The Contribution of Pre-Prosthetic Periodontal Surgery in the Success of Anterior Fixed Prostheses
Hajjaji S*, Taktak R, Hajjami H, Boughzella A
Dental Medicine Department, CHU Farhat Hached Sousse, Tunisia.
*Corresponding Author
Dr. Sihem Hajjaji,
Univeristy Assistant in Fixed Prosthodontics,
Department of Dental Medicine,
Farhat Hached Univeristy Hospital, Sousse, Tunisia.
Tel: 55020234
Fax: 73502749
E-mail: sihemhajjaji@gmail.com
Received: December 05, 2016; Accepted: January 16, 2017; Published: January 19, 2017
Citation: Hajjaji S, Taktak R, Hajjami H, Boughzella A (2017) The Contribution of Pre-Prosthetic Periodontal Surgery in the Success of Anterior Fixed Prostheses. Int J Dentistry Oral Sci. 4(1), 401-404. doi: dx.doi.org/10.19070/2377-8075-1700080
Copyright: Hajjaji S© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Pre-prosthetic periodontal surgery plays a major role in the aesthetic and functional integration of prosthetic restorations, especially in the anterior area. Indeed, any dento-gingival disharmony of volume or form must be corrected before hand, thus justifying the use of plastic periodontal surgery.
Clinical Report: A 20-year-old patient consulted our department primarily for an aesthetic reason: the restoration of the fractured 11. The clinical examination revealed the presence of a defective temporary prosthesis on the 11, an aesthetically disturbing composite resin on the 21, an asymmetry of the gingival contour, and a lower labial frenum. A juxta-osseous dilapidation of the lingual wall of the 11 was well demarcated on the Periapical examination.
Discussion: In order to meet the growing aesthetic demand of the patient, a multidisciplinary management was planned: A gingivectomy was thus carried out, in order to align tooth 11 with 21, associated with a Coronal extension of the biological space on the lingual side of the 11. To optimize the final therapeutic result, a superior labial frenectomy was performed.
2.Introduction
3.Clinical Report
4.Discussion
5.Conclusions
6.References
Keywords
Coronary Elongation; Periodontal Surgery; Biological Space; Aesthetics; Gingivectomy.
Introduction
The aesthetic integration of prostheses fixed in the anterior area is ensured by a harmonious cohabitation between the prosthetic elements and the periodontium. To optimize final therapeutic success, a compromise is often sought between the desired aesthetic result and biology. For this, periodontal adjustments are sometimes necessary. Therefore, prior and precise screening of the periodontium is systematic [1].
Our work aims to highlight, through a clinical case, the role of pre-prosthetic periodontal surgery in the aesthetic success of a prosthetic restoration fixed at the level of the anterior sector.
Clinical Report
A young patient, aged 20, consulted our department for an essentially aesthetic reason: the restoration of the 11.
The patient expressed great dissatisfaction with the aesthetic aspect of her smile and wished for a global care (not only at the 11th level), allowing her to overcome her aesthetic "handicap". In view of these requirements, a rigorous clinical and radiographic study of the teeth and the periodontium was carried out.
Initial clinical examination revealed sufficient oral hygiene, however, with the presence of localized gingival inflammation with respect to the 11th. The thorough examination of the endobuccal confirmed the patient's concerns about the asymmetry of the gingival contour of the two central incisors, with a lower upper labial frenum (Figure 1).
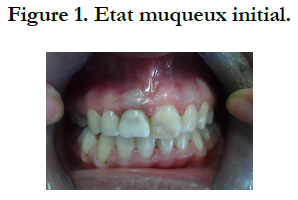

Figure 1. Etat muqueux initial.
The dental examination revealed a defective restoration by the composite resin on the 21, as well as a provisional root crown on the 11 (Figure. 2). Examination of this prosthesis revealed an inadequate morphology with a vestibular overhang, a mesio-distal diameter greater than that of the 21, narrow gingival embrasures compressing the inter-dental papillae (which also explains the gingival inflammation at this level), as well as a lower height than that of the 21.
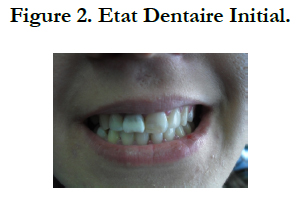

Figure 2. Etat Dentaire Initial.
After removing the temporary crown, careful examination of the 11 revealed an important decay which compromised more than half the coronary height, with a lingual wall almost absent (Figure 3).
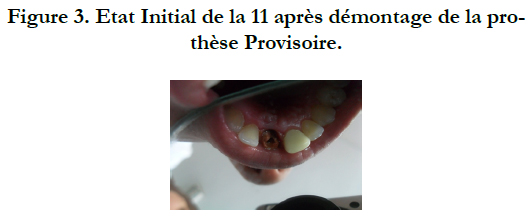

Figure 3. Etat Initial de la 11 apres demontage de la prothese Provisoire.
Radiological examination revealed a defective root canal restoration at the level of the 11 with the presence of a periapical radiolucent image. The root anchorage of the temporary prosthesis was very low in the root. The lingual residual wall was juxta-osseous, which will already compromise the realization of a prosthesis respecting the integrity of the periodontium (violation of the biological space). However, the length and shape of the root were considered favorable for the preservation of the tooth (ratio CR / RR < 1) (Figure 4).
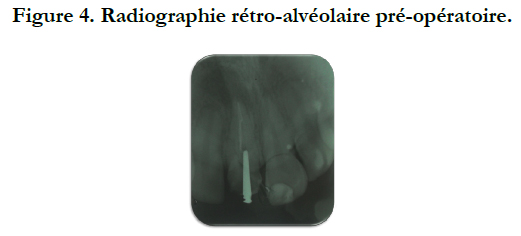
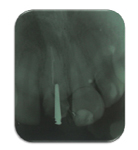
Figure 4. Radiographie retro-alveolaire pre-operatoire.
The prosthetic decision was therefore the realization of two ceramic-ceramic crowns respectively on the 11 and the 21. For this, we started with the making of the wax up whose objective was to visualize the prosthetic project as a whole (Figure 5).
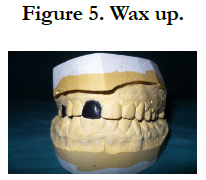

Figure 5. Wax up.
The patient agreed on the treatment plan, which enabled us to begin the pre-prosthetic development phase. For this, we began by resuming the endodontic treatment on the 11 to improve the canal obturation (Figure 6). Subsequently, we began the surgical phase aiming firstly on the biological space on the lingual surface of the 11 (Figure 7), and on the other hand, the alignment of the crown of this tooth with that of the 21 (Figure 8); The objective being to obtain an aesthetic prosthesis and respecting periodontal health.
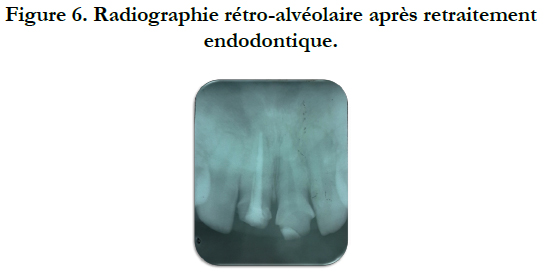
Figure 6. Radiographie retro-alveolaire après retraitement endodontique.
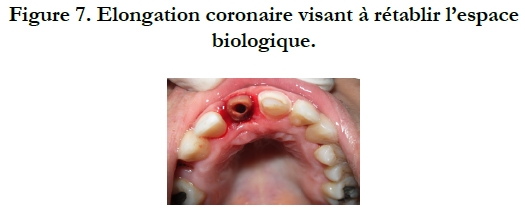

Figure 7. Elongation coronaire visant a retablir l'espace biologique.


Figure 8. Gingivectomie.
In order to maintain the result obtained on the one hand and to guide the healing on the other hand, a provisional cured resin prosthesis was made on the 11 and 21 respectively (Figures 9a, 9b).
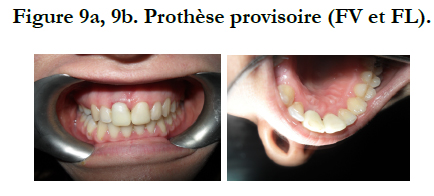

Figure 9a, 9b. Prothèse provisoire (FV et FL).
A first check was made one week after surgery; we noticed a good healing of the gingival contour of the 11, with no inflammation or pain. The aesthetic appearance is greatly improved with the alignment of the crown of the 11 with that of the 21. (Figure 10).
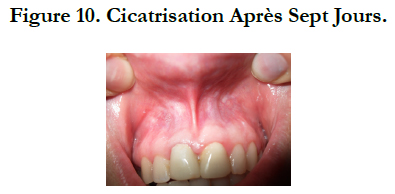

Figure 10. Cicatrisation Après Sept Jours.
At this stage, it was essential to guarantee the stability of the result obtained and to prevent any change in the levels of the crowns by the traction of the upper labial frenum. For this a frenectomy was performed (Figure 11).
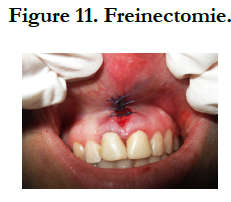

Figure 11. Freinectomie.
Seven days after, the stitches were removed: the condition of the periodontium was stable with good healing (Figure 12). These parameters allowed us to proceed to the realization of the prosthesis itself. For this, we began by reconstructing the fiber 11 (Figure 13).


Figure 12. Cicatrisation apres sept jours.


Figure 13. Reconstitution fibrée de la 11.
All the steps of the conventional prosthetic chain were subsequently rigorously observed until the two ceramic-ceramic crowns of zirconia were placed on the 11 and 21 (Figure 14).
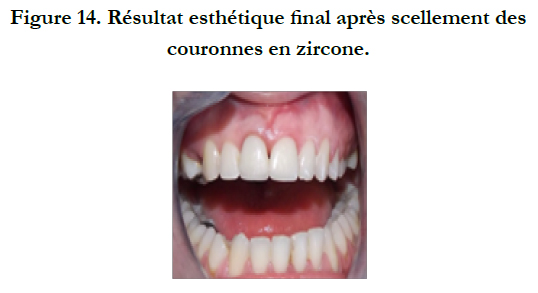

Figure 14. Resultat esthetique final apres scellement des couronnes en zircone.
The patient was very satisfied with the final aesthetic outcome.
Discussion
In fixed prosthodontics, the search for the aesthetic or more precisely the "natural" must take into account a large number of factors and call upon a succession of multidisciplinary treatments, which constitutes the major element of success. The essential purpose is to provide the patient with a functional and aesthetic prosthesis in accordance with his requirements and carried out according to a protocol assuming all the consequences [2-4].
The diagnostic elements, the attached gingiva, the biological space and the alignment of the collars, must be analyzed during a careful preoperative clinical and radiographic examination in order to guide the simplest and best periodontal therapy. These elements are essential because they will allow to analyze the possibilities offered by the periodontium, to solve the various problems, to discuss the probable prosthetic decisions and to consider if necessary techniques of pre-prosthetic tissue development allowing the improvement of the gingival situation [5-10].
In the previously described case, the pre-prosthetic periodontal fitting was necessary in order to obtain an aesthetic prosthesis conforming to the expectations of the patient. Indeed, in view of the asymmetry marked by the displacement of the gingival edges, the too low insertion of the upper labial frenum, as well as the dental decay compromising the integrity of the biological space, it was impossible to carry out the prosthetic implantation without the correction of these "anomalies" in order to restore to the periodontium an anatomy adapted to its function, with a view to the elaboration of prosthetic elements with a perfect biological and functional integration. For this purpose the following interventions were carried out respectively:
The coronary elongation to recreate the biological space following the major coronary destruction on the lingual surface of the 11th. This intervention resulted from the evaluation, on the periapical radiography, of the distance between the limit of the healthy residual dental tissue and the top of the bone crest: the pre-prosthetic surgical space. This space was almost equal to 3 millimeters, which justified the use of this surgical intervention (without touching the level of the bone crest [3, 5, 11-14].
Gingivectomy, which is probably the oldest surgical technique in periodontal surgery. Its aim is to eliminate the gingival tissue in excess in order to obtain a gingival contour of the 11 aesthetically harmonious with that of the 21, and compatible with the individual and professional hygiene maneuvers. This intervention could not be performed except in the presence of a sufficient attached gingiva height [15, 16].
Frenectomy or total surgical removal of the frenum was indicated because of its low position: to make the marginal gingiva unstable, to impede the control of the plate, to impede the taking of the impression, disharmonious aspect for the aesthetics of the smile [17-20].
Timing was essential: this phase allowed us to appreciate the stabilization of the periodontal environment at the stage of the transient prostheses and the final aesthetic aspect of the gingival frame after surgical installation [21, 22].
Conclusion
Pre-prosthetic periodontal surgery is a therapeutic necessity to ensure the reliability and sustainability of restorative treatments. It is essential when it is necessary to promote a prosthetic morphology combining aesthetics and respect for the integrity of the periodontium. It must follow a treatment plan that emanates from a detailed and exhaustive clinical observation. It is the only guarantee of the smooth progress of the various therapeutic steps without major surprises [4, 23, 24].
References
- Al Wazzan KA (2004) The visible portion of anterior teeth at rest. J Contemp Dent Pract. 5(1): 53-62.
- Armand S (1999) Methodology of coronary peripheral preparations for esthetic fixed prostheses. Cah Proth. 108: 63-74.
- ArmandS (1999) Fixed prosthesis and periodontium. Inf Dent. 11: 771.
- HoudrainS, ErwanM, Lecerf J (2004) What is the interest of the temporary prosthesis to prepare the marginal periodontal before a footprint ? j prosthetic strategy. 5: 349-54.
- Borghetti A, LabordeG (1996) Pro-prosthetic periodontal surgery. Actual Odontostomatol(Paris). 194-227.
- Borghetti A, Monnet-Corti V (2000) Physiopathology and clinical examination of the mucogingival complex. Periodontal plastic surgery. Paris: CdP, 41-67.
- Glise JM, Monnet-Corti V, Borghetti A (1999) Contribution of periodontics to dental aesthetics. Cah Proth. 108: 49-60.
- Laborde G (2000) Marginal tissues and fixed prosthesis. Periodontal plastic surgery. Paris: CdP, 361-85.
- Ouhayoun JP (1999) Aesthetic and reconstructive periodontics. Real Clin. 10: 73-91.
- Zuck G (2003) Faced with prospthetic failure. Inf Dent. 31: 2167-70.
- Altglass S (1997) The preprosthetic periodontal phase. Inf Dent. 34: 2439-40.
- Borghetti A, Monnet-Corti V (2000) Plastic surgery: the conjunctive graft associated with the flap positioned coronally. Periodontal plastic surgery. Paris: CdP, 209-19.
- Danan M, Ben Mehdi S (2003) Aesthetic Coronary elongation. J Parodontol. 22: 133-44.
- Davarpanah M, Caraman M, Jakubowicz B, Kébir M (2004) Aesthetic coronary elongation. Alternatives. 11: 215-23.
- Danan M, Dridi SM (2000) Gingivectomies. Real Clin. 11: 169-79.
- Liébart MF, Borghetti A (2003) Periodontal resection plastic surgery. J Parodontol Impl Orale. 22: 171-4.
- Borghetti A, Glise JM (2000) Arrangement of the edentulous ridge for the prosthesis fixed on natural pillars. periodontal plastic surgery. Paris: CdP, 391-419.
- Borghetti A, Monnet-Corti V (2000) Frénéctomie. periodontal plastic surgery. Paris: CdP, 179-88.
- Hugly C (1995) Frénéctomie lingual. Real Clin. 6: 313-6.
- Wilson G (2003) Periodontal Maintenance. Real Clin. 14: 347-56.
- TaiebF, GalloisF, DananM (1999) Preprosthetic surgical coronary elongations. Cah Proth. 105: 7-17.
- Viargues P, MeyerJ (1995) Minimal biological space. J Parodontol. 14: 269-274.
- Borghetti A, Monnet-Corti V (2000) The flap positioned laterally. Periodontal plastic surgery. Paris: CdP, 127-33.
- Hürzeler MB, Weng D (1999) Functional and esthetic outcome enhancement of periodontal surgery by application of plastic surgery principles. Rev Int Parod Dent Rest. 19: 37-43.





