A Radiographic Study of Non-Syndromic Congenitally Missing Teeth in Permanent Dentition of Nigerian Dental Patients
Yemitan TA*, Adediran VE, Ajisafe OA, Ogunbanjo BO
Faculty of Dental Surgery, Department of Child Dental Health, Orthodontic unit, Lagos State University College of Medicine, Lagos, Nigeria.
*Corresponding Author
Tolulase A Yemitan,
Faculty of Dental Surgery, Department of Child Dental Health,
Orthodontic unit, Lagos State University College of Medicine, Lagos, Nigeria.
Tel: +2348023056044
E-mail: tolulaseyemitan@yahoo.com
Received: April 24, 2016; Accepted: May 23, 2016; Published: May 27, 2016
Citation: Yemitan TA, Adediran VE, Ajisafe OA, Ogunbanjo BO (2016) A Radiographic study of Non-syndromic Congenitally Missing Teeth in Permanent Dentition of Nigerian Dental Patients. Int J Dentistry Oral Sci. 3(5), 258-263.DOI : dx.doi.org/10.19070/2377-8075-1600052
Copyright: Yemitan TA© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Congenitally missing permanent teeth was evaluated on orthopantomograms of 611 apparently healthy patients, aged 10 to 25 years at a specialist dental clinic in Lagos, Nigeria. The prevalence of congenitally missing teeth (CMT) including third molars was 7.3% in boys and 10.7% in girls, and 9.3% for both sexes combined. There were in total 57 CMT, and on average 2.1 permanent teeth were missing per child. The most commonly absent tooth was the maxillary lateral incisor (n = 22), followed by equal number of maxillary and mandibular third molars (n = 21), then mandibular second premolars (n = 19). On the other hand, no first and second molars were missing, and there were no cases with oligodontia (6 or more CMT excluding the third molar). Symmetry of CMT was predominant with 43 pairs (72.3%) of bilateral symmetry recorded. The distribution of CMT either between the maxilla and the mandible, or between the right and left quadrant did not show any significant association with sex (P > 0.05).
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.Acknowledgement and Declarations
8.References
Keywords
CMT; Hypodontia; Prevalence; Radiographic; Nigerian.
Introduction
Congenitally missing teeth (CMT) had been defined as those teeth that fail to erupt into the oral cavity and remain invisible in radiographs [1]. This could be in form of hypodontia (agenesis of one to six teeth), oligodontia (absence of six or more teeth, excluding the third molar) or anodontia (complete failure of one or both dentitions to develop [2-6]. It could be an isolated trait, or could be syndromic with an underlying recognizable clinical syndrome [7].
The prevalence of congenitally missing teeth among different population had been reported with a wide range from 0.3% to 17.1% [4, 7, 8-17]. This wide variation in the prevalence and distribution reported worldwide could be attributed to variations in age distribution of the study population, sampling techniques, methods of examination, as well as sex and racial origin of the different sample populations [10, 12, 18].
Third molars are the most commonly absent tooth in the dentition [19]. Many authors reported that the most frequently CMT after the third molar was mandibular second premolars, followed by maxillary second premolars or maxillary lateral incisors [15,20]. There were however, contrary reports which showed maxillary lateral incisors [7, 10, 14, 21, 22], mandibular incisors [9], and mandibular lateral incisors [23] as the most frequent congenitally missing teeth in their respective studies.
Few studies in Nigeria have recorded prevalence of CMT ranging from 0-3.6% [24-26]. In all these studies, the diagnosis of missing teeth was done by clinical examination and none was done using radiographs. Another author studied a syndromic population and recorded a prevalence of 63% in a group of patients with Down’s syndrome [27].
The knowledge of the prevalence and distribution of CMT will be of great value to clinicians, especially paedodontists and orthodontists, because the decision on time of commencement of treatment and treatment method will be influenced by the number and location of the congenitally missing teeth.
The purpose of this study was to determine the prevalence and distribution of congenitally missing permanent teeth including third molars in non-syndromic Nigerian dental patients.
Biological properties of bone
This retrospective cross-sectional study involved the use of 611 orthopantomograms (OPGs) of apparently healthy dental patients (364 females and 247 males) for diagnosis of CMT. These patients aged between 10 and 25 years with a mean age of 15.72 ± 4.69 years at the time the OPGs were taken, had visited at a specialist dental clinic in Lagos, Nigeria, between December 2013 and September 2014. This study was carried out with approval from the Research and Ethics committee of the Lagos State University Teaching Hospital.
To ensure racial homogeneity, all selected radiographs were those of Nigerian subjects. The orthopantomograms were taken on Planmeca ProMax (Planmeca USA Inc, IL, USA) at an exposure of 68KV, 13.0mA and 15.8s. Faulty radiographs with unclear or altered morphology of the teeth were excluded. Patients with a history of tooth extraction, developmental or hereditary disorders, bone defects, trauma, and fractures were excluded from study. Patients with systemic conditions, especially cleft lip and palate, Down’s syndrome, and other syndromes were excluded.
All radiographs were analyzed by one investigator in a dark room using an x-ray viewer (Slim-Line™ View Box, Select Dental Manufacturing Inc, NY, USA). A tooth was diagnosed as congenitally missing when it could not be identified or discerned radiographically on the basis of calcification and there was no evidence of extraction [28]. All cases diagnosed as CMT was reassessed 2 weeks later to confirm diagnosis of CMT.
To calculate intra-observer agreement, a set of 30 OPGs of CMT cases chosen at random were examined by the same examiner four weeks after the initial examination and intra-examiner reliability was calculated by correlation coefficient (r = 0.96, P <0.001).
Statistical analyses of data were performed using Statistical Package for Social Sciences program (SPSS, version 21.0, Chicago, IL, USA). The Pearsons Chi-square test was used to determine the significance of the differences between CMT for maxilla and mandible in the right and left quadrant for boys and girls. It was tested at the 5% level of significance.
Results
The study consisted of 59.6% female and 40.4% male patients with no statistically significant difference between the females (16.11 ± 4.7 years) and males (15.14 ± 4.6 years) according to chronological ages [Table 1].
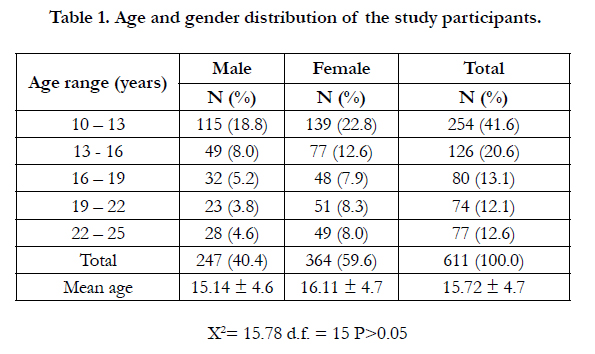

Table 1. Age and gender distribution of the study participants.
Including third molars, a total of 119 permanent teeth were congenitally missing, 40 (33.6%) in males and 79 (66.4%) in females with an average of 2.1 congenitally missing teeth per person. The distribution of hypodontia was shown in Figure 1.
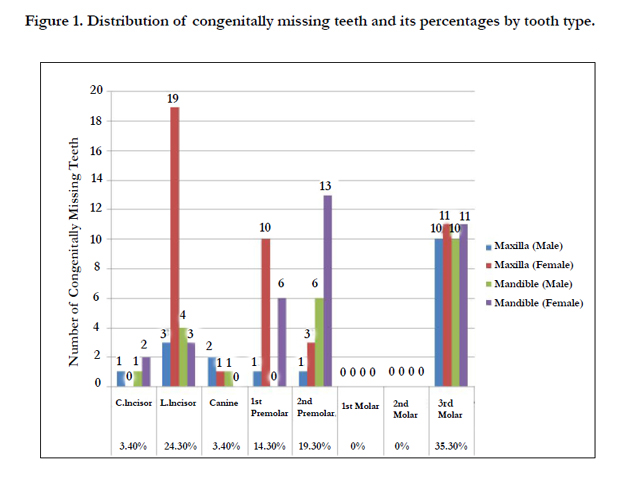
Figure 1. Distribution of congenitally missing teeth and its percentages by tooth type.
The prevalence of CMT was higher but not significantly in females (10.7%) than in males (7.3%), and for both sexes 9.3% (Table 2).
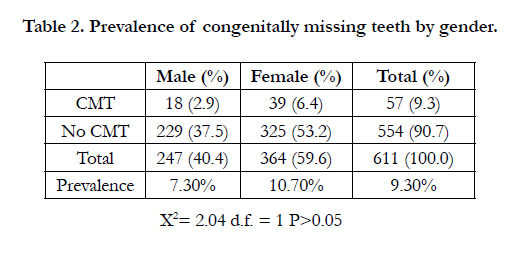
Table 2. Prevalence of congenitally missing teeth by gender.
The number of CMT per child ranged from 1 to 5 in this study. Most of the children (73,7%) had hypodontia of either one or two teeth (Table 3).
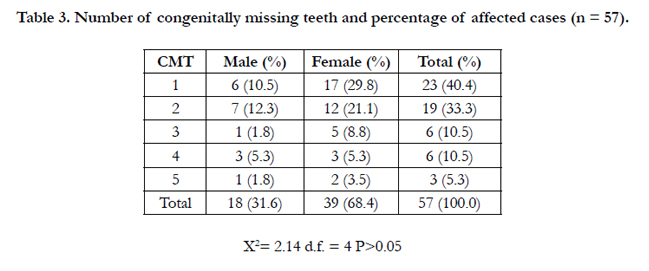
Table 3. Number of congenitally missing teeth and percentage of affected cases (n = 57).
The rate of CMT was higher in the maxilla (52.1%, n=62) than in the mandible (47.9%, n=57) and there were more on the left side (51.3%, n=61) than on the right (48.7%, n=58), although there were no significant association (Table 4).
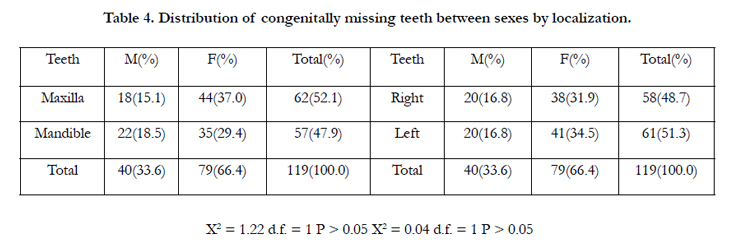
Table 4. Distribution of congenitally missing teeth between sexes by localization.
The most commonly missing teeth were the maxillary lateral incisors (18.4%, n=22) followed by maxillary and mandibular third molars in equal numbers (17.65%, n=21), then mandibular second premolars (15.9%, n=19) and maxillary first premolars (9.3%, n=11). On the other hand, maxillary and mandibular first and second molars were never absent (Figure 1). Symmetrical hypodontia was predominant, accounted for 43 pairs representing 72.3% of all the CMT, while the CMT located unilaterally had the right and left side affected almost equally. The most common tooth affected by bilateral hypodontia was the maxillary third molars, followed by mandibular third molars, maxillary lateral incisors, and mandibular second premolars (Table 5).
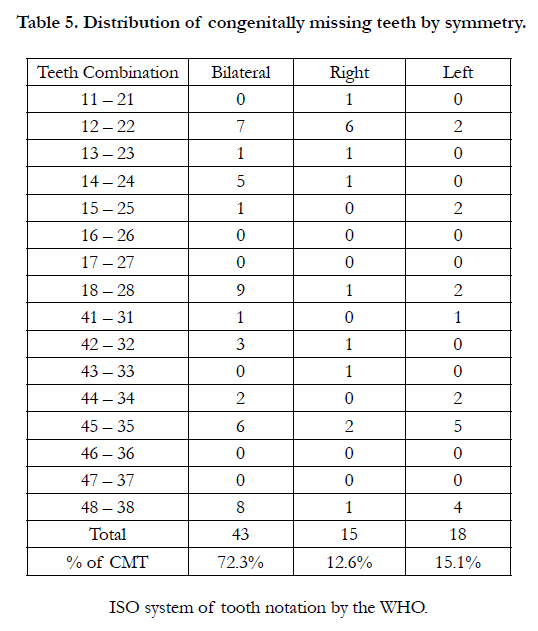
Table 5. Distribution of congenitally missing teeth by symmetry.
Discussion
Radiograghic examination is essential in the diagnosis of CMT as by definition, CMT are those that fail to erupt in the oral cavity and remain invisible in radiographs [29]. Clinical examination tend to result in underestimation of CMT in comparison with radiographic examination [11, 18, 30, 31].
Although asymptomatic in most cases, CMT can result in aesthetic and functional problems in addition to causing malocclusion and psychological problems. Drifting of teeth adjacent to site of CMT, midline shift, alveolar bone resorption as well as problems with mastication and occlusion are a few of the resulting complications [22, 32].
In this survey the third molar was included even though some authors [9, 28, 33, 34] excluded third molar in their investigation. All permanent tooth crowns except the third molars have begun their mineralization by age of six. Usually at the age of 8 to 10 years the first sign of the third molar appeared on the radiograph, but occasionally on older age. Therefore, the diagnosis of congenitally missing tooth in permanent dentition should be made after the age of 6 years if third molars were excluded, and by 10 years of age if third molars were also studied [20]. The youngest patient in this study was 10 years of age (Table 1), therefore all the patients were suitable as sample in this study according to age.
The prevalence of CMT in this study was 7.3% in boys and 10.7% in girls, and for both sexes combined it was 9.3% (Table 2), which is similar to that reported by previous study of a Japanese population [15]. Also, a high average of 2.1 CMT per patient suggests that CMT is not an uncommon condition in Nigeria. It is however higher than previously reported range of 0 – 3.6% in Nigerians [24-26]. Also, several reports from different racial populations reported prevalence of CMT ranging from 2.7% to 4.19% [13, 14, 16, 20, 21]. These differences could be due to variation in sampling techniques, methods of examination, as well as sex, age distribution and racial origin of the different sample populations. A higher CMT prevalence of 17.11% [17] and 14.69% [4] recorded among orthodontic patients may be because of a greater tendency for people with dental anomalies to seek orthodontic treatment. It may also be as a result of routine use of OPG investigation prior to orthodontic treatment.
In this and other studies [2, 14, 15, 28] there was no significant difference in CMT between males and females although some studies reported a higher tendency for females to have this anomaly [9-11], while a study found a higher occurrence of hypodontia in males than in females [12] (Table 6).
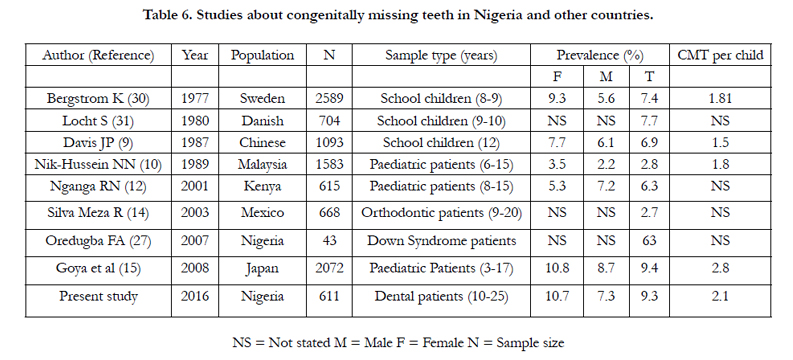
Table 6. Studies about congenitally missing teeth in Nigeria and other countries.
The present study and other studies [2, 9-11, 13, 15, 18, 28-30] indicate that hypodontia involving one or two teeth represents a wide majority of cases, being 73.7% in this study (Table 3). This suggests that most cases of CMT are relatively mild.
In agreement with other studies [14, 22, 35], the frequency of CMT was higher in the maxilla than in the mandible, although the difference was not significant (Table 4). Other studies [2, 5, 10, 15, 18] however reported higher prevalence of CMT in the mandible than in the maxilla though the difference was not significant.
This study is in agreement with previous investigations [12, 14, 15, 21, 28, 36] that reported that symmetrical hypodontia was more prevalent than unilateral hypodontia (Table 5). The frequency of bilateral CMT in this study was 72.3% of CMT, which is in accord with previous reports of 75% [14], 60% [30], and 74.6% [15] in a Mexican, Norwegian, and Japanese population respectively. This suggests a strong genetic association.
This study concurs with reports that indicated that the first molars are never absent [10, 11, 31]. It also agrees with reports that the maxillary central incisors, mandibular canines and second molars were rarely missing in hypodontia [2, 5, 11, 28, 29, 37, 39]. In the present study, the least affected teeth were maxillary central incisor, mandibular canines, and maxillary and mandibular first and second permanent molars (Figure 1). While some studies reported that the mandibular second premolars were most commonly missing teeth [15, 20, 28, 30, 31], others showed that maxillary lateral incisor was the most prevalence missing tooth in individuals with agenesis of only one or two teeth [7, 10, 14, 21, 22]. The most affected teeth in this study were maxillary lateral incisors, followed by maxillary and mandibular third molars, and mandibular second premolars.
Hydodontia appears to be an inherited characteristic, although the precise genetic mechanism responsible is not completely understood [10]. One explanation considered was that congenitally missing teeth, except for hereditary cases, has a greater likelihood of occurrence when the dental germ is developed later than the surrounding tissues, thus reducing the space available for the tooth to develop [15]. Also, previous studies demonstrated a highly significant correlation between microdontia and advanced CMT of the permanent dentition [5, 6, 41]. Both of these suggestions agreed with Bolk’s theory of terminal reduction [42] that reduction of the distal element of a tooth group occurs more frequently than in mesially placed teeth, due to the phylogenetic evolution of humans. Therefore, the teeth most often missing are the maxillary lateral incisors, second premolars, and the third molars, as observed in the present study.
Dental agenesis may also arise as a result of combined effect of genetic and environmental factors [33, 43]. These include infection, trauma, drugs, and genes associated with syndromes such as cleft lip, cleft palate, or both [44], ectodermal dysplasia [45], or Down syndrome [46].
There are evidently some limitations to the study of congenitally missing teeth. The first is that the visibility of tooth germs on radiographs depends on their stage of mineralization. Subjects of the same chronologic age may show major differences in mineralization stage and dental age. Tooth buds showing late onset of mineralization could lead to a false positive diagnosis of agenesis on radiographs [2]. Therefore, diagnosis of tooth agenesis should be made after the age of 6 years, if third molar is excluded, and after 10 years af age if the third molar is also studied [15, 20]. On the basis of this criterion, the age of inclusion in this study was set at 10 years.
Secondly, there may be difficulty in distinguishing between a central and lateral incisor, especially when the remaining teeth have drifted. This may result in misclassification. Also, superimposition of cervical vertebrae in the mental region of the mandible may result in artifact which may cause problems of identification. The re-examination of the radiographs helped to identify those cases where teeth may have been misclassified. Thus a definitive list of study participants was only derived after the revision.
Missing teeth are asymptomatic in most cases, but they may lead to some clinical problems, including malocclusion, aesthetic problems, functional difficulties, and psychological problems. All cases should be evaluated by interdisciplinary approach for appropriate treatment choices which may be by orthodontic approach or by prosthetic replacement. Therefore, early diagnosis and treatment planning by clinicians should be made for appropriate treatment modalities in order to minimize the complications of this anomaly.
Conclusion
The maxillary lateral incisor was the most frequent CMT and the first and second permanent molars were the most stable teeth. Most cases involve CMT of one or two missing teeth. There were no significant differences in the distribution of CMT between sexes or in localization by arches and quadrant sides. Symmetrical hypodontia was however predominant. These results could provide a template for use in future investigations of variation of tooth number, and also in anthropological studies in Nigerians.
Acknowledgement and Declarations
The study was funded by the authors.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
- Jorgenson RJ (1980) Clinician's view of hypodontia. J Am Dent Assoc 101(2): 283-286.
- Polder BJ, Van't Hof MA, Van der Linden FPGM, Kuijpers-Jagtman AM (2004) A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol 32(3): 217-226.
- Nordgarden H, Jensen JL, Storhaug K (2002) Reported prevalence of congenitally missing teeth in two Norwegian counties. Community Dent Health 19(4): 258-261.
- Gabris K, Fábián G, Kaán M, Rózsa N, Tarján I (2006) Prevalence of hypodontia and hyperdontia in paedodontic and orthodontic patients in Budapest. Community Dent Health 23(2): 80-82.
- Schalk-van der Weide Y, Steen WH, Bosman F (1992) Distribution of missing teeth and tooth morphology in patients with oligodontia. ASDC J Dent Child 59(2): 133-140.
- Schalk-van der Weide Y, Steen WH, Bosman F (1993) Taurodontism and length of teeth in patients with oligodontia. J Oral Rehabil 20(4): 401-412.
- Vahid-Dastjerdi E, Borzabadi-Farahani A, Mahdian M, Amini N (2010) Non-syndromic hypodontia in an Iranian orthodontic population. J Oral Sci 52(3): 455-461.
- Rosenzweig KA, Garbarski D (1965) Numerical aberrations in the permanent teeth of grade school children in Jerusalem. Am J Phys Anthropol 23(3): 277-283.
- Davis PJ (1987) Hypodontia and hyperdontia of permanent teeth in Hong Kong schoolchildren. Community Dent Oral Epidemiol 15(4): 218-220.
- Nik-Hussein NN (1989) Hypodontia in the permanent dentition: a study of its prevalence in Malaysian children. Aust Orthod J 11(2): 93-95.
- Aasheim B, Ögaard B (1993) Hypodontia in 9-year-old Norwegians related to need of orthodontic treatment. Scand J Dent Res 101(5): 257-260.
- Ng’ang’a RN, Ng’ang’a PM (2001) Hypodontia of permanent teeth in a Kenyan population. East Afr Med J 78(4): 200-203.
- Osuji OO, Hardie J (2002) Dental anomalies in a population of Saudi Arabian children in Tabuk. Saudi Dent J 14(1): 11-14.
- Silva Meza R (2003) Radiographic assessment of congenitally missing teeth in orthodontic patients. Int J Paediatr Dent 13(2): 112-116.
- Goya HA, Tanaka S, Maeda T, Akimoto Y (2008) An orthopantomographic study of hypodontia in permanent teeth of Japanese paediatric patients. J Oral Sci 50(2): 143-150.
- Gupta SK, Saxena P, Jain S, Jain D (2011) Prevalence and distribution of selected developmental dental anomalies in an Indian population. J Oral Sci 53(2): 231-238.
- Trakiniene G, Ryliškyte M, Kiaušaite A (2013) Prevalence of teeth number anomalies in orthodontic patients. Stomatologija 15(2): 47-53.
- Wisth PJ, Thunold K, Böe OE (1974) Frequency of hypodontia in relation to tooth size and dental arch width. Acta Odontol Scand 32(3): 201-206.
- Matalova E, Fleischmannova J, Sharpe PT, Tucker AS (2008) Tooth agenesis: from molecular genetics to molecular dentistry. J Dent Res 87(7): 617-623.
- Rahardjo P (2006) Prevalence of hypodontia in chinese orthodontic patients. Dent J (Maj. Ked. Gigi) 39: 147-150.
- Karadas M, Celikoglu M, Akdag MS (2014) Evaluation of tooth number anomalies in a subpopulation of the North-East of Turkey. Eur J Dent 8(3): 337-341.
- Peker I, Kaya E, Darendeliler-Yaman S (2009) Clinical and radiographical evaluation of non-syndromichypodontia and hyperdontia in permanent dentition. Med Oral Patol Oral Cir Bucal 14(8): e393-397.
- Niswander JD, Sujaku C (1963) Congenital anomalies of teeth in Japanese children. Am J of Phys Anthropol 21(4): 569-574.
- Onyeaso CO, Oneyeaso AO (2006) Occlusal/dental anomalies found in a random sample of Nigerian schoolchildren. Oral Health Prev Dent 4(3): 181-186.
- Ajayi EO (2008) Prevalence of malocclusion among school children in Benin City, Nigeria. J Med Biomed Res 7(1-2): 1-8.
- Temilola DO, Folayan MO, Fatusi O, Chukwumah NM, Onyejaka N, et al. (2014) The prevalence, pattern and clinical presentation of developmental dental hard-tissue anomalies in children with primary and mix dentition from Ile-Ife, Nigeria. BMC Oral Health 14: 125.
- Oredugba F (2007) Oral health condition and treatment needs of a group of Nigerian individuals with Down syndrome. Down Syndrome Res Pract 12(1): 72-76.
- Endo T, Ozoe R, Kubota M, Akiyama M, Shimooka S (2006) A survey of hypodontia in Japanese orthodontics patients. Am J Orthod Dentofacial Orthop 129(1): 29-35.
- Pemberton TJ, Das P, Patel PI (2005) Hypodontia: genetics and future perspectives. Braz J Oral Sci 4(3): 695-706.
- Bergström K (1977) An orthopantomographic study of hypodontia, supernumeraries and other anomalies in school children between the ages 8-9 years, an epidemiological study. Swed Dent J 1(4): 145-157.
- Locht S (1980) Panoramic radiographic examination of 704 Danish children aged 9-10 years. Community Dent Oral Epidemiol 8(7): 375-380.
- Ajami B, Shabzendedar M, Afzal A, Mehrjerdian M(2010) Prevalence and pattern of Congenital Missing teeth in a group of Iranian adolescents. Shiraz Univ Dent J 10 suppl: 40-44.
- Backman B, Wahlin YB (2001) Variation in number and morphology of permanent teeth in 7-year-old Swedish children. Int J Pediatric Dent 11(1):11–17.
- Steffen W, Rohling J, Bauss O (2006) Prevalence of symptoms of disturbed development of the dentition. J Dent Oral Med 8(1): 307.
- Altug-Atac AT, Erdem D (2007) Prevalence and distribution of dental anomalies in orthodontic patients. Am J Orthod Dentofacial Orthop 131(4): 510-514.
- Rolling S (1980) Hypodontia of permanent teeth in Danish schoolchildren. Scand J Dent Res 88(5): 365-369.
- Dhanrajani PJ (2002) Hypodontia: etiology, clinical features, and management. Quintessence Int 33(4): 294-302.
- Zarrinnia K, Bassiouny MA (2003) Combined aplasia of maxillary first molars and lateral incisors: a case report and management. J Clin Pediatr Dent27(2): 127-131.
- Kirzioğlu Z, Köseler Sentut T, Ozay Ertürk MS, Karayilmaz H (2005) Clinical features of hypodontia and associated dental anomalies: a retrospective study. Oral Dis 11(6): 399-404.
- Niswander JD, Sujaku C (1963) Congenital anomalies of teeth in Japanese children. Am J Phys Anthropol 21(4): 569-574.
- Rune B, Sarnäs KV (1974) Toothsize and tooth formation in children with advanced hypodontia. Angle Orthod 44(4): 316-321.
- de Beer GR (1951) Embryo and ancestors. Clarendon Press, Oxford, 58-59.
- Amini F, Rakhshan V, Babaei P (2012) Prevalence and pattern of hypodontia in the permanent dentition of 3374 Iranian orthodontic patients. Dent Res J 9(3): 245–250.
- Shapira Y, Lubit E, Kuftinec MM (2000) Hypodontia in children with various types of clefts. Angle Orthod 70(1): 16-21.
- Markovic M (1982) Hypodontia in twins. Swed Dent J Suppl 15: 153-162.
- Fekonja A (2005) Hypodontia in orthodontically treated children. Eur J Orthod 27(5): 457-460.





