Integrating Dental Care into Patient Centered Medical Homes and Accountable Care Organizations: A United States of America Perspective
Julie Kazimiroff1*, Sydney Spal1, Deborah Farson2, Paul Meissner1
1 Montefiore Medical Center, Department of Dentistry, The University Hospital of the Albert Einstein College of Medicine, Bronx, New York, USA.
2 Paseo de los Camisos, Santa FE, NM, USA.
*Corresponding Author
Julie Kazimiroff, DDS, MS,
Director of Community Dentistry, Montefiore Medical Center,
The University Hospital of the Albert Einstein College of Medicine,
111 East 210th Street, Bronx, New York 10467, USA.
Tel: 1-718-920-4937
Fax: 1-718-654-4340
E-mail: jkazimir@montefiore.org
Received: July 05, 2016; Accepted: August 06, 2016; Published: August 10, 2016
Citation: Julie Kazimiroff, Sydney Spal, Deborah Farson, Paul Meissner (2016) Integrating Dental Care into Patient Centered Medical Homes and Accountable Care Organizations: A United States of America Perspective. Int J Dentistry Oral Sci. 3(8), 296-300.DOI : dx.doi.org/10.19070/2377-8075-1600060
Copyright: Julie Kazimiroff© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Increasing evidence links oral health to total physical and mental health and, underscores the need to integrate dental health programs with medical care. The newly emerging transition to Patient Centered Medical Homes (PCMH) and Accountable Care Organizations (ACOs) aligns payment and provides incentives for health systems to pursue this strategy. PCMH and ACOs are efforts to improve patient outcomes by creating partnerships between patients, physicians, hospitals, and other caregiving institutions to provide evidenced-based medical care, while slowing the growth of health-related costs.
Although primary medical care is customary in ACOs and in PCMHs, dental care has been largely omitted from these new delivery systems. Many health systems are becoming ACOs and being certified as PCMHs. The adoption of electronic medical and dental records in many health systems creates an opportunity to bring together data from two traditionally separate systems. Information Technology (IT) integration of dental and medical records is more common as health care systems are purchasing integrated records. Therefore, the clinical integration for medical and dental interprofessional care coordination should yield financial and health outcome improvements. The goal of this article is to describe why and how dental professionals should and can participate in PCMH transitions to be a part of a Patient Centered Medical-Dental Home (PCM-DH) and ACO. This position paper provides valid reasons for developing a PCM-DH and ACO that includes dental care.
This perspective is relevant to United States healthcare system delivery models that are part of the U.S. healthcare reform legislation of 2010.
2.Accountable Care Organizations
3.Patient Centered Medical Home Initiative
4.Dental Health is Critical to Mental and Physical Health
5.Academic Health Centers
6.Conclusions
7.References
Introduction
The increasing evidence that links oral health to total physical and mental health, underscores the need to integrate dental health programs into the newly emerging transition to Patient Centered Medical Homes (PCMH) and Accountable Care Organizations (ACOs). PCMH and ACO are efforts to improve patient outcomes by creating partnerships between patients, physicians, hospitals, and other care-giving institutions to provide evidencedbased medical care, while slowing the growth of health-related costs. PCMHs, like ACOs, foster team-oriented healthcare goals around primary medical care, but unlike ACOs, focus care on the full range of cost-effective services for individuals and families from prevention and acute care to chronic disease management [1, 2]. Although primary medical care is customary in ACOs and in PCMHs, dental care has been largely omitted from these new delivery systems. The goal of this article is to describe why and how dental professionals should and can participate in PCMH transitions to be a part of a Patient Centered Medical-Dental Home (PCM-DH) and ACOs. This position paper provides valid reasons for developing a PCM-DH and ACO that includes dental care. This perspective does not directly address the traditional private dental practice in the United States.
The evidence linking oral health to physical health substantially supports the need for integrated dental care. Historically, a respectful distance has been maintained between dentistry and medicine. Despite common scientific links between the two disciplines, traditional dental and medical education has been delivered separately; medical schools provide little training in oral diseases,while only a handful of dental schools incorporate medical training into their curriculum. As a result, dentists do not consider themselves part of the chronic care model and doctors only react to oral disease from a systemic perspective [3]. This separation is reflected in the public perception that dental care is secondary to medical care and optional. The division extends to other important stakeholders such as insurers, higher levels of administrative and clinical leadership, and policy makers [4]. For instance, the current divide between medical and dental insurance makes the coordination of medical and dental services more difficult. The formation of separate sets of claims and diagnostic codes and terminologies contributes further to this division and feeds the general perception of dental care as an “optional” service [4]. In addition, insurance policies that allow either medical or dental visits but not both in one business day or just no dental coverage, further contribute to this divide.
Despite the division line between dentistry and medicine in the educational and stakeholder levels, there is an extensive body of literature, which supports the bidirectional link between oral health and overall health. This bidirectional link is best seen in the mutual relationship between diabetes and periodontitis [5, 6]. A large body of evidence supports diabetes as a risk factor in periodontal disease; furthermore, periodontitis is known to be the sixth complication of diabetes [7]. The overwhelming majority of well-controlled studies indicate an increased likelihood of periodontitis in patients with diabetes [8].
Accountable Care Organizations
The Affordable Health Care Act of 2010 chartered the Centers for Medicare and Medicaid Services (CMS) to create a demonstration program for a defined population of Medicare clients. On March 31, 2011, the U.S. Department of Health and Human Services issued proposed rules that define how to set up an ACO[9] Under these proposed rules, ACO participants are responsible for improving the quality of care according to stated benchmarks, and in return would receive a portion of any savings in cost of care generated by this new coordination of services [10]. The theory behind an ACO follows a collaborative model working for a health and health care system with better health, better care, and lower costs for all [11]. While the concept of ACOs is relatively new, programs and initiatives based on an ACO format are underway and have faced challenges [12]. We are presently at a five year review under the Affordable Care Act [13]. An example of a representative ACO, The New Hampshire Citizens Health Initiative proposed the establishment of an ACO that would focus on more collaboration between patients and physicians to create individualized treatment plans and streamlining processes to reduce costs. Rather than have accountability dispersed across a wide range of doctors, hospitals, and labs, the ACO assumes accountability for outcome and would coordinate a single payment structure [14, 15]. There are in the range of 180 ACOs serving 3 million beneficiary lives and include Pioneer ACOs (N=9), Medicare Shared Savings Program (MSSP) ACOs, and Next Generation ACO (N=18) which builds upon experiences from Pioneer and MSSP AC0s as well as additional commercial ACO models which look at alternative payment and investment options [12]. For example MSSP ACOs are groups of doctors and other health care providers who voluntarily work together with Medicare to give high quality service to Medicare Fee-for-Service beneficiaries.
An ACO is not a Medicare Advantage plan or an HMO. As part of healthcare reform, ACOs are considered health care delivery design trail blazers and risk takers [15]. The goal of an ACO is an improved health care system for the patients and the communities in which they live [12]. However, dental care is not included in these programs. We suggested that by including dental care, an ACO could benefit by reaching member patients that may not attend regular medical visits but require emergent dental care. In effect, by dental care integration, patients at high risk of chronic illness could then be referred in a coordinated system for needed medical care and thereby decrease hospitalizations.
As reported by Baxley and Stanek, in 2004, teams from U.S. teaching hospitals formed the Academic Chronic Care Collaborative (ACCC), which had the dual focus of improving the care of patients with chronic diseases (asthmas, diabetes, and COPD) and training health care teams in academic settings [16]. Using Wagner’s Chronic Care Model [17], the program goals included “evidencebased improvements, partnership with improvement-focused institutions, identification of improvement innovators practicing in academic settings, convening of these innovators and other experts to craft strategies to move the academic medical community toward better care and learning, and supporting these faculty to develop their academic careers around healthcare improvement.” The report cited a high level of enthusiasm among participating institutions with a number of benefits, such as multidisciplinary team care, better strategic planning, and enhanced diffusion of innovation across departments [16].
Patient Centered Medical Home Initiative
PCMH is an innovation in health care delivery designed to advance and achieve the Triple Aim of improved patient experience, improved population health, and reduced cost of care [11, 18]. PCMH provides primary care services of value to patients, their families, and the care teams who work with them. The evolving model promises improved access to high-quality, patient-centered primary care through relationships with patients, families, and caregivers; incorporates team-based care with clinicians and staff working at the top of their skill set; and provides cost-effective care coordination and population health management connecting patients to the “medical neighborhood” and to their community [2].
On April 11, 2016, the Centers for Medicare and Medicaid Services (CMS) announced the launch of a new advanced primary care medical home model called Comprehensive Primary Care Plus (CPC+). CPC+ is said to reward value and quality by offering an innovative payment structure to support comprehensive primary care. Part of this payment reform effort will include an effort by CMS to define and reward PCMH practices and understand which components have the greatest impact on adoption and reduction of costs while improving patient outcomes and quality of care. As a policy change announced May 27, 2016, CMS will offer an opportunity for eligible practices to participate in both the MSSP - ACOs and CPC+ [19]. In theory, through this revision, CMS will address variability in the PCMH models under the CPC+ directives using existing PCMH measures to assure better alignment with those that have the most impact. Under the Shared Savings Program, CMS assesses an ACO’s quality and financial performance based on a population of assigned beneficiaries to determine whether the ACO has met the quality performance standards and reduced growth in expenditures compared to a historical financial benchmark [20]. Yet, there is still no mention of dental care.
Dental Health is Critical to Mental and Physical Health
It should be noted however, that neither the NH Initiative nor the ACCC have dental programs within their ACO programs. While improved oral health has long been associated with improved mental health [21] and improved daily life [22, 23], the relationship between oral health and physical health has also been well established [24], and dentists could be in the front line of detecting systemic diseases.
Dentists are uniquely positioned to recognize the link between oral health, obesity, and diabetes. For instance, the daily, between meal consumption of soft drinks is strongly associated with caries development, and is strongly associated with incidence of obesity in children [25]. Within an ACO setting, the children and families could receive dietary counseling and early diabetes monitoring that is not usually provided in a dental practice.
In medically underserved populations, oral diseases not normally found in the general population such as oral candidiasis, Kaposi sarcoma, and oral hairy leukoplakia can be useful markers for AIDS diagnosis and progression [22, 23, 26, 27].
Geerts, et al., link periodontal disease as a risk factor for cardiovascular disease [28-30]. Periodontitis and diabetes appear to have a synergy whereby periodontitis is worse in poorly controlled diabetics and may decrease glycemic control even further [6, 7, 31-34].
Blue Cross Blue Shield of Massachusetts (BCBSMA) examined their patient claims data for 2009-2010 and found that members with coronary artery disease (CAD) or diabetes who had dental prophylaxis and/or periodontal treatment had a 10–15% decrease in medical costs compared to other patients who did not receive dental care (Figure 1) [35]. Their data also show that periodontal service for diabetic and CAD patients did not impact pharmacy or outpatient costs, the impact was entirely on inpatient costs.
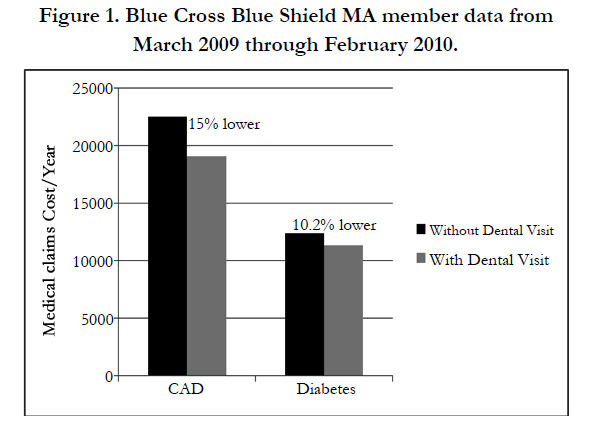
Figure 1. Blue Cross Blue Shield MA member data from March 2009 through February 2010.
In a study conducted at Montefiore Medical Center during a six month period (2012), there were 29,398 dental visits for unique patients, among whom 29.6% did not have a medical visit with in ten years and 39.2% did not have a medical visit within two years of their dental visit. Further among these dental patients ≥30 years old that had a medical visit within two years, we found that 23.65% had a diagnosis of type 2 diabetes mellitus. Patients with diabetes mellitus (DM) were more likely to be seen for dental emergency visits when compared to those without diabetes [OR of 1.2054 (95% CI: 1.0771–1.3491)] p=0.0520. We found that those with HbA1C ≥ 9 had increased dental emergency visits with an OR of 1.55 (95% CI: 1.1386-2.1042) p < 0.01. (Note: There are patients who may have received dental or medical care outside of the Montefiore healthcare system.) This study received Institutional Review Board approval and was conducted as a Performance Improvement Project. The data was derived by the use of Information Technology (IT) that bridges a gap from electronic medical and dental records using Clinical Looking Glass®, a data mining software program, and substantially demonstrates the need for care coordination.
The integration of dental care into PCMHs and ACOs would contribute to the twin goals of creating healthier populations, as well as significantly decreasing health care costs. Care coordination using multidisciplinary team care can address the patients that may arrive for dental care yet have not been seen at medical and medical providers can refer their patients to dental as they do with other care hand-offs and transitions.
Academic Health Centers
Academic Health Centers (AHC) may be uniquely poised to foster the unification of PCMHs and ACOs and creating a PCMDH. Talia, et al., argue that AHCs “should serve as the organizing entities that bring the full spectrum of health professions education, research, and care to needs of local populations”[1]. They also point out that since AHCs often exist with the context of a university system, that AHCs have significant biomedical research expertise, as well as social, political and economic resources. AHCs are in a position to bring together all of the stakeholders: patients, payers (insurance and employers), doctors, hospitals, and the community at large.
The American Hospital Association Report identified key competencies that will be required of ACOs [3]:
- Leadership
- Culture of teamwork
- Relationships with other providers
- IT infrastructure
- Infrastructure for monitoring, managing, and reporting quality
- Manage financial risk
- Receive and distribute payments or savings
- Resources for patient education and support
- Spread: identify and disseminate best practices that promote efficiency of care, improved quality of care and reduced cost
- Reach: links between ACOs and public health/community resources
- Regional health information exchange-multi-stakeholder exchange
AHCs with an established PCMH will have systems already in place that meet these competency requirements and can include dental care. Like an ACO, the PCMH system is oriented towards the whole person; the care is integrated across all aspects of the health care system and tracked by computer registries that allow for information exchange [36]. Established PCMH programs have a culture of teamwork. They have created patient education and support programs. The IT infrastructure not only supports patient registries, but also creates efficiencies in appointments, billing and payments tracking. There are systems in place for monitoring, managing and reporting performance quality [2].
Herein, we reported clinical data to support the need for integrated medical and dental care from an AHC, Montefiore Medical Center. Montefiore is an inner city academic healthcare system which provides care to a population with a heavy burden of chronic disease, has a Department of Dentistry, and has participated in interprofessional education to move towards a Patient Centered Medical and Dental Home [37]. Montefiore is further positioned to be at the forefront of integrating dental services into their successful Pioneer ACO program.
Conclusions
Academic Health Centers with established Patient Centered Medical Homes are well positioned to take a leading role in the development of Patient Centered Medical-Dental Homes and Accountable Care Organizations. Since the link of oral health to mental and physical well-being is well established, Academic Health Centers with a Department of Dentistry organized around a model of Patient Centered Medical-Dental Homes would be in a position to be the first to integrate oral health into the ACO model. This integration would allow for those patients that are at risk for chronic illness that fall between medical and dental care to receive care coordination which may well improve their overall health outcomes.
References
- Talia AF, Amenta PS, Jones SK (2010) Academic Health Centers as Accountable Care Organizations. Academic Medicine 85(5): 766-767.
- Nielsen M, Buelt L, Patel K, Nichols LM (2016) The Patient-Centered Medical Home’s Impact on Cost and Quality, Review of Evidence, 2014- 2015. The Patient-Centered Primary Care Collaborative 1-14.
- Wagner EH, Coleman K, Reid RJ, Phillips K, Abrams MK, et al., (2012) The changes involved in patient-centered medical home transformation. Prim Care 39(2): 241-259.
- Grant Makers in Health (2012) Returning the Mouth to the Body: Integrating Oral health & Primary Care. Washington, DC.
- Taylor GW (2006) Bidirectional Interrelationships between Diabetes and Periodontal Diseases: An Epidemiologic Perspective. Ann Periodontol 6(1):99-112.
- Mealey BL (2006) Periodontal disease and diabetes. A two-way street. J Am Dent Assoc 137 : 26S-31S.
- Loe H (1993) Periodontal disease. The sixth complication of diabetes mellitus. Diabetes Care 16(1): 329-334.
- Daniel R, Gokulanathan S, Shanmugasundaram N, Lakshmigandhan M, Kavin T (2012) Diabetes and Periodontal Disease. J Pharm Bioall Sci 4(2):S280-282.
- Berwick DM (2011) Launching Accountable Care Organizations--The Proposed Rule for the Medicare Shared Savings Program. N Engl J Med 364(16): e32.
- American Hospital Association (2010) Committee on Research. AHA Research Synthesis Report: Accountable Care Organization, Chicago.
- Berwick DM, Nolan TW, Whittington J (2008) The triple aim: care, health, and cost. Health Aff (Millwood). 27(3): 759-769.
- National Association of ACOs (2016) ACOs at a Crossroads: Cost, Risk and MACRA White Paper.
- Blumenthal D, Abrams M, Nuzum R (2015) The Affordable Care Act at 5 Years. N Engl J Med 373(16): 1580.
- Staples H, Porter J (2011) Accountable Care--The Overarching Vehicle for Rehabilitating Health Care--A New Hampshire Perspective. 2010.
- Citizens Health Initiative (2016) The Accountable Care Project: Transforming Systems through Shared Data and Learning.
- Baxley EG, Stanek M (2007) The AAMC Academic Chronic Care Collaborative: Family Medicine's Participation and Lessons Learned. Annuals in Family Medicine 5: 183-184.
- Wagner EH (1998) Chronic Disease Management: What Will It Take to Improve Care for Chronic Illness? Eff Clin Pract 1(1): 2-4.
- Institute for Healthcare Improvement (2014) Triple Aim Measures.
- Federal Register (2015) Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations; Final Rule. Centers for Medicare & Medicaid Services. United States Government, Washington, DC. 80:32692-32845.
- Centers for Medicare & Medicaid Services (2016) Summary of the June 2015 Final Rule Provisions for Accountable Care Organizations (ACOs) under the Medicare Shared Savings Program. The Medicare Learning Network ®, MLN Connects®, and MLN Matters®, Washington, DC.
- Coulter ID, Heslin KC, Marcus M, Hays RD, Freed J,et al., (2002) Associations of self-reported oral health with physical and mental health in a nationally representative sample of HIV persons receiving medical care.Qual Life Res 11(1): 57-70.
- Brown JB, Rosenstein D, Mullooly J, O'Keeffe Rosetti M, Robinson S, et al., (2002) Impact of Intensified Dental Care on Outcomes in Human Immunodeficiency Virus Infection. AIDS Patient Care STDS 16(10): 479-486.
- Coogan M, Greenspan J, Challacombe S (2005) Oral Lesions in Infection with Human Immunodeficiency Virus. Bull world Health Organ 83(9):700-706.
- Navazesh M, Mulligan R, Kono N, Kumar SKS., Nowicki M, et al., (2010) Oral and Systemic Health Correlates of HIV-1 Shedding in Saliva. J Dent Res 89(10): 1074–1079.
- Waldo B (2009) Oral health means more than just healthy teeth. Inside Dental Assisting.
- Hodgson TA, Naidoo S, Chidzonga M, Ramos-Gomez F, Shiboski C (2006) (A1) Identification of Oral Health Care Needs in Children and Adults, Management of Oral Diseases. Adv Dent Res 19(1): 106-117.
- Ranganathan K, Hemalatha R (2006) Oral Lesions in HIV Infection in Developing Countries: an Overview. Adv Dent Res 19(1): 63-68.
- Geerts SO, Nys M, De Mol P, Charpentier J, Albert A, et al., (2008) Systemic Release of Endotoxins Induced by Gentle Mastication: Association with Periodontitis Severity. J Periodontol 73(1): 73-79.
- Zoellner H (2011) Dental Infection and Vascular Disease. Semin Thromb Hemost 37(3): 181-192.
- de Souza AB, Okawa RT, Silva CO, Araujo MG (2016) Short-term changes on C-reactive protein (CRP) levels after non-surgical periodontal treatment in systemically healthy individuals. Clin oral investig 1-8.
- Gurav AN (2016) Management of diabolical diabetes mellitus and periodontitis nexus: Are we doing enough?. World J Diabetes 7(4): 50-66.
- Lalla E, Papapanou PN (2011) Diabetes mellitus and periodontitis: a tale of two common interrelated diseases. Nat Rev Endocrinol.. 7(12):738-748.
- Taylor GW, Burt BA, Becker MP, et al., ( 1996) Severe periodontitis and risk for poor glycemic control in patients with non-insulin-dependent diabetes mellitus. J Periodontol 67(10):1085-1093.
- Emrich LJ, Shlossman M, Genco RJ (1991) Periodontal disease in noninsulin- dependent diabetes mellitus. J Periodontol 62(2):123-131.
- Lewando R (2016) Massachusetts Oral Care 2025 Innovation/Finance/Delivery. Leadership Forum V: Oral Care 2025-A Multidisciplinary Approach 2009.
- Patient-Centered Primary Care Collaborative (2011) Joint Principles of the Patient Centered Medical Home.
- National Network for Oral Health Access (2015) A User’s Guide for Implementation of Interprofessional Oral Health Core Clinical Competencies: Results of a Pilot Project.





