CBCT Variants of Sinonasal Cavity: What Oral and Maxillofacial Radiologists Need to Know
Omami G
Diplomate, American Board of Oral and Maxillofacial Radiology Assistant Professor, Department of Oral Health Practice University of Kentucky College of Dentistry, Rose Street, Lexington, Lexington, USA.
*Corresponding Author
Galal Omami, BDS, MSc, MDentSc, FRCD,
Diplomate, American Board of Oral and Maxillofacial Radiology Assistant Professor,
Department of Oral Health Practice University of Kentucky College of Dentistry, 800 Rose
Street, Lexington, KY 40536 Lexington, KY 40536, USA.
Tel: (859) 323 9833
Fax: (859) 323 9136
E-mail: jellodent@yahoo.com
Received: July 27, 2016; Accepted: August 19, 2016; Published: August 22, 2016
Citation: Omami G (2016) CBCT Variants of Sinonasal Cavity: What Oral and Maxillofacial Radiologists Need to Know. Int J Dentistry Oral Sci. 3(8), 301-308.DOI : dx.doi.org/10.19070/2377-8075-1600061
Copyright: Omami G© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
2.Nasal Cavity
2.1.Deviated nasal septum
2.2.Concha Bullosa
2.3.Paradoxical Middle Turbinate
2.4.Septal spur
3.Maxillary Sinus
3.1.Alveolar recess of maxillary sinus
3.2.Palatine recess of maxillary sinus
3.3.Accessory ostia
3.4.Maxillary sinus septa
4.Ethmoidal sinuses
4.1.Haller (Infraorbital ethmoid) cells
4.2.Agger nasi cells
4.3.Onodi (Sphenoethmoidal) cells
4.4.Supraorbital cell
5.Frontal Sinuses
5.1.Teaching point
6.Sphenoidal Sinus
6.1.Vomeral recess of sphenoid sinus
6.2.Pterygoid recess of sphenoid sinus
6.3.Clinoid recess of sphenoid sinus
6.4.Lateral recess of sphenoid sinus
7.Conclusion
8.References
Introduction
The anatomical variations of sinonasal cavity are well documented in literature [1-3]. The sinonasal cavity is usually partially or fully imaged in cone beam CT (CBCT) exams taken for the teeth and jaws. So, oral and maxillofacial radiologists need to be familiar with the regional anatomy of the sinonasal complex (Figure 1). However, some anatomical variations can predispose to sinus disease or complicate sinus surgery. Therefore, solid understanding of the imaging anatomy of the sinonasal cavity is of paramount importance in order to eliminate or minimize surgical complications [4, 5]. CBCT scan is an advancement in technology that has begun to emerge as a potentially low dose and high contrast 3D imaging modality for visualizing bony structures in the dentomaxillofacial complex [6]. The objective of this pedagogical review is to provide oral and maxillofacial radiologists with a pictorial overview of the common anatomical variations of the sinonasal cavity as depicted on CBCT images.
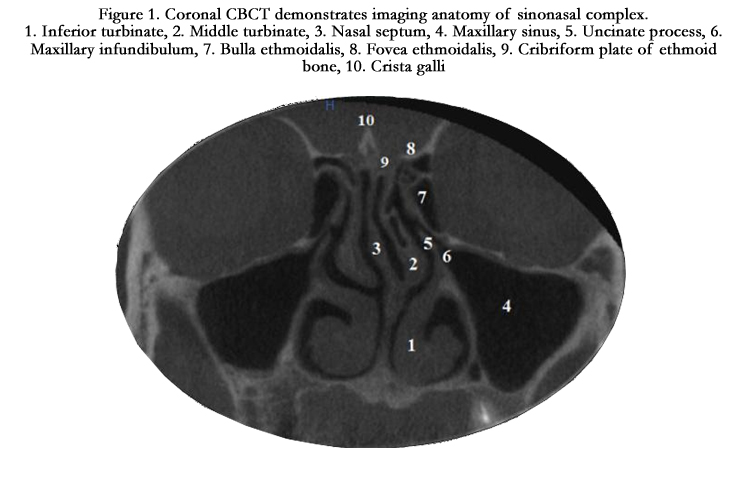
Figure 1. Coronal CBCT demonstrates imaging anatomy of sinonasal complex. 1. Inferior turbinate, 2. Middle turbinate, 3. Nasal septum, 4. Maxillary sinus, 5. Uncinate process, 6. Maxillary infundibulum, 7. Bulla ethmoidalis, 8. Fovea ethmoidalis, 9. Cribriform plate of ethmoid bone, 10. Crista galli
Nasal Cavity
The nasal septum is made up of bony and cartilaginous parts. The bony component is formed by the vomer and perpendicular plate of ethmoid done. The septum usually deviates off the median plane (Figure 2). Septal deviation is the most common variation of the nasal cavity. Earwaker reported prevalence of septal deviation in 44% of individuals with slight right side predominance but equal gender distribution [7]. Septal deviation can be too severe that it comes into contact with the lateral nasal wall and obstructs breathing or exacerbates snoring.
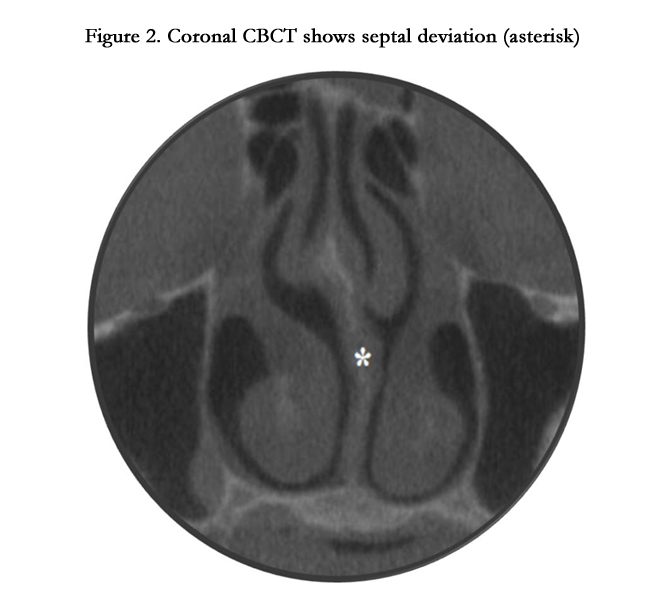
Figure 2. Coronal CBCT shows septal deviation (asterisk)
Concha bullosa is a middle turbinate that is pneumatized by an ethmoid air cell (Figure 3). Concha bullosa is only recognized when the bulbous portion of the turbinate is aerated. Aeration into the upper lamina attachment of the turbinate is simply referred to as partial aeration of the turbinate. Prevalence of concha bullosa was reported in 55% and 34% of patients in Earwaker and Zinreich studies, respectively [7, 8]. Concha bullosa can compromise the middle meatus, particularly the ostiomeatal complex, and predispose to sinus disease due to its negative effect on the mucociliary drainage [9].
Ostiomeatal complex is the term used to refer collectively to the maxillary sinus ostium, hiatus semilunaris, frontal recess (frontonasal duct), middle ethmoidal cells ostia, and middle meatus (Figure 1).
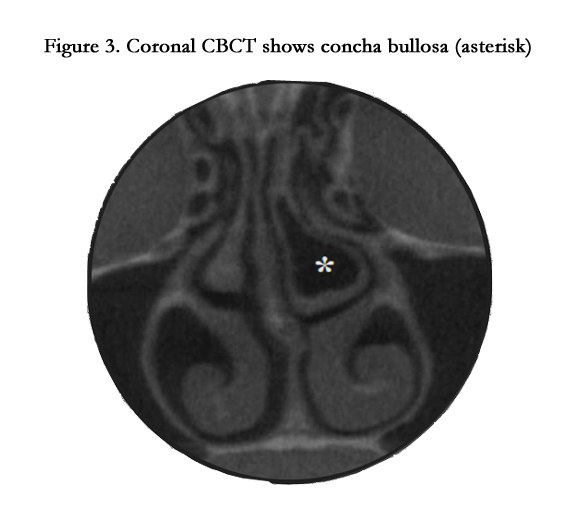
Figure 3. Coronal CBCT shows concha bullosa (asterisk)
The configuration of middle turbinate normally follows that of the inferior turbinate (i.e. convex medially). Paradoxical middle turbinate has a reversed configuration (convex laterally) (Figure 4). Perez et al., reported paradoxical middle turbinate in 10% of patients [4]. Earwaker identified 269 cases (33%) with paradoxical middle turbinate [7]. Unless there is obvious obstruction of the nasal airways from the paradoxical turbinate, there is no consistent literature that relates paradoxical middle turbinate to sinusitis.
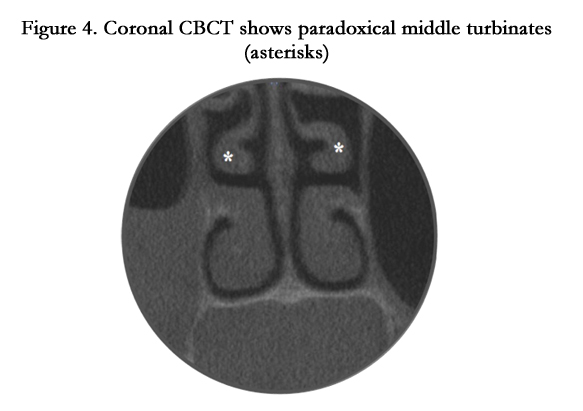
Figure 4. Coronal CBCT shows paradoxical middle turbinates (asterisks)
Septal spur is a transverse bony ridge arising from the nasal septum (Figure 5). Takanishi has proposed that malalignment of the three components of the nasal septum (Septal cartilage, perpendicular plate of ethmoid bone and vomer) gives rise to formation of septal spur [10]. Prevalence of septal spur was recognized in 18.5% of patients with a four fold predominance on the left side [7].
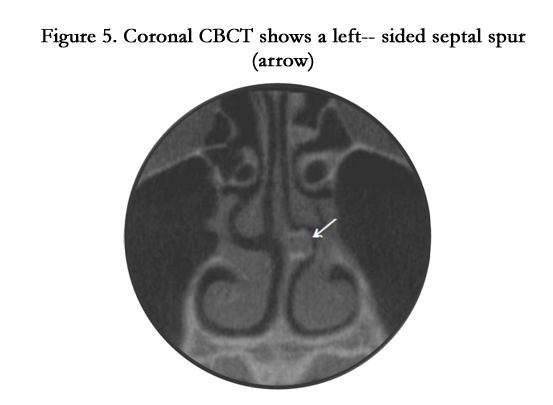
Figure 5. Coronal CBCT shows a left-‐sided septal spur (arrow)
Maxillary Sinus
Each maxillary sinus has four recesses: The zygomatic recess, extending into the body of the zygoma; The palatine recess, extending into the hard palate; The tuberosity recess, extending into the maxillary tuberosity; and The alveolar recess, extending into the alveolar process of the maxilla (Figure 6). In dentate maxilla, the alveolar recess is closely related to the molar and premolar teeth whose roots may produce conical projections into the sinus floor. However, alveolar recess is more seen in edentulous sites of maxilla where the height of the residual alveolar ridge is additionally compromised by the crestal bone loss. The reported prevalence of alveolar recess is 18% [7].
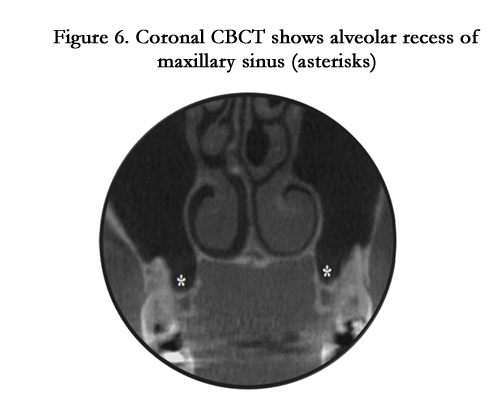
Figure 6. Coronal CBCT shows alveolar recess of maxillary sinus (asterisks)
The hard palate (nasal floor) is formed of the palatal process of maxilla (anterior 2/3) and horizontal plate of palatine bone (posterior 1/3). Palatine recess of maxillary sinus may be encountered on routine radiographs and confused for a lesion (Figure 7). Earwaker has recognized the palatal recess when the distance between the recesses is less than half the width of the nasal floor at the level of the inferior meati. He reported this variant is 11.5% of his patients [7].
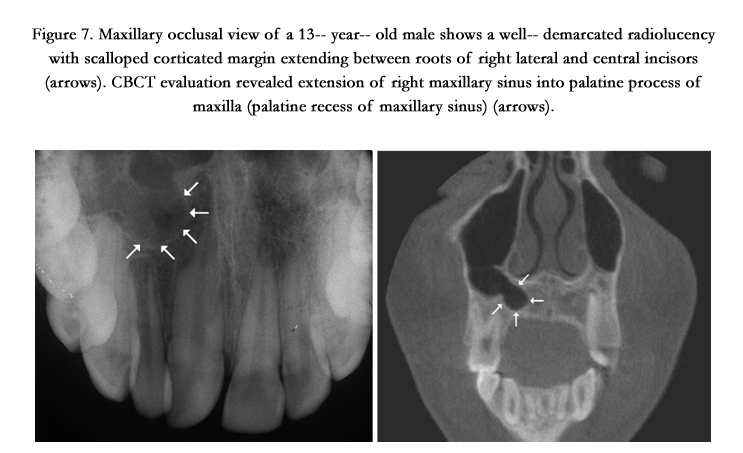
Figure 7. Maxillary occlusal view of a 13year old male shows a well demarcated radiolucency with scalloped corticated margin extending between roots of right lateral and central incisors (arrows). CBCT evaluation revealed extension of right maxillary sinus into palatine process of maxilla (palatine recess of maxillary sinus) (arrows).
Messerklinger has reported defects in the middle meati behind and below the uncinate process [11]. These defects are concealed by mucoperiostium and consequently referred to as nasal fontanelles, which in turn were described as the sites of accessory ostia for maxillary sinus (Figure 8). The reported prevalence in the literature is 13% [7].
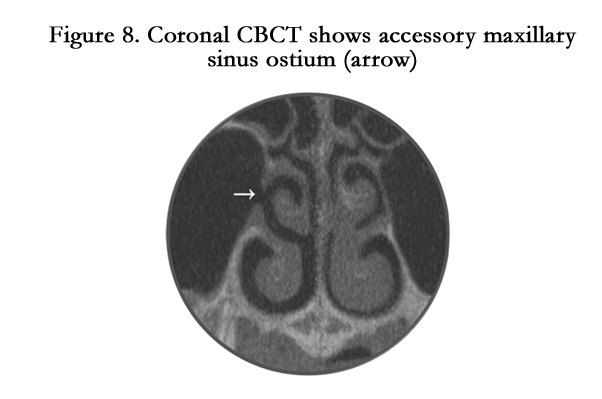
Figure 8. Coronal CBCT shows accessory maxillary sinus ostium (arrow)
Partial or complete intrasinus septum partitions the sinus cavity into multiple compartments (Figure 9). They are usually unilateral and encountered in the anterior portion of the sinus. This variant was reported in 3% of patients in Earwaker’s series [7].
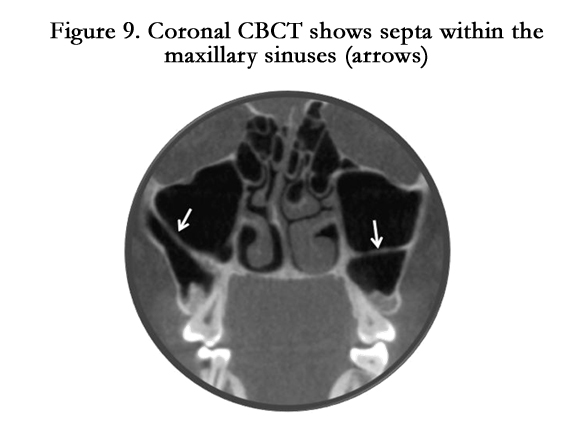
Figure 9. Coronal CBCT shows septa within the maxillary sinuses (arrows)
Ethmoidal sinuses
Haller cells were first described by Albert von Haller as the anterior ethmoidal air cells located along the medial portion of the orbital floor lateral to the maxillary infundibulum [12] (Figure 10). Enlarged or inflamed Haller cell can significantly constrict the maxillary sinus ostium and predispose to sinus disease [13]. Due to its critical location, inflamed Haller cell has been reported as potential cause of unilateral orbital cellulitis [14]. The reported prevalence of Haller cell ranges from 2.7% to 45% [9]. It is likely these mixed reports reflect the inconsistency in defining Haller cell.
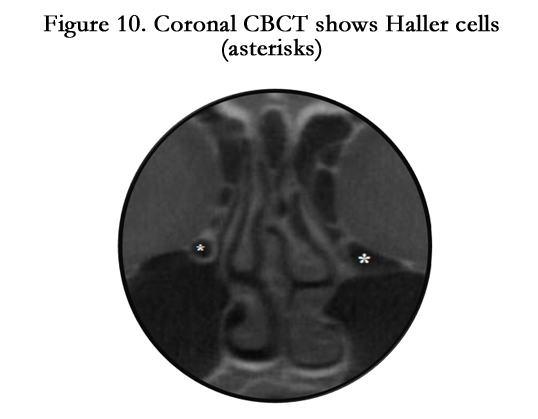
Figure 10. Coronal CBCT shows Haller cells (asterisks)
Agger nasi (nasal ridge) cells are the most anterior ethmoidal air cells, which are formed by pneumatization of the lacrimal bone and the frontal process of maxilla (Figure 11). Agger nasi cells are identified on sinus CT by its location just superior to the upper end of nasolacrimal duct. However, the inconsistency in defining agger nasi cells may have partly resulted in wide range of occurrences (10% -98%) [2, 15]. Agger nasi cells are closely related to the frontal recess (frontonasal duct); consequently, enlargement of these cells may obstruct the frontonasal duct and result in frontal sinus mucocele [2].
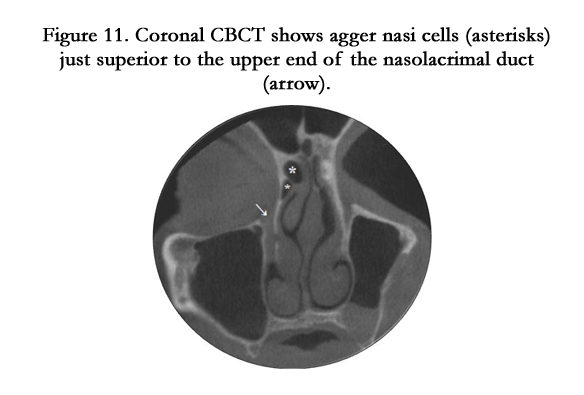
Figure 11. Coronal CBCT shows agger nasi cells (asterisks) just superior to the upper end of the nasolacrimal duct (arrow).
Onodi cells were first described in 1910 by Adolf Onodi as the most posterior ethmoid cell that pneumatizes superolaterally into the sphenoid sinus and is intimately associated with the optic canal [16] (Figure 12). Prevalence of Onodi cell was estimated to range from 3.4% to 51% [17]. As Onodi cells abut or may even surround the optic nerve, thereby placing this nerve at a higher risk during surgical exploration of these cells [2].
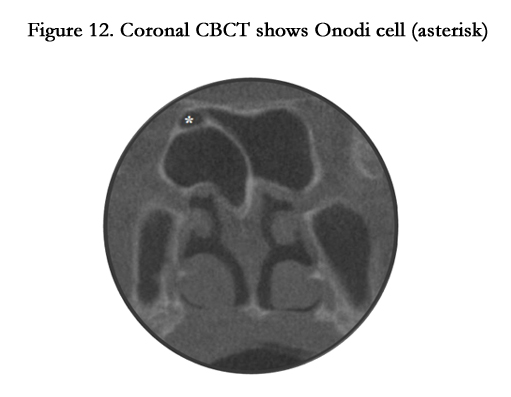
Figure 12. Coronal CBCT shows Onodi cell (asterisk)
Supraorbital cells were described by Som as supraorbital extension of anterior ethmoidal cells into the orbital roof [18] (Figure 13). Earwaker identified these cells in 8% of cases [7].
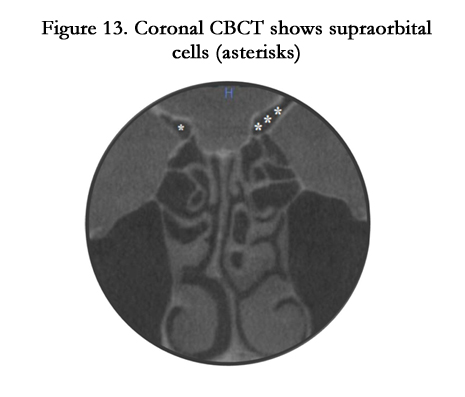
Figure 13. Coronal CBCT shows supraorbital cells (asterisks)
Frontal Sinuses
The frontal sinuses are the only paranasal sinuses that are absent at birth. The sinuses undergo primary expansion with the eruption of the first deciduous molars and secondary expansion with the eruption of the first permanent molars [19]. However, they only reach their full size after puberty. Additional sinus expansion may be attributed to the age-related changes in the volume of sinus aeration [2]. In extreme cases, the frontal sinuses may expand to pneumatize the entire frontal bone (Figure 14). Moreover, frontal sinus aeration may expand to involve crista galli (part of ethmoid bone) (Figure 16). Som et al., reported crista galli pneumatization in 13% of subjects [20].
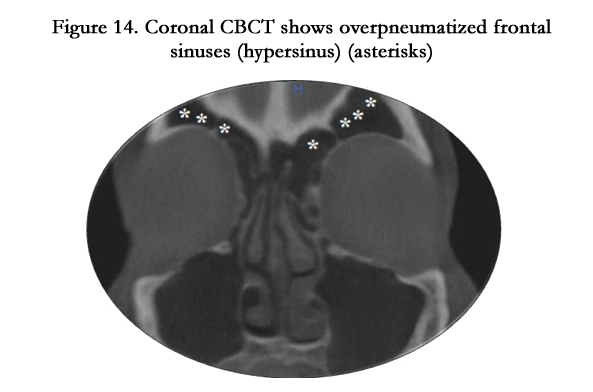
Figure 14. Coronal CBCT shows overpneumatized frontal sinuses (hypersinus) (asterisks)
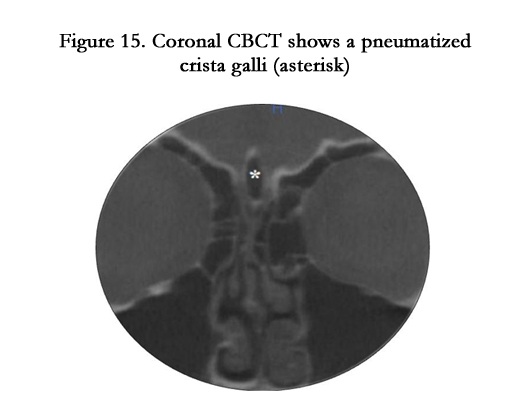
Figure 15. Coronal CBCT shows a pneumatized crista galli (asterisk)
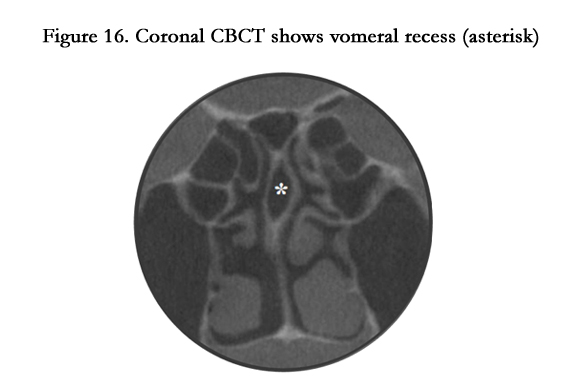
Figure 16. Coronal CBCT shows vomeral recess (asterisk)
Pneumosinus dilatans is a rare condition refers to an aerated sinus that is abnormally expanded; however, sinus walls are of normal thickness. Extension of sinus aeration beyond the normal bony boundaries differentiates pneumosinus dilatans from hypersinus. Pneumocele refers to an aerated sinus with expansion and thinning of the bony sinus walls [21].
Sphenoidal Sinus
Vomeral recess of sphenoid sinus is caused by downward extension of the sphenoid sinus into the posterior aspect of the nasal septum (vomer) (Figure 15). This recess was reported in 8% of patients [7].
Pterygoid recess of sphenoid sinus occurs by extension of the sinus cavity into the ptreygoid process of sphenoid bone (Figure 16). Hewaidi et al., defined pterygoid recess when the pneumatization extends beyond a horizontal plane across the pterygoid (Vidian) canals [22]. They encountered pterygoid recess in 29% of their patients and shown significant association between pterygoid recess and ipsilateral protrusion of pterygoid canal into the sphenoid sinus cavity (Figure 17). Pterygoid recess of sphenoid sinus may be encountered in panoramic or lateral ceph radiography as well-defined radiolucency posterior to the maxillary sinus and can be mistaken for an abnormality [23] (Figure 18).
Sluder’s (Vidian) neuralgia is a rare disorder has been hypothetically attributed to irritation of Vidian nerve fibers secondary to sphenoid sinusitis [24]. Sluder’s neuralgia is characterized by unilateral, severe, burning pain starting around the eye and the bridge of the nose, radiating to the maxilla and maxillary teeth, zygoma, mastoidal area and occiput, or as down as the shoulder and arm.
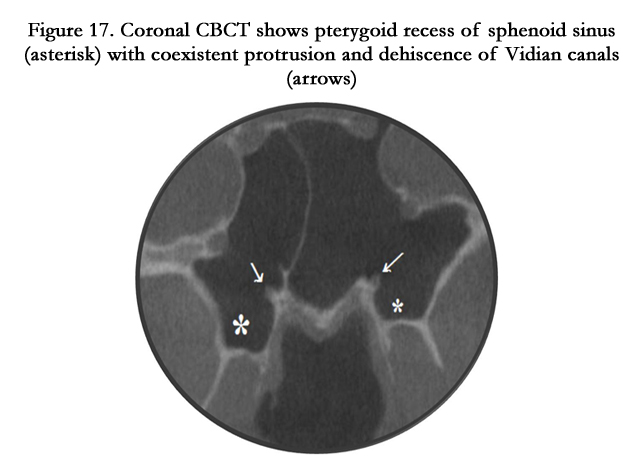
Figure 17. Coronal CBCT shows pterygoid recess of sphenoid sinus (asterisk) with coexistent protrusion and dehiscence of Vidian canals (arrows)
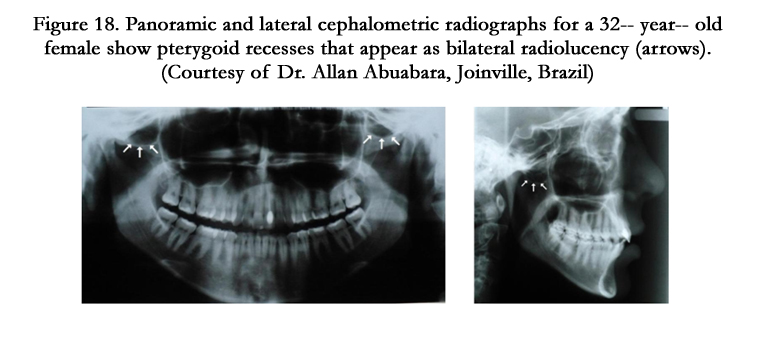
Figure 18. Panoramic and lateral cephalometric radiographs for a 32 year old female show pterygoid recesses that appear as bilateral radiolucency (arrows). (Courtesy of Dr. Allan Abuabara, Joinville, Brazil)
Clinoid recess is pneumatization of the anterior clinoid process by the sphenoid sinus (Figure 19). Bolger et al., reported a prevalence of clinoid recess of 14% [9]. Clinoid recess is supposed to concur with ipsilateral protrusion of the optic canal or internal carotid artery (Figure 20). Accordingly, neurovascular injury can occur as a result of surgical trauma or sinus disease [2].
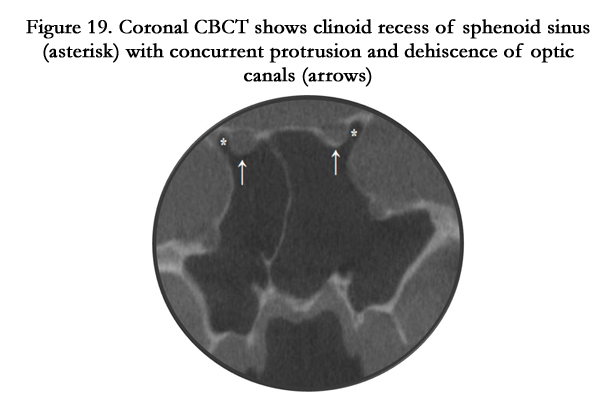
Figure 19. Coronal CBCT shows clinoid recess of sphenoid sinus (asterisk) with concurrent protrusion and dehiscence of optic canals (arrows)
Lateral recess of sphenoid sinus occurs when the sinus cavity extends laterally into the greater wing of sphenoid bone (floor of middle cranial fossa) (Figure 20). Hewaidi et al., recognized the lateral recess when the pneumatization extends beyond a vertical plane along the maxillary canal (foramen rotundum) [22]. They have reported significant co-existence between the lateral recess of sphenoid sinus and ipsilateral protrusion of the maxillary canal into the sinus cavity (Figure 20). A protruded or dehiscent maxillary canal renders the maxillary nerve vulnerable to damage during sphenoid surgery. Moreover, inflammatory irritation of the maxillary nerve can occur secondary to sphenoid sinusitis and may present clinically as neuralgic pain in the distribution of the nerve [25]. Hewaidi et al., reported lateral recess in 20% of their patients [22].
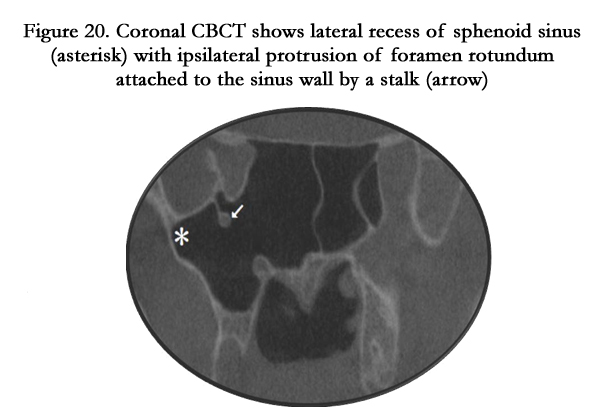
Figure 20. Coronal CBCT shows lateral recess of sphenoid sinus (asterisk) with ipsilateral protrusion of foramen rotundum attached to the sinus wall by a stalk (arrow)
Conclusion
This educational review highlighted the common sinonasal variations with reference to their clinical implications. Some variations can appear as well-demarcated radiolucency on routine imaging leading to a possible misdiagnosis of abnormality. This necessitates oral and maxillofacial radiologists to get accustomed to the sinonasal anatomy. The CBCT report should include not only details about the area of interest but also information about the anatomical variants and their implications. However, the presence of variants does not constitute a pathologic condition per se.
References
- Cheung DK, Attia E, Kirkpatrick DA, Marcarian B, Wright B (1993) An anatomic and CT scan study of the lateral wall of the sphenoid sinus as related to the transnasal transethmoid endoscopic approach. J Otolaryngol 22(2): 63-68.
- Mafee MF, Chow JM, Meyers R (1993) Functional endoscopic sinus surgery: anatomy, CT screening, indications, and complications. Am J Roentgenol 160(4): 735-744.
- Delano MC, Fun FY, Zinrich SJ (1996) Relationship of the optic nerve to the posterior paranasal sinuses: a CT anatomic study. Am J Neuroradiol 17(4): 669-675.
- Perez P, Sabate J, Carmona A, Catalina CJ, Jimenez J (2000) Anatomical variations in the human paranasal sinus region studied by CT. J Anat 197(2): 221-227.
- Mecit K, Murat K, Fatih A, Omer O, Adnan O, et al., (2004) Remarkable anatomic variation in paranasal sinus region and their clinical importance. Eur J Radiol 50(3): 296- 302.
- Miracle AC, Mukherji SK (2009) Cone beam CT of the Head and Neck, Part 2: Clinical Applications. Am J Neuroradiol 30(7): 1285–1292.
- Earwaker J (1993) Anatomic Variants in sinonasal CT. Radiographics 13(2): 381-415.
- Zinreich SJ, Mattox DE, Kennedy DW, Chisholm HL, Diffley DM, et al., (1988) Concha bullosa: CT evaluation. J Comput Assist Tomogr 12(5): 778-784.
- Bolger WE, Butzin CA, Parsons DS (1991) Paranasal sinus bony anatomic variations and mucosal abnormalities: CT analysis for endoscopic sinus surgery. Laryngoscope 101(1): 56-64.
- Takanishir R (1987) The formation of the nasal septum and the etiology of septal deformity. The concept of evolutionary paradox. Acta Otolaryngol Suppl 443: 1-160.
- Messerklinger W (1978) Endoscopy of the nose.Urban & Schwarzenberg, Baltimore. 180.
- Von Haller A (1803) First Lines of Physiology. (3rd edn), Obrabran Penniman, New York. 223-225.
- Sarah AS, David RE (1997) The Anatomic Relevance of the Haller Cell in Sinusitis. Am J Rhinol 11(3): 219-223.
- Sebrechts H, Vlaminck S, Casselman J (2000) Orbital edema resulting from Haller cell pathology: 3 case reports and review of literature. Acta Otorhinolaryngol Belg 54(1): 39- 43.
- Zinreich SJ, Kennedy DW, Rosenbaum AE (1987) Paranasal sinuses: CT imaging requirements for endoscopic surgery. Radiology 163(3): 769-775.
- Onodi A (1910) The Optic Nerve and Accessory Sinuses of the Nose: A contribution to the study of canalicular neuritis and atrophy of the optic nerve of nasal origin. Wood, New York. 80-81.
- Weinberger D, Anand V, Al-‐ Rawi M, Cheng H, Messina A (1996) Surgical anatomy and variations of the Onodi cell. Am J Rhinol 10(6): 365-370.
- Som PM (1985) CT of the paranasal sinuses. Neuroradiology 27(3): 189- 201.
- Gray H (1989) Gray’s Anatomy. (37th edn), Churchill Livingstone, Edinburgh, New York.
- Som PM, Park EE, Naidich TP, Lawson W (2009) Crista Galli Pneumatization Is an Extension of the Adjacent Frontal Sinuses. Am J Neuroradiol 30(1): 31–33.
- Urken M, Som P, Lawson W, Edelstein D, Weber AL, et al., (1987) Abnormally large frontal sinuses II: nomenclature, pathology, and symptoms. Laryngoscope 97(5): 606-611.
- Hewaidi GH, Omami GM (2008) Anatomic Variation of Sphenoid Sinus and Related Structures in Libyan Population: CT scan Study. Libyan J Med 3(3): 128-133.
- Terra ER, FR Guedes, FR Manzi, FN Bo´scolo (2006) Pneumatization of the sphenoid sinus. Dentomaxillofacial Radiol 35(1): 47–49.
- Oomen KP, van Wijck AJ, Hordijk GJ, de RU JA (2010) Sluder’s neuralgia: A trigeminal autonomic cephalalgia? Cephalalgia 30(3): 360–364.
- Chong VF, Fan YF, Lau DP (1994) Imaging the sphenoid sinus. Austrlas Radiol 29: 47-54.





