries. The differences may relate to speeding and lack of legislation in the developing countries. On the other hand, alcoholism appears to be a major factor responsible for assault and interpersonal violence in developed countries [14,15].
Libya is a conservative Arab developing country where alcohol is prohibited, yet it is relatively accessible to young men drinking in their cars at night, or celebrating parties in farm where alcohol is available. Drunken men may cause lower incidence of causative assault in the society, but another factor of road traffic accident instead. This study have not recorded alcohol consumption that was related to the cause of fracture because of some reasons, including patient reporting and patient history recording by the doctors. Likewise, some patients arrived unconscious, intubated, or late after the injury.
Fall from height is another cause of facial bone fractures in this study mainly at home when men traditionally do maintanance without following safety instructions and using primitive equipments and tools, also falls from roof of houses, in childrens falls from stairs or high wall, trees as usually many boys and girls due to lack of supervison by mothers as she busy with something else!! as in typical libyan families gathering especially in weddings and death of family members which last minimum three continous days.
Another common cause of fall due to improperly designed bavements construction as many cases reported as fall in holes beside the road or in poorly maintained pavements.
Several reasons of road traffic accidents in the country are attributed by many young reckless drivers ignoring traffic regulations in the absence of traffic police to enforce them. In 2011 A. Ismael, H.A.M. Yahia [16] noted the main reasons for traffic accidents in Libya (2007-2010):
Also there are cases reported in this study RTA when driver lost control of his car as he is busy using mobile phone or texting massage!!
The driving licence easialy obtined without passing real driving test!! That’s why most of the young drivers know littile or nothing about law of driving and serious consequences follow.
Therefore this study shows the most common cause of maxillofacial fracture, road traffic accidents for both men and women. The government and health sectors in the country need to enforce traffic rules and regulations and to ensure speedy implementation to reduce such accident. Assault and accidental falls was the second most common cause accounting both 12% of the total injuries. Those suffering injuries caused by assault were mainly male and mostly affected age group of 21-30 years, while female reported accidental falls as the second most frequent reason for their injuries. Injuries to children at age 0-10 are mainly caused by falls and animal-related injury. The childrenare curious and adventurous not aware of the consequences of the situation leading them in danger. Gunshot injury become the third most commonly cause of maxillofacial fracture. During the Libyan unrest on 2011, vast majority of young adult were involved in war injuries. Kick by horse or camel, sports and other cause of injury were least common in this study.
With regard to the maxillofacial fractures, the most commonly involved bones were the mandible, followed by zygomatic-orbital complex. These reports are consistent with some other literatures [4,7, 8] but differ in other study from South Korea [17] that denotes nasal bone as the most fractured site followed by the mandible.
Determination of the location and type of fracture beside to the fixation of the associated structures affected by the fracture is very important in the determination of the treatment modality. Treatment of maxillofacial fractures can range from conservative to definitive surgical approach. Open reduction and internal fixation has emerged as the management tool in this study using titanium micro/mini plates and reconstruction plates. The rationale of this approach is to obtain best exposure and to provide optimal function and aesthetics.
Conclusion
This retrospective study shows the high frequency distribution of road traffic accident that remains to be the main etiological factor of maxillofacial fractures. Government officials should take serious measures to reduce road accidents, such as strict and comprehensive laws in driving, speeding, seat-belts, speed limits, speed camera and road maintainance.
National campaign in schools and public to educate people how to reduce these injuries is very important.
Fall from highet at home can be prevented by educating people to waer safety helmet and use proper tools and safety instructions.
Assaults can be reduced by education, strict law and study underlying causes such as unemployment and violence in youngester.
Furthermore, we need software program to improve data collection that will be helpful in conducting further research, which involve epidemiology of maxillofacial trauma that can be used as frameworks in establishing clinical and research protocols, so as to treat and prevent such injuries.
References
- Firras N, Samir T, Ismael F (2013) Pattern of traumatic maxillofacial injuries among the young adult Qatari population during the years 2006-2009. A retrospective study. Egyptian J Ear Nose Throat Allied Sci.ens. 14: 11-15.
- Anna K, Elisabeth A, Robert S, Clemens Z, Florian P, et al., (2012) Craniomaxillofacial Trauma: Synopsis of 14,654 Cases with 35,129 Injuries in 15 Years. Craniomaxillofacial Trauma Reconstr. 5(1): 41-50. doi: 10.1055/s-0031-1293520.
- Bormann KH, Wild S, Gellrich NC, Kokemuller H, Stuhmer C, et al., (2009) Five-year retrospective study of mandibular fractures in Freiburg, Germany: incidence, etiology, treatment, and complications. J Oral Maxillofac Surg. 67(6): 1251-5. doi: 10.1016/j.joms.2008.09.022.
- Giuliano A, Francisca C, Michele C, Paolo M, Claudio C (2014) Maxillofacial Fractures in the Province of Pescara, Italy: A Retrospective Study. ISRN Otolarngology. 2014: 101370. doi: 10.1155/2014/101370.
- Zarina S, Stephen W (2002) Epidemiology of facial trauma in a sample of patients aged 1-18 years. Injury. 33(8): 669-671.
- Haug RH, Foss J (2000) Maxillfacial injuries in the pediatric patient. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 90(2): 126-34.
- Ashfaq A, Waseem A, Syed G, Omer S, Uzair L, et al., (2012) The Maxillofacial Trauma Management Trends at Armed Forces Institute of Dentistry, Rawalpindi. Pakistan Oral & Dental J. 32(2): 191- 195.
- Jair M, Ligia Maria C, Marina G, Vinicius M, Fabricio F, et al., (2006) Etiology and Incidence Facial Fractures in Children and Adults: experience in 513 cases. Rev Bras Otorrinolaringol. 72(2): 235-41. doi: 10.1590/S0034-72992006000200014.
- Jose M, Frederico K, Ernani SH (2010) Epidemiological Characteristics of Trauma Patients Maxillofacial Surgery at the Hospital Geral de Blumenau SC From 2004 to 2009. Thieme publ. 14(02):192-198. DOI: 10.7162/S1809-48722010000200008.
- Convington DS, Wainwright DJ, Teichgraeber JF, Parks DH (1994) Changing patterns in the epidemiology and treatment of zygoma fractures: 10-year review. J Trauma. 37(2): 243-8.
- Imahara SD, Hopper RA, Wang J, Rivara FP, Klein MB (2008) Patterns and outcomes of pediatric facial fractures in the United States: a survey of the National Trauma Data Bank. J Am Coll Surg. 207(5): 710-6. doi: 10.1016/j.jamcollsurg.2008.06.333.
- Khan SU, Khan M, Khan AA, Murtaza B, Maqsood A, et al., (2007) Etiology and pattern of maxillofacial injuries in the Armed Forces of Pakistan. J Coll Physicians Surg Pak. 17(2): 94-7.
- Back CP, McLean NR, Anderson PJ, David DJ (2007) The conservative management of facial fractures: indications and outcomes. J Plast Reconstr Aesthet Surg. 60(2): 146-51.
- Marker P, Nielsen A, Bastian HL (2000) Fractures of the mandibular condyle. Part 1: patterns of distribution of types and causes of fractures in 348 patients. Br J Oral Maxillofac Surg. 38(5): 417-21.
- Akinbami BO, Akadiri OA, Udeavor S, Obiechina AE (2013) Pattern, severity, and management of craniomaxillofacial soft-tissue injuries in Port Harcourt, Nigeria. J Emerg Trauma Shock. 6(4): 235-240. doi: 10.4103/0974-2700.120362.
- Amiruddin I, Hussin AMY Causes and effect of road traffic accidents in Tripoli- Libya. Proceeding the 6th Civil Engineering Conference in Asia Region: Embracing the Future through Sustainability.
- Kun H, Sun HY (2010) Analysis of facial bone fractures: An 11-year study of 2,094 patients. Indian J Plast Surg. 43(1): 42-48. doi: 10.4103/0970-0358.63959.





