Radicular Cyst on Deciduous Molar or Dentigerous Cyst on Permanent Tooth?
Boudaoud Z*, Maou S, Badi Y
Pathology and Oral Surgery Department of the University Hospital Mustapha - Algiers.
*Corresponding Author
Zahia Boudaoud
Professor, Pathology and Oral Surgery Department of the University Hospital Mustapha - Algiers
Fax: 00213 021235251
E-mail: zahia.bakir2016@yahoo.com
Received: August 20, 2016; Accepted: September 19, 2016; Published: September 22, 2016
Citation: Boudaoud Z, Maou S, Badi Y (2016) Radicular Cyst on Deciduous Molar or Dentigerous Cyst on Permanent Tooth?. Int J Dentistry Oral Sci. 3(9), 331-335. doi: dx.doi.org/10.19070/2377-8075-1600066
Copyright: Boudaoud Z© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distrbution and reproduction in any medium, provided the original author and source are credited.
Abstract
The radicular cysts developed on primary teeth are infrequent compared to their evolution in permanent teeth. However, dentigerous cysts are ranked second in frequency after inflammatory cysts. They surround the crown of a tooth erupting while the radiculo- inflammatory dental cysts are hanging from the roots of the mortified teeth. This is the probable coexistence of these two entities that we have been faced in a patient aged 10 years with mixed dentition who presented a radiolucent lesion surrounding infected roots of a mandibular second primary molar in the vicinity of the tooth successor. In our presentation, we discuss problem diagnosis but also treatment. Indeed, we proceeded to avulsion of deciduous molar and we opted for a cystotomy or marsupialisation to preserve the replacement tooth.
2.Introduction
3.Case report
4.Treatment
4.Follow up
5.Discussion
6.Conclusions
7.References
Introduction
Radicular Cyst; Nonvital Decidious Molar; Dentigerous Cyst; Decompression; Marsupialisation;Spontaneous Eruption.
Introduction
Radicular cysts of inflammatory origin are due to the pulp necrosis. They are most prevalent in permanent dentition but their frequency in primary dentition is about 0.5 to 3.3% [1].
Dentigerous cysts result from abnormal development of enamel epithelium. In a pediatric population, they represent 64.8% of all cysts of the jaws and are ranked first in terms of frequency before inflammatory cysts [2]. These cysts are common among children and adolescents and are manifested by a radiolucent picture that forms around the crown of a permanent tooth that has not changed in the arch.
The aims of this study are to report a case of radicular cyst developed on a deciduous molar with a possible diagnosis of dentigerous cyst related to the successor tooth and conservative treatment with a marsupialisation has clarified the diagnosis but also promoted the development of premolar to its eruption site.
Case report
10 years old child without medical and surgical history was referred from his general dental practitionner for left mandibular swelling.
The history of the disease stretching back to 7 months marked by the appearance of a mandibular swelling gradually increasing volume, which has motivated parents to consult. During the oral examination, we noted:
- Poor oral hygiene with four decayed teeth (55, 64, 84, 74) whose 74 has a coronary destruction.
- The Vestibular filling facing the 74 and 75 is covered with a normal mucosa. The internal table is not distorted (Figure 1).
The panoramic radiograph shows the presence of a radiolucent frame pendant to the roots of 74 dilapidated extended to incorporate the crown of 34 to the bud state. This one, in comparison to its counterpart does not seem to be excessively discharged to the basilar, expansion of the cyst.
From these data we discussed two types of cystic lesions:
- Radicular inflammatory cyst in connection with the 74 mortified
- Dentigerous cyst , the lesion surrounds the crown of the 34 changing.
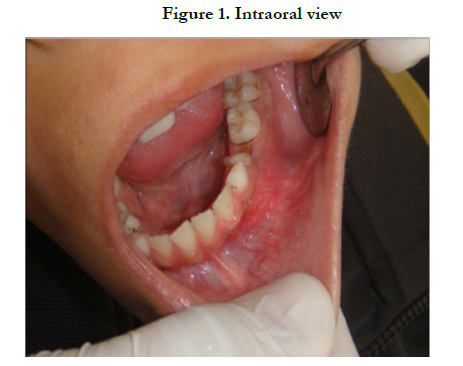

Figure 1. Intraoral view
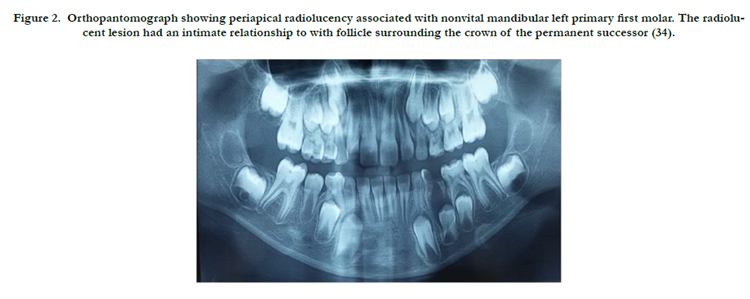
Figure 2. Orthopantomograph showing periapical radiolucency associated with nonvital mandibular left primary first molar. The radiolucent lesion had an intimate relationship to with follicle surrounding the crown of the permanent successor (34).
Treatment
In our treatment plan, we opted for for the extraction of 74 and marsupialization of the cystic lesion in order to preserve 34.
- Under local anesthesia (using 1.8 cc of 2 carpules scandicaine 1% with adrenalin) , after avulsion of the 74, we conducted a cystotomy that left welling purulent fluid (Figure 3) .
- The wound was loosely sutured and packed with iodoform gauze for a week. (Figure 4)
- Medical treatment was prescribed for a period of 8 days: Amoxicillin 1.5 g / day and Paracetamol 900mg / day.
- The cyst wall was addressed later in the laboratory for histhological examination.
- We reviewed the child several times after the procedure to renew the locks and monitor his oral hygiene (Figure 5).
- Histopathological analysis was in favor of Benin inflammatory cyst may correspond to a radiculo dental cyst. (Figure 6)
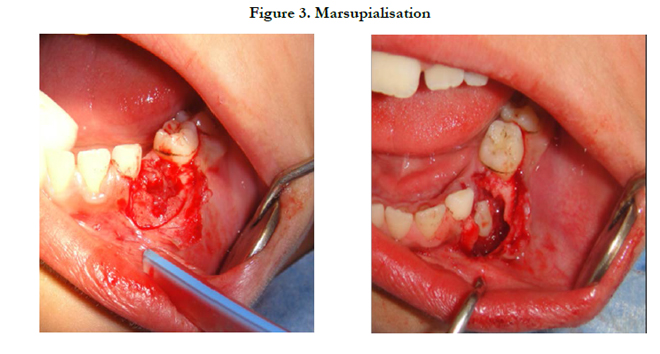
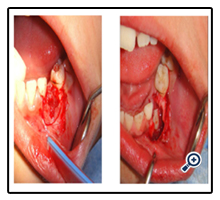
Figure 3. Marsupialisation
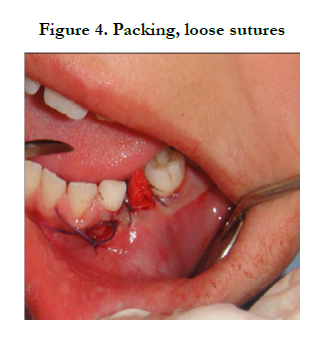

Figure 4. Packing, loose sutures
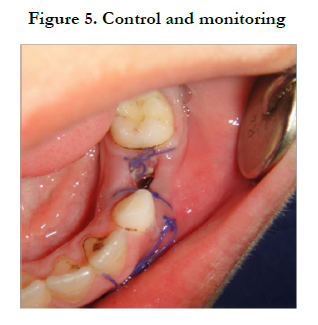
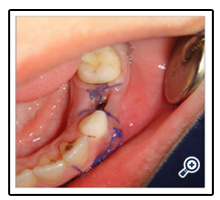
Figure 5. Control and monitoring
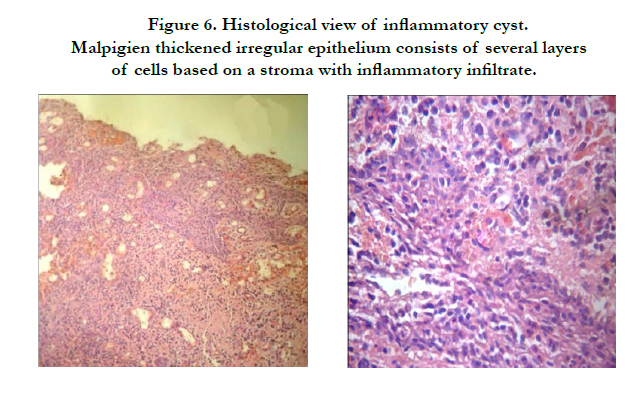
Figure 6. Histological view of inflammatory cyst.Malpigien thickened irregular epithelium consists of several layers of cells based on a stroma with inflammatory infiltrate.
Follow up
Seven months later, the panoramic control radiograph showed the rise of the 34 building with almost 2/3 of its root. It is at the stage of pre emergence incompatible with its degree of root maturation (Figure 7).
Otherwise, we noted a widening around the crowns of 33 and 43 showing an intense activity follicular bags; process to monitor.
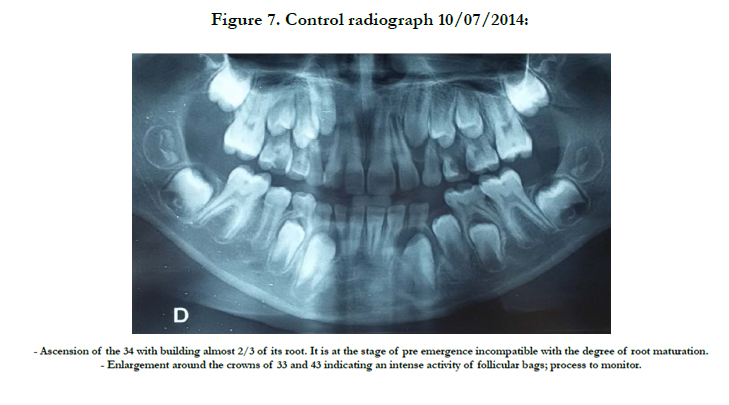
Figure 7. Control radiograph 10/07/2014:
Discussion
Shear [3] estimated that the frequency of dentigerous cysts in the first decade of life is about 9 % , while that of radicular cysts is about 1 % in the same age group.
Most radicular cysts encountered in primary teeth are located at the interradicular area of deciduous molars often suffering from gangrene pulp and having been the object of root canal treatment or mummification [4, 5]. In dentition, the caries process is the cause of inflammatory cyst in the molar sector while in the anterior region is often alveolo - dental injuries that are the cause. These cysts are derived from epithelial debris Malassez present in the dental periodontal ligament following the infiltration of inflammatory cells associated. This chronic inflammation is a consequence of pulp necrosis.
However, a dentigerous cyst is the one that surrounds the crown of an impacted tooth often at the cemento-enamel junction.
It results from the proliferation of enamel epithelium regression after the formation of the enamel.
Radiologically, they manifest in an unilocular radiolucency well defined by a condensate border in the absence of inflammation. This area of osteolysis is pendant to the roots of the infected tooth in the case of a radicular dental cyst and dental cap the crown of an impacted tooth moved into a more or less ectopic position in the case of a dentigerous cyst.
The diagnosis is often delayed for several reasons:
- The periapical osteolytic picture usually associated with primary teeth is often asymptomatic generating little pain or deformity and in many cases, disappeared after avulsion.
- Many radicular cysts are discovered accidentally when taking radiographs.
- Inter root infections on primary teeth tend to drain more than permanent teeth.
- The differential diagnosis in mixed dentition between a radicular cyst and dentigerous cyst is difficult to establish, given the intimate relationship between the deciduous molars and the follicle premolar bud.
Angela Benn [6] confirms that the histological distinction between these two types of lesions is difficult. A final diagnosis should be based on the confrontation of clinical, radiographic and histological critera.
Indeed, histologically, the cyst is always covered with a squamous epithelium in which the reshuffle and the thickness depend, scalability of the inflammatory process. It may contain mucus-secreting and ciliated cells.
In our case, we think that inflammation from the deciduous tooth necrotic propagating caused a chronic irritation of the follicle of the permanent tooth development; simulating the formation of dentigerous cysts.
Benn and Altini [6] suggest that there are two types of dentigerous cysts. The first type is of a developmental anomaly or metaplasia which occurs in mature impacted or retained teeth. The second type of inflammatory nature and is manifested in the periapical region of a deciduous tooth mortified and extends follicular bag successor immature permanent tooth.
Benn and Manjunatha [6, 7] prefer the term "inflammatory dentigerous cyst" with respect to the label of follicular cyst pulpoinduced periodontal inflammation of deciduous teeth. Reviewed cases (Table 1) suggest that for several authors [8-24], the treatment of inflammatory dentigerous cysts includes the extraction of non-vital primary tooth and marsupialization of the cyst. This conservative option allows the healing of the cystic cavity and induces the eruption of the permanent tooth. In our case, the opening of the cyst wall stimulated the eruptive movement 34 which is early pre-emergence situation while its root is not built in two-thirds.
The enucleation of the cyst carrying permanent teeth associated with it is not the ideal solution, because the sacrifice of these teeth in children can have functional impact (occlusal order in the sagittal and transverse directions). Add to this the problem of replacing missing teeth in growing children.
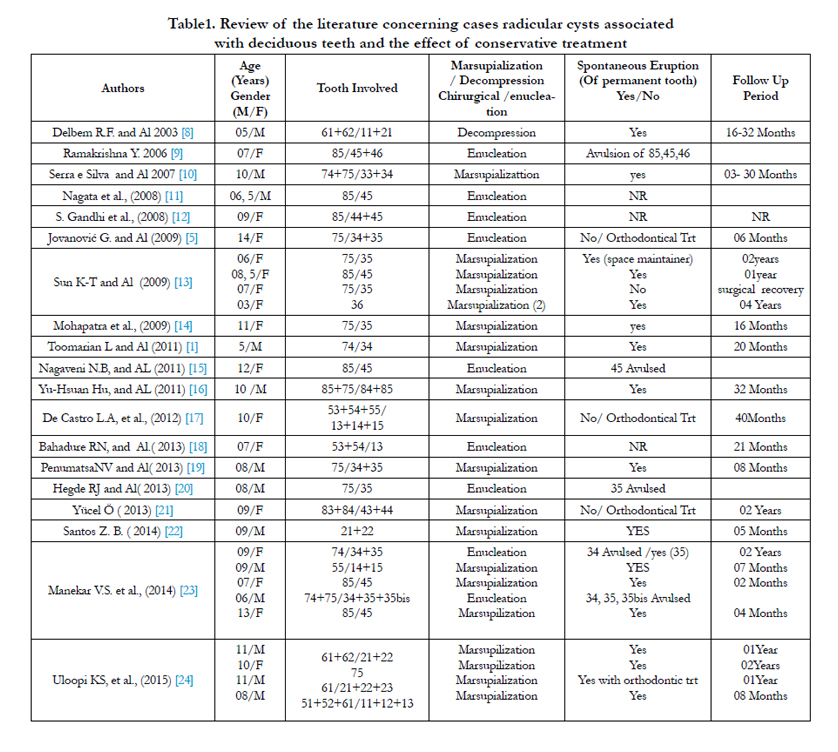

Table1. Review of the literature concerning cases radicular cysts associated with deciduous teeth and the effect of conservative treatment
Conclusions
The reported case lets discuss the differential diagnosis of cystic lesions, which is especially difficult in mixed dentition as a result of the close proximity relationship between deciduous tooth and permanent tooth germ. A clinical, radiological and histological correlation is essential to achieve a positive diagnosis.
Therapeutically, whenever possible, should be favored marsupialization is a simple method of realization and in addition, seeks to preserve the permanent tooth changing.
Respect for annual inspections, would have allowed, by intercepting the carious disease avoid surgery.
References
- L. Toomarian, M. Moshref, M. Mirkarimi, A Lotfi, M Beheshti (2011) Radicular cyst associated with a primary first molar: A case report; J Dent (Tehran). 8(4): 213-217.
- Padmakumar SK, Beena VT, Aloka D, Lav R, Sivakumar R (2015) Cysts of the Jaws in Pediatric Population: A 12-Year Institutional Study. Oral Maxillofac Pathol J. 6(1): 532-536.
- Shear M (1994) Developmental odontogenic cysts. An update. J Oral Pathol Med. 23(1): 1-11.
- Elango I, Baweja DK, Noorani H, Shivaprakash PK (2008) Radicular cysts associated with deciduous molar following pulp therapy: A case report. Dent Res J. 5(2): 95-8.
- Goran Jovanovic and Al (2009) A radicular cyst in lower deciduous molar Acta Stomatologica Naissi. 25(60): 901 – 906.
- Angela Benn, Mario Altini; (1996) Dentigerous cysts of inflammatory origin “A clinicopathologic study”. Oral Surgery Oral Medicine Oral Pathology. 8(1): 203-209.
- Manjunatha Bhari Sharanesha, Deepak Pateel Gowda Sadashivappa (2010) Dentigerous Cyst of Inflammatory origin: a Diagnostic Challenge. Acta Stomatol Croat. 44(1): 61-64.
- Delbem, R. F. Cunha, Vieira , Pugliesi (2003) Conservative treatment of a radicular cyst in a 5-year-old child: a case report. Int J Paediatr Dent. 13(6): 447–450.
- Ramakrishna Y, Verma D (2006) Radicular cyst associated with a deciduous molar: A case report with unusual clinical presentation. J Indian Soc Pedod Prev Dent. 24(3): 158-160.
- Fabricio Moreira Serra e Silva, Renato Sawazaki, Márcio de Moraes (2007) Eruption of Teeth Associated with a Dentigerous Cyst by only Marsupialization Treatment: A Case Report. J Dent Child. 74(3): 228-30.
- Nagata T et al., (2008) Radicular cyst in a deciduous tooth. Journal of Dentistry for Children. 75(1): 80-84.
- S. Gandhi, D.L. Franklin, (2008) Presentation of a Radicular Cyst Associated with a Primary Molar. Eur Arch Paediatr Dent. 9 (1): 56-9.
- Sun K-T, Chen MY, Chiang HH, Tsai HH (2009) Treatment of Large Jaw Bone Cysts in Children. J Dent Child. 76(3): 217-22.
- Mohapatra PK, Joshi N (2009) Conservative Management of a Dentigerous Cyst Associated with an Impacted Mandibular Second Premolar in Mixed Dentition: A Case Report . J Dent Res Dent Clin Dent Prospect. 3(3):98-102.
- Nagaveni NB, Umashankara KV, Radhika NB (2011) Inflammatory dentigerous cyst associated with an endodontically treated primary second molar: a case report. Archives of Orofacial Sciences. 6(1): 27-31.
- Yu-Hsuan Hu, Yu-Liang Chang, and Aileen Tsai (2011) Conservative treatment of dentigerous cyst associated with primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 112(6): e5-e7.
- De Castro LA, Campos Maia SR (2012) Maxillary osteolytic lesion in a 10-year-old girl: A dentigerous or radicular cyst? A case report and Discussion. Rev. Port. Estomatol Med. Dent. Cir. Maxilofac. 53(1): 24–28.
- Bahadure RN, Khubchandani M, Thosar NR, et al., ( 2013) BMJ Case Report.
- Penumatsa NV, Nallanchakrava S, Muppa R, Dandempally A, Panthula P (2013) Conservative Approach in the Management of Radicular Cyst in a Child: Case Report Case Reports in Denti. 48: 1-3.
- Hegde RJ, Khare SS, Devrukhkar VN (2013) Dentigerous Cyst in a young child: Clinical Insight and A Case report. J Indian Soc Pedod Prev Dent. 3(3): 209-11.
- Yücel Ö, Yildirim G, Tosun G, Müge Baka Z, Bedii Göyenç Y, Günhan Ö (2013) Eruption of Impacted Permanent Teeth after Treatment of a Dentigerous Cyst: A Case Report. J Dent Child. 80(2): 92-6.
- Santos ZB. Beltrame AP, Bolan M, Grando LJ, Rodríguez Cordeiro MM (2014) Dentigerous Cyst of Inflammatory Origin. J Dent Child. 81(2): 112-6.
- Manekar VS et al., (2014) Cysts in Periradicular Region of Deciduous Molars in Mixed Dentition: Retrospective Study of Five Cases. Int J Clin Pediatr Dent. 7(3): 229-235.
- Uloopi KS, Shivaji RU, Vinay C, P, Shrutha SP, Chandrasekhar R (2015) Conservative management of large radicular cysts associated with non-vital primary teeth: A case series and literature review. J Indian Soc Pedod Prev Dent. 33(1): 53-6.





