Bone Graft Substitutes for Bone Defect Regeneration. A Collective Review
M Kheirallah1*, H Almeshaly2
1 Department of Maxillofacial Surgery, College of Dentistry, Alanadalos University for Medical Sciences, Al-Qadmous, Syria.
2 Postgraduate student in Dental Sciences, College of Dental Medicine, Majmaah University, Kingdom of Saudi Arabia.
*Corresponding Author
Mouetaz Kheirallah, DDS, OMFS, PhD
Department of Maxillofacial Surgery, College of Dentistry,
Alanadalos University for Medical Sciences, Al-Qadmous, Syria.
Tel: +963 43 657600
Email: m.kheirallah@mu.edu.sa , moutazkheirallah@gmail.com
Received: March 07, 2016; Accepted: May 03 2016; Published: May 16, 2016
Citation: M Kheirallah, H Almeshaly (2016) Bone Graft Substitutes for Bone Defect Regeneration. A Collective Review. Int J Dentistry Oral Sci. 03(5), 247-255.DOI : dx.doi.org/10.19070/2377-8075-1600051
Copyright: M Kheirallah© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: The purpose of this review article is to illustrate the current state of development of bone graft substitutes that could be used for bone defect regeneration, as well as to analyze their efficacy for clinical use.
Methods: An electronic search of the PubMed, was performed for articles written in English. The focused question was “ideal graft substitute material to choose in clinical practice”?. The searches were limited to articles including: bone graft, bone defect scaffold, bone substitutes, and bone regeneration. An attempt was made to identify clinical studies. During the data
collection, the data were extracted from the studies including scaffold material, properties and advantages of bone substitutes,
as well as clinical results if the study has been provided clinically.
Results: In spite of several acceptable scaffold options available for bone regeneration, these options still need to bridge the
gap between research and clinical practice. There is little information available about the cellular basis for bone regeneration
in humans. Several problems limit the broad usage of such options, including lack of randomized controlled human studies,
and dubious long term results.
Conclusion: The studies should be nurtured and monitored by a combination of clinical experience. Future trends may focus
on the effective combinations of osteoinductive materials, osteoinductive growth factors and cell-based tissue regeneration
tactics using composite carriers. There is no single ideal graft material to choose in clinical practice, therefore researches are
ongoing in all relevant fields, to establish modern bone regeneration protocols that may lead to the innovation of ideal graft
substitutes.
2.Introduction
3.Biological properties of bone
4.Bone grafts into the recipient site
5.Bone graft substitutes
6.Scaffolds and bone substitutes
6.1.Polymers scaffolds
6.2.Ceramic scaffolds
6.3.Metallic and Composite scaffolds
7.Results
8.Conclusion
9.References
Keywords
Bone graft, Scaffold Bone Defect, Bone Substitutes, Bone Regeneration.
Introduction
Bone is the second most transplanted tissue in the body [1, 2], with approximately 3.5 million bone graft procedures performed each year [3]. There are many cases in which bone grafts are needed in large quantity such as for reconstruction of large bone defects caused by trauma, tumors, infections, and congenital defects, and also in cases where the regeneration is compromised (osteoporosis, necrosis and atrophic non-unions) [4, 5]. All these facts emphasis that, large bone defects are still a challenge for maxillofacial surgeons.
Generally four elements are needed of bone grafts for bone regeneration: Osteoconduction, osteoinduction, osteointegration, and osteogenesis [6, 7]. Osteoconduction is the ability to support bone growth on a surgical site, during which pores, channels, and blood-vessels are formed within bone. Osteoblasts from the margin of the defect that is being grafted utilize the bone graft material as a framework upon which to spread and generate new bone. Osteoinduction involves the stimulation of osteoprogenitor cells to differentiate into osteoblasts that then begin new bone formation. The most widely studied type of osteoinductive cell mediators are bone morphogenetic proteins (BMPs) [8]. A bone graft material that is osteoconductive and osteoinductive will not only serve as a scaffold for currently existing osteoblasts but will also trigger the formation of new osteoblasts. Osteointegration is the direct contact of living bone to graft material [9]. Finally osteogenesis is the formation of new bone by osteoblasts within the graft material[5-7].
There are three main types of bone grafts, autografts, allografts and bone graft substitutes [5]. The autograft is considered as the standard in bone grafts. The ilium is the most frequent donor site accounting for one-third of all cases [10]. However, its use is limited by complications such as pain, additional operating time, infection, scarring, blood loss, and donor site morbidity [10, 11].
Allograft from cadavers or living donors is the most commonly used alternative to autografts [12]. The main advantage of allografts is increased availability in various shapes and sizes and the avoidance of donor-site morbidity [6]. On the other hand they have no viable cells to offer osteogenic properties, which may result in incomplete integration with the host tissue [13]. They lack the osteogenic capacity of autografts and carry the risk of infectious agents or immune rejection [14]. Both types of the bone graft options come with inherent limitations; which has led to the need for the development of new bone graft substitutes. Substitute materials are advantageous because of their unlimited availability but unfortunately they lack both osteoinductive and osteogenic properties, so suffer from poor integration and eventual mechanical failure [5, 13]. Therefore, the next generation of bone graft substitutes must be developed. Using tissue engineering techniques, it is possible to design new scaffolds aiming to decrease the disadvantages of traditional grafts and improve graft integration, osteogenicity, osteoconductivity, and osteoinductivity. The aim of this review article is to illustrate the current state of development of these substitutes that could be used as alternative for their application in bone defect regeneration, as well as to analyze their efficacy for clinical use.
Biological properties of bone
Proceeding from the need of bone graft substitutes, the field of tissue engineering seeks to address this need using different aspects of medicine, biology, and material science. However, before a suitable bone tissue replacement can be engineered, the biological properties of the bone must be better understood.
Bone tissue consists of bone extracellular matrix and bone cells, extracellular matrix is comprised of both organic and inorganic components [15]. The organic components are formed of type- I collagen fibrils, osteopontin and osteocalcin. Within the bone extracellular matrix, osteopontin is known to promote cell attachment through covalent binding with fibronectin and type I collagen. Both osteopontin and osteocalcin have an alliance with calcium and may support the nucleation of calcium phosphate during mineralization [16]. The inorganic components of the matrix are calcium, carbonate, and phosphate ions, arranged in a crystalline-like structure. Matrix mineralization starts with nucleation of calcium phosphate crystals, and followed by crystal growth [17]. Non-collagenous proteins can be nucleation points for crystallization [18]. There are three types of bone cells in bone tissue: osteoblasts, osteoclasts, and osteocytes. Osteoblasts are responsible for bone formation through the synthesis and secretion of an organic extracellular matrix, and also synthesize a variety of growth factors including transforming growth factor-β (TGF-β) and bone morphogenic proteins (BMPs) that can aid in both the recruitment and differentiation of stem cells [15]. When matrix is no longer actively being formed, the osteoblasts become embedded within the extracellular matrix and become osteocytes. Osteoclasts are responsible for bone resorption [19]. Communication between the three types of bone cells regulate the formation and resorption of bone.
Bone grafts into the recipient site
It is known that an ideal bone graft should have osteogenesis,osteoinductivity, osteoconductivity, and osseointegration characcharacteristics
[1, 20, 21]. Therefore it is important to understand the mechanism of action for each graft. Bone grafts are used to bridge a critical size bone defect, they become incorporated into the recipient site. Incorporation of the bone graft involves two essential steps: (1) the union between the edges of the graft with the edges of native bone segments, (2) gradual resorption of the graft, associated with its replacement by new bone [22-24]. The space occupied by that the graft should ultimately turn into viable bone and permanently accessible to the physiological remodeling mechanisms. This process is typically very slow, and cannot always be accomplished. There are many factors which regulate the incorporation process, these factors may be relevant to the type of graft, it porosity, recipient site, and the graft - bone interface. Incorporation is better in autogenous grafts, because of their porous nature, which allow easy vascular and cellular invasion. The graft structure has a large surface area that is covered by osteoblasts, making it osteoconductive and osteogenic, also through the extensive vascular invasion, the bone matrix can be demineralized and its proteins exposed through the actions of osteoclasts. Lack of integration between the graft and adjacent bone segments, makes the process slow and rarely complete [22]. Finally, graft incorporation can be summed up into five main steps [2]: (1) hematoma formation, release of bone inducing factors and cellular recruitment, (2) inflammation and development of fibro-vascular tissue, connecting the graft to the adjacent bone, (3) vascular invasion of the graft, (4) focal resorption of the graft by recruited osteoclasts, (5) new bone formation, union between the graft and the surrounding bone, and graft remodeling.
Bone graft substitutes
Selection of bone graft substitutes should be based on its characteristics and properties of the biomaterials, which include mechanical, chemical, toxicological, and morphological properties. The overall success is based on tissue compatibility of a biomaterial, as well as the nature, degree, frequency, and its constituents to the intended tissues into which it will be utilized. During the few last years, studies have been focused on the optimal scaffold design which changed the requirements and properties of the biomaterials used. Since 2002, Hench has defined three different generations [25], starting with the earliest and following the order in which they occurred. First generation of bone graft substitutes desired to match the biomaterial with the physical properties of the tissue to be replaced, while maintaining inertia with the immediate small-scale environment of the tissue. This generation contains metals (stainless steel, titanium), alloys (alumina, zirconia), and polymers (silicone, polypropylene, polymethylmethacrylate). A common manifestation for this generation is the formulation of fibrous tissue at the tissue graft interface that would finally enclose the graft then leading to loosening. The material cannot be phagocytosed since it is encapsulated by fibrous connective tissue, isolating it from the surrounding tissues [26]. In order to avoid the formation of this fibrous layer and improve osseointegration, tissue engineering has developed the second generation of bone graft substitutes, by covering the biomaterial with hydroxyapatite, Beta-tricalcium phosphate, or bioactive glass. This generation used synthetic or natural polymers to stimulate a controlled chemical slump, leading to passive products which can be resorbed [27]. Third generation of bone graft substitutes have been developed, to get material nearer to the autograft, using patient material which induces, at molecular level, cellular response by combination of the bioactivity and biodegradability of second generation devices. This generation has been founded on the notion of bone tissue engineering which lead to creation of a device that support bone regeneration through the cooperation between bone osteoprogenitor cells and growth factors (natural components) for stimulation of cells into a scaffold made of various natural or synthetic biomaterials [28].
Tissue engineering has established specific scaffold properties, which guarantee biocompatibility, porosity, Micro & Nano scale structure, rate of degradation , and growth factor delivery [29]. Biocompatibility is linked to a scaffold material which does not formulate undesirable local or systemic responses [30]. Porosity is related to interconnectivity, this means that it improve osteogenesis. A highly porous scaffold expedites cell husbandry and migration, while smaller pores allow tissue ingrowth [14]. Although the mechanical strength of the scaffold decreases with porosity, this estimation should be tied with the mechanical needs of the bone tissue which have to be replaced. Also pores promote the diffusion from and to the scaffold and simplify vascularization [14]. Micro & Nano scale structure promote cell functions leading to improved osteoinduction and osseointegration [31]. The proportion of degradation of the scaffold must stay tuned to stock the structure until the new bone has adequate mechanical strength [32]. Lack of this state, may lead to the scaffold fracture after a mechanical loading, before the completion of bone healing process. Delivery of growth factors such as transforming growth factorβ (TGFβ), insulinlike growth factors (IGF), platelet derived growth factors (PDGF), and bone morphogenetic proteins (BMP), increase the potential of osteoprogenitor and osteoblast functions to enhance bone growth by encouraging MSCs to migrate into the scaffold, proliferate, differentiate, and begin extracellular matrix production [33]. There are many techniques to deliver these growth factors such as controlled release from biodegradable scaffolds, osmotic pumps, bolus injection, and surface adsorbed protein release. The confrontation of these techniques is a short half-life which leads to loss of their bioactivity, in addition to restrictive control of administered dose.
Scaffolds and bone substitutes
A wide variety of biomaterials are currently used as scaffolds, in modern clinical practice, including collagen, hydroxyapatite (HA), β-tricalcium phosphate (β-TCP), calcium-phosphate, and glass ceramics [34, 35]. Bone substitutes can be defined as “a synthetic, inorganic or biologically organic combination biomaterial which can be inserted for the treatment of a bone defect instead of autogenous or allogenous bone” [36]. In the past, inoperative scaffolds have been used as space possessors during the restoration processes. Currently no one single scaffold can display osteoinductive, osteogenic, promote vascularisation and has suitable mechanical properties. Subsequently, the challenge is to form a scaffold with biologically active molecules, living cells, and promote the regeneration of bones. Currently used scaffold biomaterials can be classified into different groups:
Polymer materials are divided into natural polymers and synthetic polymers. Natural polymers, have likable properties, and facilitate the addition of chemicals, proteins, peptides, and cells to scaffolds texture. In addition, the porosity and mechanical strength can be controlled by inconstant polymer concentrations.
The most widely studied of natural polymers are collagen/gelatin, chitosan, silk, alginate, hyaluronic acid, and peptides (Table 1). Collagen can be isolated from animal tissues [37], it is characterized by biodegradability, biocompatibility and bioreabsorbability, also it has low antigenicity and ability of being crosslinked [38, 39], but it is difficult to control the rate of degradability [40]. Scaffold properties can be modified by using various concentrations of collagen [41]. Collagen is the main protein of the extracellular matrix, provides support to connective tissues such as skin, bones , blood vessels, and ligaments [42, 43], so collagen sponges have been used for the treatment of long bone fractures (Collagraft®) [44]. Yannas et al. has inspected, collagen scaffold in dermal regeneration process [45]. Kohara and Tabata induced bone formation by using gelatin sponges with bone morphogenetic proteins, also concluded that the use of gelatin scaffold mixed with multiple osteoinductive agents could be active to induce bone formation [46].
The synthetic polymers contain polyesters, polyanhydride, polyorthoester and polycaprolactone. The most commonly used synthetic polymers are the polyesters such as poly glycolic acid, poly lactic acid, and their copolymer of poly lactic-co-glycolic acid (Table 2). These polymers lack the desired bioactivity as documented by Holzwarth and Ma [47]. However they have the ability to be converted into specific material with chemical and mechanical properties needed for the required application [48-50]. Although synthetic polymer has shown clinical outcomes comparable to autograft, it was found to be connected with bad incorporation and biodegradation forms [51, 52]. Synthetic polymer implements poorly on radiographic estimation with elevated rates of graft breakdown, nonunion, displacement, and even as a spacer is debatable [53-55]. However since both the polymers (natural and synthetic) have certain advantages, a combination of them can be used to produce composite scaffolds with safely better biological and mechanical properties. Yang combined polycaprolactone with chitosan to create bioactive nanofibers [56]. This new hybrid scaffold takes advantage of the physical properties of the synthetic polymer and the bioactivity of the natural polymer while minimizing the disadvantages of both. A collagen and poly lactic acid scaffold with parallel collagen fibres embedded within a PLA matrix has been fabricated by Dunn et al. They suggested that resorbable polymeric composite scaffolds are potentially useful for reconstruction of the anterior cruciate ligament of the knee [57].
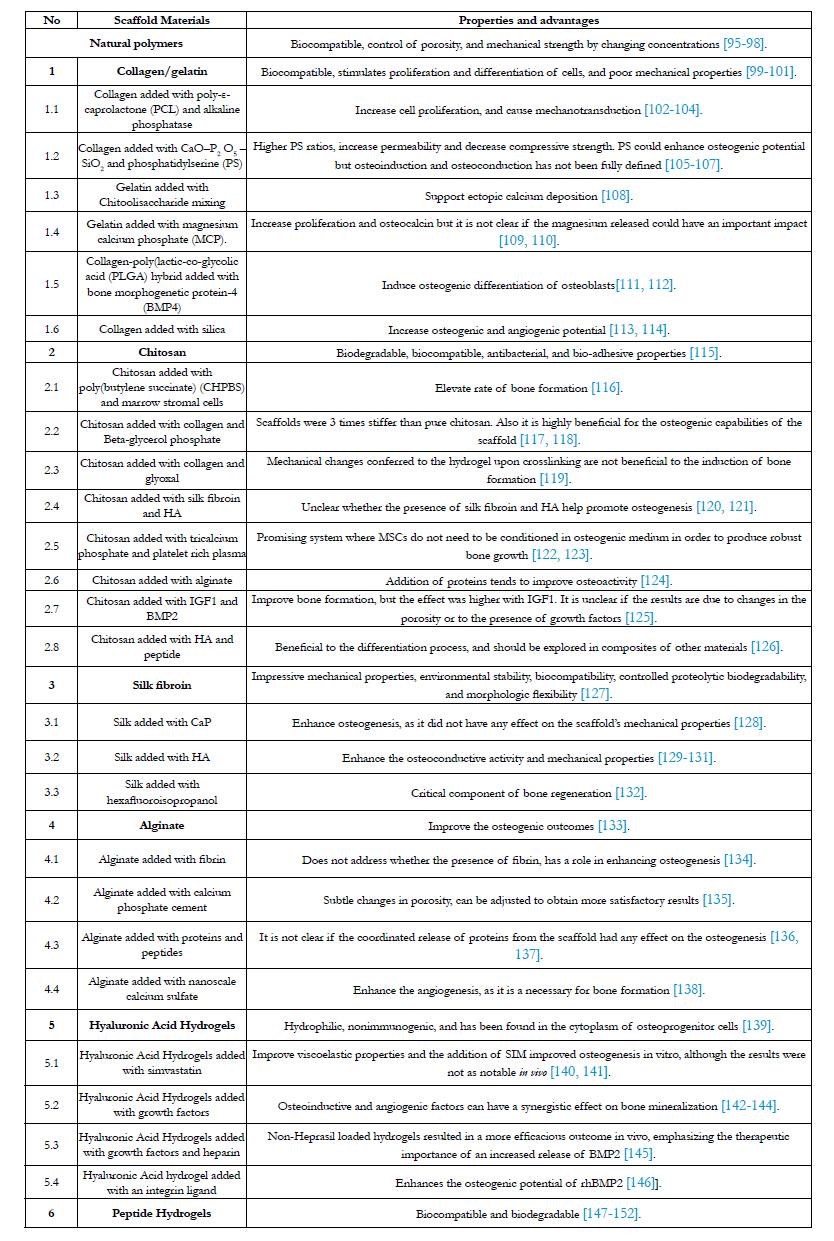

Table 1. Properties and advantages for natural polymers scaffolds.
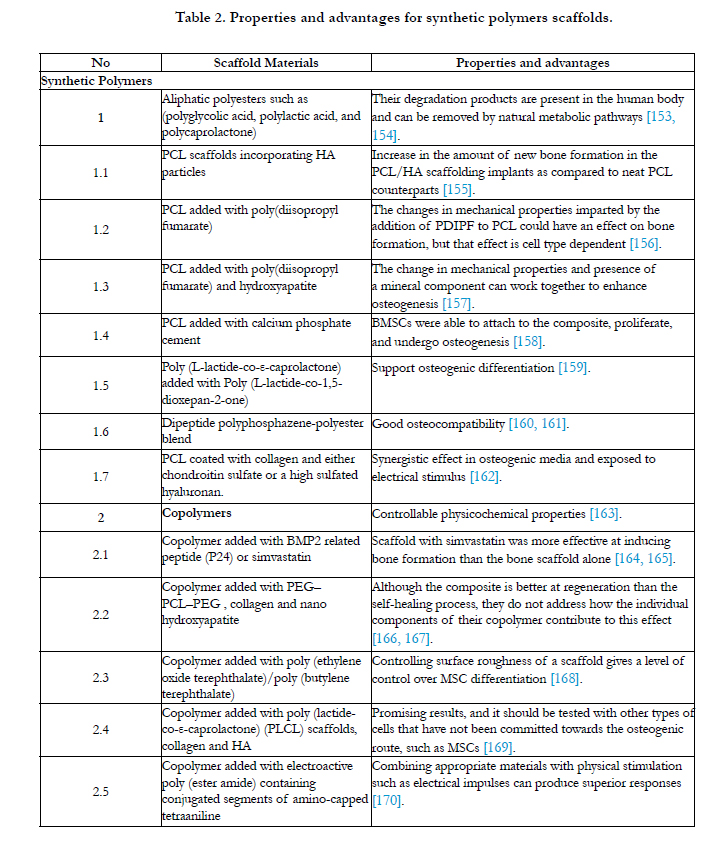
Table 2. Properties and advantages for synthetic polymers scaffolds.
Ceramics are crystalline texture of inorganic, nonmetallic mineral salts. This group is classified to two subgroups: bioinert or bioactive, also bioactive ceramics are categorized as resorbable or nonresorbable (Table 3) [58, 59]. Hydroxyapatite (HA), Calcium Phosphate (CP), Tricalcium Phosphates (TCP), and glass ionomer cesments, are all designated in this group [60]. The most commonly inspected are calcium phosphate ceramics, tricalcium phosphate and hydroxyapatite, because of their chemicophysical uniformities to the bone mineralization phase [61], they form a perfect osteoconductive scaffold for bone regeneration. Suetsuna et al. analyzed the records of 36 patients, where HA scaffold (40–45% porosity) sunk slightly into the vertebral body, for one level herniated cervical discs, no graft related complications were observed [62]. On the other hand Kim et al., using a HA scaf fold (30% porous), found that all implants carried out had fusion at 6–12 months, with good clinical results and no graft collapse [63]. In another study, HA but with plating was used, and complete fusion occurred in 98-100% [64]. Dai and Jiang investigated clinical controlled trial of βTCP, contained in interbody cages, for patients with cervical radiculopathy [65]. A total of 62 patients were randomized into an anterior plating or nonplating treatment group, and followed for 2 years. At 6 months, successful fusion was noted in all patients. The authors concluded interbody cage containing βTCP to be an appropriate treatment for cervical fusion. However, the debate is still ongoing about their mechanical strength and resorbability.
Calcium sulphate can be used safely in benign metaphyseal bone defects, but it has a quicker resorption rate with more inconsistent results [66]. Biphasic calcium phosphates, which combine 40% TCP with 60% HA, may produce further physiological equation between mechanical support and bone regeneration. Yamada et al. accomplished a histological research of βTCP, HA with various ratios of the two so as to recognize which was the most conducive to osteoclastic activity [67]. This study suggests 60/40 ratio to give a more natural surface than either βTCP or HA alone. Biphasic macroporous ceramic scaffold appears effective in the treatment of metaphyseal defects for bone cysts and benign bone tumors, also the addition of osteoprogenitor cells from a bone marrow aspirate may hasten bone regeneration. Siegel et al. [68] observed 51 patients with benign bone tumors treated with the combined scaffold of βTCP and osteoprogenitor cells aspirated from bone marrow. At six months after operation, all implanted grafts showed radiological features comparable to the framing cancellous bone, as well the trabeculation and resorption rates were similar. In addition El-Adl et al. [69] reported on 34 patients with benign bone tumors treated with TCP/HA scaffold and bone marrow aspirate. This study demonstrated that the rate of bone regeneration was directly related to the size of defect. Several studies have estimated the wall cyst confusion by injection of a ceramic. Mik et al. marked out 55 patients who were treated for bone cysts using calcium sulphate pellets [70]. This study showed that 80% of patients had a complete or partial response after treatment. Furthermore Joeris et al. used percunateous tricalcium sulphate for bone regeneration and concluded that 96% of patients were with good results [71].
Coral in the presence of a phosphate donates calcium hydroxyapatite (known as coralline HA) and removes all immunogenic protein [72]. Agrillo et al. using granulated coralline HA within a carbon fiber cage demonstrated complete fusion in all 45 patients at 12 months with no complications [73].
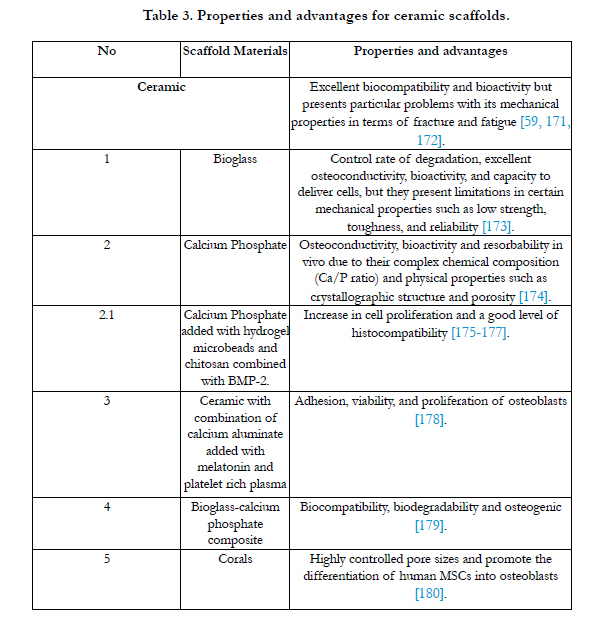
Table 3. Properties and advantages for ceramic scaffolds.
Several metallic scaffolds are used to provide support for bone defect regeneration, such as titanium [74], stainless steel [75], and aluminum [76], these metals are mechanically strong but are not biodegradable and release toxic metallic ions that lead to inflammatory cascades, allergic reactions, and tissue loss [77]. The essential abuse of metallic scaffolds is the deficiency of biological realization on the material surface. To overcome this problem, tissue engineering presents different ways to protect the mechanical properties and improve the biocompatibility of the surface. For example, Hydroxyapatite has been used to provide the necessary bioactivity to the titanium mesh with a porous network to assist osteoconduction [78, 79], also in cases where there is existing gap, titanium scaffolds often has been complemented with delivery of TGF- and BMP-2 [80, 81], as well as stem cells have been cultured in vitro onto titanium scaffolds to induce the formation of calcified nodules and increase the production of mineralized extracellular matrix onto the scaffold [82]. Different clinical studies have utilized porous Ti scaffolds for tissues reconstruction. Kuttenberger et al. have applied laser-perforated titanium micro-mesh into 20 patients with defects in the craniofacial region [83]. The results showed loss of the mesh and excellent long-term stability during 8 years follow-up. Also Bystedt et al. concluded that implantation of porous titanium granules seem to function well as augmentation material in the sinus floor [84]. As well Jaquiéry et al. have used titanium meshes and autogenous bone graft into 26 patients with small and midsize orbital defects. This study indicated that titanium meshes provided stability and can support the orbital content [85]. Although there is a paucity of literature regarding the clinical outcomes and result of porous titanium scaffolds, longer follow-up periods and a larger sample of patients is still required in order to obtain reliable clinical success rates.
Combining two or more materials such as ceramics and polymers [86-88], the structure and biochemical properties can be modified to achieve more favorable characteristics, like biodegradability [89, 90]. For example, hydroxyapatite/PLGA composites possess the osteoconductive properties of hydroxyapatite and biodegradability of PLGA [91]. Polycaprolactone-tricalcium phosphate (PCL–TCP) scaffolds combined with recombinant human BMP7 has been demonstrated to completely bridge a critical size of tibial defect in a sheep model [92]. Also adult stem cells have been used to generate new tissue in combination with scaffold matrices [93]. Currently tissue engineering has developed smart delivery system which act in a sequential manner (one agent appears while another disappears) to achieve sequential delivery of BMP-2 and BMP-7, where nanocapsules of PLGA release one of the growth factors and then co-entrapped in chitosan fiber or PCL 3-D plotted scaffolds [94]. Smart systems can be used for controlled drug delivery using a group of polymers that physically or chemically respond to environmental stimuli such as light, temperature or pH. The mechanism of delivery suggests that upon decrease of temperature of the target site, swelling of nanospheres leads to release of their content, maximizing delivery at the target site.
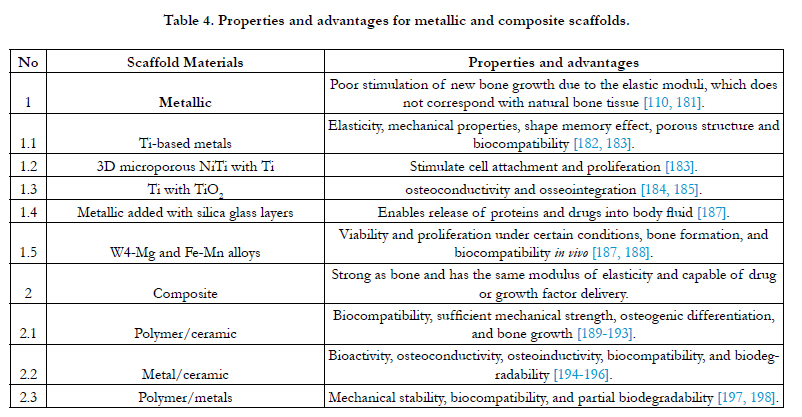
Table 4. Properties and advantages for metallic and composite scaffolds.
Results
In spite of several acceptable scaffold options being available for bone regeneration, these options still need to bridge the gap between research and clinical practice. There is little information available about the cellular basis for bone regeneration in humans. Several problems limit the broad usage of such options, including lack of randomized controlled human studies, regulatory necessity, dubious long term results, as well as technique specific limitations.
Conclusion
The studies should be nurtured and monitored by a combination of clinical experience, and knowledge of basic biological principles. Future trends may focus on the effective combinations of osteoinductive materials, osteoinductive growth factors and cell-based tissue regeneration tactic using composite carriers.
There is no single ideal graft material to choose in clinical practice, therefore research is ongoing within all relevant fields, to establish modern bone regeneration protocols that may lead to ideal graft substitutes.
References
- Nandi SK, Roy S, Mukherjee P, Kundu B, De DK, et al. (2010) Orthopedic applications of bone graft and graft substitutes: a review. Indian J Med Res 132(1): 15–30.
- Elsalanty ME, Genecov DG (2009) Bone grafts in craniofacial surgery. Craniomaxillofac Trauma Reconstr 2(3): 125–134.
- Dinopoulos H, Dimitriou R, Giannoudis PV (2012) Bone graft substitutes: What are the options? Surgeon 10(4): 230–239.
- Bigham AS, Dehghani SN, Shafiei Z, Torabi Nezhad S (2008) Xenogenicbone matrix and fresh autogenous cortical bone effects on experimentalb bone healing: radiological, histopathological and biomechanical evaluation. J Orthop Traumatol 9(2): 73–80.
- Scaglione M, Fabbri L, Dell’Omo D, Gambini F, Guido G (2014) Long bone nonunions treated with autologous concentrated bone marrow-derived cells combined with dried bone allograft. Musculoskelet Surg 98(2): 101- 106.
- Greenwald AS, Boden SD, Goldberg VM, Khan Y, Laurencin CT, et al. (2001) Bone-graft substitutes: facts, fictions and applications. J Bone Joint Surg Am 83(2): 98–103.
- Kneser U, Schaefer DJ, Munder B, Klemt C, Andree C (2002) Tissue engineering of bone. Min Invas Ther & Allied Technol 11(3): 107-116.
- Klokkevold PR, Jovanovic, SA (2002) Advanced implant surgery and bone grafting techniques. Carranza's Clinical Periodontology, 9th Edition. Philadelphia: WB Saunders Co: 907-908.
- Boyan BD, Weesner TC, Lohmann CH, Andreacchio D, Carnes DL, et al. (2000) Porcine fetal enamel matrix derivative enhances bone formation induced by demineralized freeze dried bone allograft in vivo. J Periodontol 71(8): 1278–1286.
- Russell JL, Block JE (2000) Surgical harvesting of bone graft from the ilium: point of view. Med Hypotheses 55(6): 474-479.
- Stevens B, Yang Y, Mohandas A, Stucker B, Nguyen KT (2008) A review of materials, fabrication methods, and strategies used to enhance bone regeneration in engineered bone tissues. J Biomed Mater Res B 85(2): 573-582.
- Graham S, Leonidou A, Aslam-Pervez N, Hamza A, Panteliadis P et al. (2010) Biological therapy of bone defects: the immunology of bone allotransplantation. Expert Opin Biol Ther 10(6): 885-901.
- Moore WR, Graves SE, Bain GI (2001) Synthetic bone graft substitutes. ANZ J Surg 71(6): 354-361.
- Polo-Corrales L, Latorre-Esteves M, Ramirez-Vick JE (2014) Scaffold Design for Bone Regeneration. J Nanosci Nanotechnol 14(1): 15–56.
- Holtorf HL, Jansen JA, Mikos AG (2006) Modulation of cell differentiation in bone tissue engineering constructs cultured in a bioreactor. Adv Exp Med Biol 585: 225-241.
- Gadeau AP, Chaulet H, Daret D, Kockx M, Daniel-Lamaziere JM (2001) Time course of osteopontin, osteocalcin, and osteonectin accumulation and calcification after acute vessel wall injury. J Histochem Cytochem 49(1): 79- 86.
- Sikavitsas VI, Temenoff JS, Mikos AG (2001) Biomaterials and bone mechanotransduction. Biomaterials 22(9): 2581-2593.
- Nudelman F, Pieterse K, George A, Bomans PHH, Friedrich H, et al. (2010) The role of collagen in bone apatite formation in the presence of hydroxyapatite nucleation inhibitors. Nat Mater 9(12): 1004-1009.
- Kini U, Nandeesh BN (2012) "Physiology of Bone Formation, Remodeling, and Metabolism". Radionuclide and Hybrid Bone Imaging. Eds. Fogelman, et al. Berlin Heidelberg: Springer-Verlag: 29-57.
- Albrektsson T, Johansson C (2001) Osteoinduction, osteoconduction and osseointegration. Eur Spine J 10(2): 96–101.
- Parikh SN (2002) Bone graft substitutes: past, present, future. J Postgrad Med 48(2): 142–148.
- Dell PC, Burchardt H, Glowczewskie FP (1985) Aroentgenographic, biomechanical, and histological evaluation of vascularized and nonvascularized segmental fibular canine autografts. J Bone Joint Surg Am 67(1): 105–112.
- Goldberg VM, Stevenson S (1987) Natural history of autografts and allografts. Clin Orthop Relat Res 225: 7–16.
- Stevenson S, Li XQ, Davy DT, Klein L, Goldberg VM (1997) Critical biological determinants of incorporation of nonvascularized cortical bone grafts. Quantification of a complex process and structure. J Bone Joint Surg Am 79(1): 1–16.
- Hench LL, Polak JM (2002) Third-generation biomedical materials. Science 295(5557): 1014-1017.
- Anderson JM (2001) Biological Responses to Materials. Annu Rev Mater Res 31(1): 81-110.
- Navarro M, Michiardi A, Castano O, Planell JA (2008) Biomaterials in orthopaedics. J R Soc Interface 5(27): 1137-1158.
- Amini AR, Laurencin CT, Nukavarapu SP (2012) Bone tissue engineering: recent advances and challenges. Crit Rev Biomed Eng 40(5): 363-408.
- Sundelacruz S, Kaplan DL (2009) Stem cell- and scaffold-based tissue engineering approaches to osteochondral regenerative medicine. Semin Cell Dev Biol 20(6): 646-655.
- Williams DF (2008) On the mechanism of biocompatibility. Biomaterials 29(20): 2941-2953.
- Rivera-Chacon DM, Alvarado-Velez M, Acevedo-Morantes CY, Singh SP, Gultepe E, et al. (2013) Fibronectin and Vitronectin Promote Human Fetal Osteoblast Cell Attachment and Proliferation on Nanoporous Titanium Surfaces. J Biomed Nanotechnol 9(6): 1092-1097.
- Freed LE, Vunjak-Novakovic G, Biron R, Eagles D, Lesnoy D, et al. (1994) Biodegradable polymer scaffolds for tissue engineering. Biotechnology 12(7): 689-693.
- Hughes FJ, Turner W, Belibasakis G, Martuscelli G (2006) Effects of growth factors and cytokines on osteoblast differentiation. Periodontol 41(1): 48-72.
- Giannoudis PV, Dinopoulos H, Tsiridis E (2005) Bone substitutes: an update. Injury 36(3): 20-27.
- Finkemeier CG (2002) Bone-grafting and bone-graft substitutes. J Bone Joint Surg Am 84(3): 454-464.
- Schlickewei W, Schlickewei C (2007) The Use of Bone Substitutes in the Treatment of Bone Defects-the Clinical View and History. Macromol Symp 253(1): 10–23.
- Massia SP, Holecko MM, Ehteshami GR (2004) In vitro assessment of bioactive coatings for neural implant applications. J Biomed Mater Res 68(1): 177-86.
- Broderick E, Infanger S, Turner TM, Sumner DR (2005) Depressed bone mineralization following high dose TGF-beta1 application in an orthopedic implant model. Calcif Tissue Int 76(5): 379-384.
- McKinney L, Hollinger JO (1996) A bone regeneration study: transforming growth factor-beta 1 and its delivery. J Craniofac Surg 7(1): 36-45.
- Critchlow MA, Bland YS, Ashhurst DE (1995) The effect of exogenous transforming growth factor-beta 2 on healing fractures in the rabbit. Bone 16(5): 521-527.
- Willerth SM, E. Sakiyama-Elbert SE (2007) Approaches to neural tissue engineering using scaffolds for drug delivery. Adv Drug Deliv Rev 59(4-5):325-338.
- Schmidmaier G, Lucke M, Schwabe P, Raschke M, Haas NP, et al. (2006) Collective review: bioactive implants coated with poly (d,l-lactide) and growth factors IGF-I, TGF-beta1, or BMP-2 for stimulation of fracture healing.J Long-Term Eff Med Implants 16(1): 61-69.
- Street J, Bao M, DeGuzman L, Bunting S, Peale FV, et al. (2002) Vascular endothelial growth factor stimulates bone repair by promoting angiogenesis and bone turnover. Proc Natl Acad Sci 99(15): 9656-9661.
- Yang C, Hillas PJ, Baez JA, Nokelainen M, Balan J, et al. (2004) The application of recombinant human collagen in tissue engineering. BioDrugs 18(2): 103-119.
- Yannas IV, Burke JF, Gordon PL, Huang C, Rubenstein RH (1980) Design of an artificial skin. II. Control of chemical composition, J Biomed Mater Res 14(2): 107-132.
- Kohara H, Tabata Y (2011) Enhancement of ectopic osteoid formation following the dual release of bone morphogenetic protein 2 and Wnt1 inducible signaling pathway protein 1 from gelatin sponges. Biomaterials 32(24):5726-5732.
- Holzwarth JM, Ma PX (2011) Biomimetic nanofibrous scaffolds for bone tissue engineering. Biomaterials 32(36): 9622-9629.
- Borden M, El-Amin SF, Attawia M, Laurencin CT (2003) Structural and human cellular assessment of a novel microspherebased tissue engineered scaffold for bone repair. Biomaterials 24(4): 597-609.
- Mikos AG, Czerwonka LA, Bao Y, Langer R, Winslow DN, et al. (1994) Preparation and Characterization of Poly(L-Lactic Acid) Foams. Polymer 35(5): 1068-1077.
- Zein I, Hutmacher DW, Tan KC, Teoh SH (2002) Fused deposition modeling of novel scaffold architectures for tissue engineering applications. Biomaterials 23(4): 1169-1185.
- Ibanez J, Carreno A, GarciaAmorena C, Caral J, Gaston F, et al. (1998) Results of the biocompatible osteoconductive polymer (BOP) as an intersomatic graft in anterior cervical surgery. Acta Neurochir 140(2): 126–133.
- Madawi AA, Powell M, Crockard HA (1996) Biocompatible osteoconductive polymer versus iliac graft. A prospective comparative study for the evaluation of fusion pattern after anterior cervical discectomy. Spine 21(18): 2123–2129.
- Dorward NL, Malik NN, Illingworth RD (1997) Disintegration of cervical interbody BOP grafts with neurological sequelae: a report of 2 cases. Br J Neurosurg 11(1): 65–68.
- Hafez RF, Crockard HA (1997) Failure of osseous conduction with cervical interbody BOP graft. Br J Neurosurg 11(1): 57–59.
- McLorinan GC, Choudhari KA, Cooke RS (2001) Life threatening complication of biocompatible osteoconductive polymer graft after anterior cervical discectomy. Br J Neurosurg 15(4): 363–365.
- Yang X, Chen X, Wang H (2009) Acceleration of osteogenic differentiation of preosteoblastic cells by chitosan containing nanofibrous scaffolds. Biomacromolecules 10(10) : 2772-2778.
- Dunn MG, Bellincampi LD, Alfred J, Tria Jr, Zawadsky JP (1997) Preliminary development of a collagen-PLA composite for ACL reconstruction. J Applied Polymer Scienc 63: 1423–1428.
- Williams DF (2009) On the nature of biomaterials. Biomaterials 30(30): 5897–5909.
- Doremus RH (1992) Bioceramics. J Mater Sci 27: 285–297.
- Xin R, Leng Y, Chen J, Zhang Q (2005) A comparative study of calcium phosphate formation on bioceramics in vitro and in vivo. Biomaterials 26(33): 6477–6486.
- Helm G (2005) Bone graft substitutes for use in spinal fusions. Clin Neurosurg 52: 250–255.
- Suetsuna F, Yokoyama T, Kenuka E, Harata S (2001) Anterior cervical fusion using porous hydroxyapatite ceramics for cervical disc herniation. a two year follow up. Spine J Off J N Am Spine Soc 1(5): 348–357.
- Kim P, Wakai S, Matsuo S, Moriyama T, Kirino T (1998) Bisegmental cervical interbody fusion using hydroxyapatite implants: surgical results and long term observation in 70 cases. J Neurosurg 88(1): 21–27.
- Bruneau M, Nisolle JF, Gilliard C, Gustin T (2001) Anterior cervical interbody fusion with hydroxyapatite graft and plate system. Neurosurg Focus10(4): E8.
- Dai L, Jiang L (2008) Anterior cervical fusion with interbody cage containing betatricalcium phosphate augmented with plate fixation: a prospective randomized study with 2year follow up. Eur Spine J 17(5): 698–705.
- Faour O, Dimitriou R, Cousins CA, Giannoudis PV (2011) The use of bone graft substitutes in large cancellous voids: any specific needs?. Injury 42(2): S87- S90.
- Yamada S, Heymann D, Bouler JM, Daculsi G (1997) Osteoclastic resorption of calcium phosphate ceramics with different hydroxyapatite/betatricalcium phosphate ratios. Biomaterials 18(15): 1037–1041.
- Siegel HJ, Baird RC 3rd, Hall J, Lopez-Ben R, Lander PH (2008) The outcome of composite bone graft substitute used to treat cavitary bone defects. Orthopedics 31(8): 754-758.
- El-Adl G, Mostafa MF, Enan A, Ashraf M (2009) Biphasic ceramic bone substitute mixed with autogenous bone marrow in the treatment of cavitary benign bone lesions. Acta Orthop Belg 75(1): 110-118.
- Mik G, Arkader A, Manteghi A, Dormans JP (2009) Results of a minimally invasive technique for treatment of unicameral bone cysts. Clin Orthop Relat Res 467(11): 2949-2954.
- Joeris A, Ondrus S, Planka L, Gal P, Slongo T (2010) ChronOS inject in children with benign bone lesions: does it increase the healing rate? Eur J Pediatr Surg 20(1): 24-28.
- Shors EC (2003) The development of coralline porous ceramic bone graft substitutes. Bone graft substitutes.West Conshohocken, PA: ASTM International. 271-288.
- Agrillo U, Mastronardi L, Puzzilli F (2002) Anterior cervical fusion with carbon fiber cage containing coralline hydroxyapatite: preliminary observations in 45 consecutive cases of soft disc herniation. J Neurosurg 96(3): 273–276.
- Cachinho SC, Correia RN (2008) Titanium scaffolds for osteointegration: mechanical, in vitro and corrosion behaviour. J Mater Sci Mater Med 19(1): 451-457.
- Disegi JA, Eschbach L (2000) Stainless steel in bone surgery. Injury 31(4): 2-6.
- Yoo JJ, Kim YM, Yoon KS, Koo KH, Song WS, et al. (2005) Alumina-onalumina total hip arthroplasty. A five-year minimum follow-up study. J Bone Joint Surg Am 87(3): 530-535.
- Matassi F, Botti A, Sirleo L, Carulli C, Innocenti M (2013) Porous metal for orthopedics implants. Clin Cases Miner Bone Metab 10(2): 111-115.
- Thalgott JS, Giuffre JM, Klezl Z, Timlin M (2002) Anterior lumbar interbody fusion with titanium mesh cages, coralline hydroxyapatite, and demineralized bone matrix as part of a circumferential fusion. Spine J 2(1): 63-69.
- Niu CC, Chen LH, Lai PL, Fu TS, Chen WJ (2005) Trapezoidal titanium cage in anterior cervical interbody fusion: A clinical experience. Chang Gung Med J 28(4): 212-221.
- Alam S, Ueki K, Marukawa K, Ohara T, Hase T, Takazakura D, et al. (2007) Expression of bone morphogenetic protein 2 and fibroblast growth factor 2 during bone regeneration using different implant materials as an onlay bone graft in rabbit mandibles. Oral Surg Oral Med Oral Path Oral Radiol Endod 103(1): 16-26.
- Jansen JA, Vehof JW, Ruhe PQ, Kroze-Deutman H, Kuboki Y, et al. (2005) Growth factors-loaded scaffolds for bone engineering. J Control Release 101(1-3): 127-136.
- Zhang W, Walboomers XF, van Kuppevelt TH, Daamen WF, Bian Z, et al. (2006) The performance of human dental pulp stem cells on different threedimensional scaffolds materials. Biomaterials 27(33): 5658-5668.
- Kuttenberger JJ, Hardt N (2001) Long-term results following reconstruction of craniofacial defects with titanium micro-mesh systems. J Cranio-Max-Fac Surg 29(2): 75-81.
- Bystedt H, Rasmusson L (2009) Porous titanium granules used as osteoconductive material for sinus floor augmentation: A clinical pilot study. Clin Implant Dent Relat Res 11(2): 101-105.
- Jaquiéry C, Aeppli C, Cornelius P, Palmowsky A, Kunz C, et al.(2007) Reconstruction of orbital wall defects: critical review of 72 patients. Int J Oral Maxillofac Surg 36(3): 193-199.
- Hutmacher DW, Cool S (2007) Concepts of scaffold-based tissue engineering— the rationale to use solid freeform fabrication techniques. J Cell Mol Med 11(4): 654–669.
- Tanner KE (2010) Bioactive composites for bone tissue engineering. Proc Inst Mech Eng H 224: 1359–1372.
- Miyazaki T (2013) Design of bone integrating organic-inorganic composite suitable for bone repair. Front Biosci 1(5): 333–340.
- Hutmacher DW, Schantz JT, Lam CX, Tan KC, Lim TC (2007) State of the art and future directions of scaffold-based bone engineering from a biomaterials perspective. J Tissue Eng Regen Med 1(4): 245–260.
- Hutmacher DW (2000) Scaffolds in tissue engineering bone and cartilage. Biomaterials 21(24): 2529–2543.
- Huang YX, Ren J, Chen c, Ren TB, Zhou XY (2008) Preparation and Properties of Poly(lactide-co-glycolide) (PLGA)/Nano-Hydroxyapatite (NHA)Scaffolds by Thermally Induced Phase Separation and Rabbit MSCs Culture on Scaffolds. J Biomater Appl 22(5): 409-432.
- Reichert JC, Cipitria A, Epari DR, Saifzadeh S, Krishnakanth P, et al.(2012) A tissue engineering solution for segmental defect regeneration in loadbearing long bones. Sci Transl Med 4(141): 141ra93.
- Mizuno H (2009) Adipose derived stem cells for tissue repair and regeneration: ten years of research and a literature review. J Nippon Med Sch 76(2): 56–66.
- Coskun S, Korkusuz F, Hasirci V (2005) Hydroxyapatite reinforced poly(3 hydroxybutyrate) and poly(3-hydroxybutyrate- co-3-hydroxyvalerate) baseddegradable composite bone plate. J. Biomater Sci Polym E 16(12): 1485–1502.
- Lee KY, Yuk SH (2007) Polymetric protein delivery systems. Prog Polym Sci 32(7): 669-697.
- Lee SH, Shin H (2007) Materials and scaffolds for delivery of bioactive molecules in bone and cartilage tissue engineering.Advanced Drug Delivery Reviews 59(4-5): 339-359.
- Vagaská B, Bacáková L, Filová E, Balík K (2010) Osteogenic cells on bioinspired materials for bone tissue engineering. Physiol Res 59(3): 309-322.
- Semino CE (2008) Self-assembling peptides: from bio-inspired materials to bone regeneration. J Dent Res 87(7): 606-616.
- Aravamudhan A, Ramos DM, Nip J, Harmon MD, James R, et al. (2013) Cellulose and Collagen Derived Micro-Nano Structured Scaffolds for Bone Tissue Engineering. J Biomed Nanotechnol 9(4): 719-731.
- Hiraoka Y, Kimura Y, Ueda H, Tabata Y (2003) Fabrication and biocompatibility of collagen sponge reinforced with poly(glycolic acid) fiber. Tissue Eng 9(6): 1101-1112.
- Harley BA, Leung JH, Silva ECCM, Gibson LJ (2007) Mechanical characterization of collagen-glycosaminoglycan scaffolds. Acta Biomaterialia 3(4): 463-474.
- Yu HS, Won JE, Jin GZ, Kim HW (2012) Construction of mesenchymal stem cell-containing collagen gel with a macrochanneled polycaprolactone scaffold and the flow perfusion culturing for bone tissue engineering. Biores Open Access 1(3): 124–136.
- Huang C, Ogawa R (2010) Mechanotransduction in bone repair and regeneration. FASEB J 24(10): 3625-3632.
- Kawata A, Mikuni-Takagaki Y (1998) Mechanotransduction in stretched osteocytes-temporal expression of immediate early and other genes. Biochem Biophys Res Commun 246(2): 404-408.
- Xu C, Su P, Chen X, Meng Y, Yu W, et al.(2011) Biocompatibility and osteogenesis of biomimetic bioglass-collagen-phosphatidylserine composite scaffolds for bone tissue engineering. Biomaterials 32(4): 1051-1058.
- Serpooshan V, Julien M, Nguyen O, Wang H, Li A, et al.(2010) Reduced hydraulic of three-dimensional collagen scaffolds attenuates gel contraction and promotes the growth and differentiation of mesenchymal stem cells. Acta Biomaterialia 6(10): 3978-3987.
- O’Brien FJ, Harley BA, Waller MA, Yannas IV, Gibson LJ, et al. (2007) The effect of pore size on permeability and cell attachment in collagen scaffolds of tissue engineering. Technol Healt Care 15(1): 3-17.
- Ratanavaraporn J, Damrongsakkul S, Kanokpanont S, Yamamoto M, Tabata Y (2011) Osteogenic differentiation of bone-marrow-derived stem cells cultured with mixed gelatin and chitosanoligosaccharide scaffolds. J Biomater Sci Polym 22: 1083-1098.
- Hussain A, Bessho K, Takahashi K, Tabata Y (2012) Magnesium calcium phosphate as a novel component enhances mechanical/physical properties of gelatin scaffold and osteogenic differentiation of bone marrow mesenchymal stem cells. Tissue Eng Part A 18(7-8): 768-774.
- Staiger MP, Pietak AM, Huadmai J, Dias G (2006) Magnesium and its alloys as orthopedic biomaterials: a review. Biomaterials 27(9): 1728- 1734.
- Lu H, Kawazoe N, Kitajima T, Myoken Y, Tomita M, et al. (2012) Spatial immobilization of bone morphogenetic protein-4 in a collagen- PLGA hybrid scaffold for enhanced osteoinductivity. Biomaterials 33(26): 6140-6146.
- Pang EK, Im SU, Kim CS, Choi SH, Chai JK, et al. (2004) Effect of recombinant human bone morphogenetic protein-4 dose on bone formation in a rat calvarial defect model. J Periodontol 75(10): 1364-1370.
- Niu LN, Jiao K, Qi YP, Nikonov S, Yiu CKY, et al. (2012) Intrafibrillar silicification of collagen scaffolds for sustained release of stem cell homing chemokine in hard tissue regeneration. FASEB J 26(11): 4517- 4529.
- Kitaori T, Ito H, Schwarz EM, Tsutsumi R, Yoshitomi H, et al.(2009) Stromal cell-derived factor 1/CXCR4 signaling is critical for the recruitment of mesenchymal stem cells to the fracture site during skeletal repair in a mouse model. Arthritis Rheum 60(3): 813-823.
- Costa-Pinto AR, Reis RL, Neves NM (2011) Scaffolds based bone tissue engineering: the role of chitosan. Tissue Eng Part B Rev 17(5): 331-347.
- Costa-Pinto AR, Correlo VM, Sol PC, Bhattacharya M, Srouji S, et al.(2011) Chitosan-poly(butylene succinate) scaffolds and human bone marrow stromal cells induce bone repair in a mouse calvaria model. J Tissue Eng Regen Med 6(1): 21-28.
- Wang L, Stegemann JP (2010) Thermogelling chitosan and collagen composite hydrogels initiated with beta-glycerophosphate for bone tissue engineering. Biomaterials 31(14): 3976-3985.
- Hoemann CD, Chenite A, Sun J, Hurtig M, Serreqi A, Lu Z, et al. (2007) Cytocompatible gel formation of chitosan-glycerol phosphate solutions supplemented with hydroxyl ethyl cellulose is due to the presence of glyoxal. J Biomed Mater Res A 83(2): 521-529.
- Wang L, Stegemann JP (2011) Glyoxal crosslinking of cell-seeded chitosan/collagen hydrogels for bone regeneration. Acta Biomate 7(6): 2410-2417.
- Lima PAL, Resende CX, Soares GD, Anselme K, Almeida LE (2013) Preparation, characterization and biological test of 3D-scaffolds based on chitosan, fibroin and hydroxyapatite for bone tissue engineering. Mater Sci Eng C Mater Biol Appl 33(6): 3389-3395.
- Wang L, Li C (2007) Preparation and physicochemical properties of a novel hydroxyapatite/chitosan-silk fibroin composite. Carbohyd Polym 68(4): 740-745.
- Bi L, Cheng W, Fan H, Pei G (2010) Reconstruction of goat tibial defects using an injectable tricalcium phosphate/chitosan in combination with autologous platelet-rich plasma. Biomaterials 31(12): 3201-3211.
- Kiuru J, Viinikka L, Myllylä G, Pesonen K, Perheentupa J (1991) Cytoskeleton-dependent release of human platelet epidermal growth factor. Life Sci 49(26):1997-2003.
- Florczyk SJ, Leung M, Li Z, Huang JI, Hopper RA, et al.(2013) Evaluation of three-dimensional porous chitosan-alginate scaffolds in rat calvarial defects for bone regeneration applications. J Biomed Mater Res A 101(10): 2974-2983.
- Nandi SK, Kundu B, Basu D (2013) Protein growth factors loaded highly porous chitosan scaffold: a comparison of bone healing properties. Mater Sci Eng C Mater Biol Appl 33(3): 1267-75.
- Qu Z, Yan J, Li B, Zhuang J, Huang Y (2010) Improving bone marrow stromal cell attachment on chitosan/hydroxyapatite scaffolds by an immobilized RGD peptide. Biomed Mater 5(6): 065001.
- Vepari C, Kaplan DL (2007) Silk as a Biomaterial. Prog Polym Sci 32(8-9): 991-1007.
- Zhang Y, Wu C, Friis T, Xiao Y (2010) The osteogenic properties of CaP/silk composite scaffolds. Biomaterials 31(10): 2848-2856.
- Bhumiratana S, Grayson W, Castaneda A, Rockwood D, Gil ES, et al.(2011) Nucleation and growth of mineralized bone matrix on silkhydroxyapatite composite scaffolds. Biomaterials 32(11): 2812-2820.
- Rockwood DN, Gil ES, Park SH, Kluge JA, Grayson W, et al. (2011) Ingrowth of human mesenchymal stem cells into porous silk particle reinforced silk composite scaffolds: An in vitro study. Acta Biomater 7(1):144-151.
- Park SH, Gil ES, Shi H, Kim HJ, Lee K, et al. (2010) Relationships between degradability of silk scaffolds and osteogenesis. Biomaterials 31(24): 6162-6172.
- Wan C, Gilbert SR, Wang Y, Cao X, Shen X, et al. (2008) Activation of the hypoxia-inducible factor-1alpha pathway accelerates bone regeneration. Proc Natl Acad Sci USA 105(2): 686-691.
- Suárez-González D, Barnhart K, Saito E, Vanderby R, Hollister SJ, et al. (2010) Controlled nucleation of hydroxyapatite on alginate scaffolds for stem cell-based bone tissue engineering. J Biomed Mater Res A 95(1): 222-234.
- Zhou H, Xu HH (2011) The fast release of stem cells from alginate- fibrin microbeads in injectable scaffolds for bone tissue engineering. Biomaterials 32(30): 7503-7513.
- Lee GS, Park JH, Shin US, Kim HW (2011) Direct deposited porous scaffolds of calcium phosphate cement with alginate for drug delivery and bone tissue engineering. Acta Biomater 7(8): 3178-3186.
- Kanczler JM, Ginty PJ, White L, Clarke NMP, Howdle SM, et al. (2010) The effect of the delivery of vascular endothelial growth factor and bone morphogenic protein-2 to osteoprogenitor cell populations on bone formation. Biomaterials 31(6): 1242-1250.
- Kolambkar YM, Boerckel JD, Dupont KM, Bajin M, Huebsch N, et al. (2011) Spatiotemporal delivery of bone morphogenetic protein enhances functional repair of segmental bone defects. Bone 49(3): 485-492.
- He X, Dziak R, Mao K, Genco R, Swithart M, et al. (2013) Integration of a novel injectable nano calcium sulfate/alginate scaffold and BMP2 gene-modified mesenchymal stem cells for bone regeneration. Tissue Eng Part A 19(3-4): 508-518.
- Pavasant P, Shizari TM, Underhill CB (1994) Distribution of hyaluronan in the epiphysial growth plate: turnover by CD44-expressing osteoprogenitor cells. J Cell Sci 107(10): 2669-2677.
- Bae MS, Yang DH, Lee JB, Heo DN, Kwon YD, et al. (2011) Photo-cured hyaluronic acid-based hydrogels containing simvastatin as a bone tissue regeneration scaffold. Biomaterials 32(32): 8161-8171.
- Jha AK, Xu X, Duncan RL, Jia X (2011) Controlling the adhesion and differentiation of mesenchymal stem cells using hyaluronic acidbased, doubly crosslinked networks. Biomaterials 32(10): 2466-2478.
- Patterson J, Siew R, Herring SW, Lin ASP, Guldberg R,et al.(2010) Hyaluronic acid hydrogels with controlled degradation properties for oriented bone regeneration. Biomaterials 31(26): 6772-6781.
- Martínez-Sanz E, Ossipov DA, Hilborn J, Larsson S, Jonsson KB, et al. (2011) Bone reservoir: Injectable hyaluronic acid hydrogel for minimal invasive bone augmentation. J Control Release 152(2): 232-340.
- Bhakta G, Rai B, Lim ZX, Hui JH, Stein GS, et al. (2012) Hyaluronic acid-based hydrogels functionalized with heparin that support controlled release of bioactive BMP-2. Biomaterials 33(26): 6113-6122.
- Ruppert R, Hoffmann E, Sebald W (1996) Human bone morphogenetic protein 2 contains a heparin-binding site which modifies its biological activity. Eur J Biochem 237(1): 295-302.
- Kisiel M, Martino MM, Ventura M, Hubbell JA, Hilborn J, et al. (2013) Improving the osteogenic potential of BMP-2 with hyaluronic acid hydrogel modified with integrin-specific fibronectin fragment. Biomaterials 34(3): 704-712.
- Holmes TC (2002) Novel peptide-based biomaterial scaffolds for tissue engineering. Trends in Biotechnol 20(1): 16-21.
- Mata A, Geng Y, Henrikson KJ, Aparicio C, Stock SR, et al. (2010) Bone regeneration mediated by biomimetic mineralization of a nanofiber matrix. Biomaterials 31(23): 6004-6012.
- Kishimoto N, Momota Y, Hashimoto Y, Omasa T, Kotani J (2011) Self-assembling peptide RADA16 as a scaffold in bone tissue engineering using dedifferentiated fat cells. J Oral Tissue Engin 8(7): 151–161
- Marí-Buyé N, Luque T, Navajas D, Semino CE. Development of a three-dimensional bone-like construct in a soft self-assembling peptide matrix. Tissue Eng Part A 2013;19:870–81.
- Amosi N, Zarzhitsky S, Gilsohn E, Salnikov O, Monsonego-Ornan E, et al. (2012) Acidic peptide hydrogels loaded with β-TCP particles induce bone regeneration. Acta Biomaterialia 8:2466-75.
- Rughani RV, Salick DA, Lamm MS, Yucel T, Pochan DJ, et al. (2009) Folding, Self-Assembly, and Bulk Material Properties of a de novo Designed Three-Stranded Beta-Sheet Hydrogel. Biomacromolecules ;10(5): 1295-1304.
- Sachlos E, Czernuszka JT (2003) Making tissue engineering scaffolds work. Review: the application of solid freeform fabrication technology to the production of tissue engineering scaffolds. Eur Cell Mater 5: 29-39.
- Wang D, He Y, Bi L, Qu Z, Zou J, et al. (2013) Enhancing the bioactivity of Poly(lactic-co-glycolic acid) scaffold with a nano-hydroxyapatite coating for the treatment of segmental bone defect in a rabbit model. Int J Nanomedicine 8: 1855-1865.
- Chuenjitkuntaworn B, Inrung W, Damrongsri D, Mekaapiruk K, Supaphol P, et al. (2010) Polycaprolactone/hydroxyapatite composite scaffolds: preparation, characterization, and in vitro and in vivo biological responses of human primary bone cells. J Biomed Mater Res A 94(1): 241-251.
- Fernandez JM, Molinuevo MS, Cortizo AM, McCarthy AD, Cortizo MS (2010) Characterization of poly(epsilon-caprolactone)/polyfumarate blends as scaffolds for bone tissue engineering. J Biomat Sci Polym 21(10): 1297-1312.
- Fernandez JM, Molinuevo MS, Cortizo MS, Cortizo AM (2011) Development of an osteoconductive PCL-PDIPF-hydroxyapatite composite scaffold for bone tissue engineering. J Tissue Eng Regen Med 5(6): 126-135.
- Wang S, Zhao P, Lin C, Huang Y (2013) In Vitro and In Vivo Osteoconductivity of Bone Marrow Stromal Cells in Biomimetic Polycaprolactone/ Calcium Phosphate Cement Composites. J Biomater Tissue Eng 3(5): 512-522.
- Dånmark S, Finne-Wistrand A, Wendel M, Arvidson K, Albertsson AC, et al. (2010) Osteogenic Differentiation by Rat Bone Marrow Stromal Cells on Customized Biodegradable Polymer Scaffolds. Bioactive and Compatible Polymers 25(2): 207-223.
- Deng M, Kumbar SG, Nair LS, Weikel AL, Allcock HR, et al.(2011) Biomimetic structures: biological implications of dipeptide-substituted polyphosphazene-polyster blend nanofiber matrices for load-bearing bone regeneration. Adv Funct Mater 21: 2641-2651.
- Jabbarzadeh E, Deng M, Lv Q, Jiang T, Khan YM, et al. (2012) VEGF incorporated biomimetic poly(lactide-co-glycolide) sintered microsphere scaffolds for bone tissue engineering. J Biomed Mater Res 100(8):2187-2196.
- Hess R, Jaeschke A, Neubert H, Hintze V, Moeller S, et al. (2012) Synergistic effect of defined artificial extracellular matrices and pulsed electric fields on osteogenic differentiation of human MSCs. Biomaterials 33(35): 8975-8985.
- Drury JL, Mooney DJ (2003) Hydrogels for tissue engineering: scaffold design variables and applications. Biomaterials 24(24): 4337-4351.
- Lin ZY, Duan ZX, Guo XD, Li JF, Lu HW, et al. (2010) Bone induction by biomimetic PLGA-(PEG-ASP)n copolymer loaded with a novel synthetic BMP-2-related peptide in vitro and in vivo. J Control Release 144(2): 190-195.
- Jiang L, Sun H, Yuan A, Zhang K, Li D, et al. (2013) Enhancement of osteoinduction by continual simvastatin release from poly(lacticco- glycolic acid)-hydroxyapatite-simvastatin nano-fibrous scaffold. J Biomed Nanotechnol 9(11): 1921-1928.
- Fu S, Ni P, Wang B, Chu B, Zheng L, et al. (2012) Injectable and thermo-sensitive PEG-PCL-PEG copolymerr/collagen/n-HA hydrogel composite for guided bone regeneration. Biomaterials 33(19): 4801-4809.
- Remya KR, Joseph J, Mani S, John A, Varma HK (2013) Nanohydroxyapatite incorporated electrospun polycaprolactone/polycaprolactone-polyethyleneglycol-polycaprolactone blend scaffold for bone tissue engineering applications. J Biomed Nanotechnol 9(9):1483-1494.
- Nandakumar A, Birgani ZT, Santos D, Mentink A, Auffermann N, et al. (2013) Surface modification of electrospun fibre meshes by oxygen plasma for bone regeneration. Biofabrication 5(1): 015006.
- Akkouch A, Zhang Z, Rouabhia M (2011) A novel collagen/ hydroxyapatite/poly(lactide-co-ε-caprolactone) biodegradable and bioactive3D porous scaffold for bone regeneration. J Biomed Mater Res A 96(4):693-704.
- Cui H, Liu Y, Deng M, Pang X, Zhang P, et al. (2012) Synthesis of biodegradable and electroactive tetraaniline grafted poly(ester amide) copolymers for bone tissue engineering. Biomacromolecules 13(9): 2881-2889.
- Best SM, Porter AE, Thian ES, Huang J (2008) Bioceramics: Past, present and for the future. J Eur Ceram Soc 28(7): 1319-1327.
- Liu Y, Lim J, Teoh SH (2013) Review: development of clinically relevant scaffolds for vascularised bone tissue engineering. Biotechnol Adv 31(5): 688-705.
- Fu Q, Saiz E, Rahaman MN, Tomsia AP (2011) Bioactive glass scaffolds for bone tissue engineering: state of the art and future perspectives. Mater Sci Eng C Mater Biol Appl 31(7): 1245-1256.
- Shepherd JH, Best SM (2011) Calcium phosphate scaffolds for bone repair. JOM 63(4): 83-92.
- Zhao L, Weir MD, Xu HH (2010) Human umbilical cord stemcell encapsulation in calcium phosphate scaffolds for bone engineering. Biomaterials 31(14): 3848-3857.
- Zhao L, Weir MD, Xu HH (2010) An injectable calcium phosphate-alginate hydrogel-umbilical cord mesenchymal stem cell paste for bone tissue engineering. Biomaterials 31(25): 6502-6510.
- Abarrategi A, Moreno-Vicente C, Martinez-Vazquez FJ, Civantos A, Ramos V, et al. (2012) Biological properties of solid free form designed ceramic scaffolds with BMP-2: in vitro and in vivo evaluation 7(3): e34117.
- Clafshenkel WP, Rutkowski JL, Palchesko RN, Romeo JD, McGowan KA, et al. (2012) A novel calcium aluminate-melatonin scaffold enhances bone regeneration within a calvarial defect. J Pineal Res 53(2):206-218.
- Yu L, Li Y, Zhao K, Tang Y, Cheng Z, et al. (2013) A novel injectable calcium phosphate cement-bioactive glass composite for bone regeneration 8(4): e62570.
- Tran CT, Gargiulo C, Thao HD, Tuan HM, Filgueira L, et al. (2011) Culture and differentiation of osteoblasts on coral scaffold from human bone marrow mesenchymal stem cells. Cell Tissue Bank 12(4): 247-261.
- Alvarez K, Nakajima H (2009) Metallic scaffolds for bone regeneration. Materials 2(3): 790-832.
- Bansiddhi A, Sargeant TD, Stupp SI, Dunand DC (2008) Porous NiTi for bone implants: a review. Acta Biomater 4(4): 773-782.
- Wu S, Liu X, Hu T, Chu PK, Ho JP, et al. (2008) A biomimetic hierarchical scaffold: natural growth of nanotitanates on three-dimensional microporous Ti-based metals. Nano Lett 8(11): 3803-3808.
- Haugen HJ, Monjo M, Rubert M, Verket A, Lyngstadaas SP, et al. (2013) Porous ceramic titanium dioxide scaffolds promote bone formation in rabbit peri-implant cortical defect model. Acta Biomater 9(2): 5390-5399.
- Wohlfahrt JC, Monjo M, Rnold HJ, Aass AM, Ellingsen JE et al. (2010) Porous titanium granules promote bone healing and growth in rabbit tibia peri-implant osseous defects. Clin Oral Implants Res 21(2): 165-173.
- Reiner T, Kababya S, Gotman I (2008) Protein incorporation within Ti scaffold for bone ingrowth using Sol-gel SiO2 as a slow release carrier. J Mater Sci Mater Med 19(2): 583-589.
- Bobe K, Willbold E, Morgenthal I, Andersen O, Studnitzky T, et al. (2013) In vitro and in vivo evaluation of biodegradable, open-porous scaffolds made of sintered magnesium W4 short fibres. Acta Biomater 9(10): 8611-8623.
- Chou DT, Wells D, Hong D, Lee B, Kuhn H, et al. (2013) Novel processing of iron-manganese alloy-based biomaterials by inkjet 3-D printing. Acta Biomater 9(10): 8593-8603.
- Li X, Xie I, Lipner J, Yuan X, Thomopoulos S, et al. (2009) Nanofiber scaffolds with gradations in mineral content for mimicking the tendon-to-bone insertion site. Nano Lett 9(7): 2763-2768.
- Nandakumar A, Yang L, Habibovic P, Blitterswijk CV (2010) Calcium phosphate coated electrospun fiber matrices as scaffolds for bone tissue engineering. Langmuir 26(10): 7380-7387.
- Moroni L, Schotel R, Hamann D, de Wijn JR, van Blitterswijk CA (2008) 3D fiber deposited electrospun integrated scaffolds enhance cartilage tissue formation. Adv Funct Mater 18(1): 53-60.
- Yang F, Both SK, Yang X, Walboomers XF, Jansen JA (2009) Development of an electrospun nano-apatite/PCL composite membrane for GTR/GBR application. Acta Biomater 5(9): 3295-3304.
- Reichert JC, Wullschleger ME, Cipitria A, Lienau J, Cheng TK, et al. (2011) Custom-made composite scaffolds for segmental defect repair in long bones. Int Orthop 35(8): 1229-1236.
- Geng F, Tan L, Zhang B, Wu C, He Y, et al. (2009) Study on -TCP coated porous Mg as a bone tissue engineering scaffold material. J Mater Sci Technol 25(1): 123-129.
- Barrere F, van der Valk CM, Meijer G, Dalmeijer RA, de Groot K, et al. (2003) Osteointegration of biomimetic apatite coating applied onto dense and porous metal implants in femurs of goats. J Biomed Mater Res B Appl Biomater 67(1): 655-665.
- Xie H, Wang Q, Ye Q, Wan C, Li L (2012) Application of K/ Sr co-doped calcium polyphosphate bioceramic as scaffolds for bone substitutes. J Mater Sci Mater Med 23(4): 1033-1044.
- Lagoa AL, Wedemeyer C, von Knoch M, Löer F, Epple M (2008) A strut graft substitute consisting of a metal core and a polymer surface. J Mater Sci Mater Med 19(1): 417-424.
- Helary G, Noirclere F, Mayingi J, Migonney V (2009) A new approach to graft bioactive polymer on titanium implants: Improvement of MG 63 cell differentiation onto this coating. Acta Biomater 5(1): 124-133.





