Needs and Demands in Prosthetic Treatment in the Population Followed within the Prosthetic Department of Casablanca’s Dental Consultation and Treatment Center
Amine M1*, Azzaz A2, Bouhaji M3, Saif. S2, Serrhier Z4, Bennani A5, Andoh A6
1 Associate Professor, Fixed Prosthesis Department, Faculty of Dentistry of Casablanca, Hassan II University of Casablanca, B.P 9157 Mers Sultan, Casablanca, Morocco.Casablanca’s Dental Consultation and Treatment Center, CHU Ibn Rochd, Casablanca, Morocco.
2 DMD from the Faculty of Dentistry of Casablanca, Hassan II University of Casablanca, B.P 9157 Mers Sultan, Casablanca, Morocco.
3 Resident, Medical Informatics Department, Faculty of Medicine and Pharmacy of Casablanca, Hassan II University of Casablanca , B.P. 9154 Mers
Sultan, Casablanca, Morocco.
4 Associate Professor, Medical Informatics Department, Faculty of Medicine and Pharmacy of Casablanca, Hassan II University of Casablanca, B.P. 9154 Mers Sultan, Casablanca, Morocco.
5 Professor of higher education, Fixed Prosthesis Department, Faculty of Dentistry of Casablanca, Hassan II University of Casablanca, B.P 9157 Mers Sultan , Casablanca, Morocco.Casablanca’s Dental Consultation and Treatment Center, CHU Ibn Rochd, Casablanca, Morocco.
6 Professor of higher education, Biology and Fundamental Matieres Department, Faculty of Dentistry of Casablanca , Hassan II University of Casablanca, B.P 9157 Mers Sultan , Casablanca, Morocco.Casablanca’s Dental Consultation and Treatment Center, CHU Ibn Rochd, Casablanca, Morocco.
*Corresponding Author
Meriem Amine,
Associate Professor, Fixed Prosthesis Department,
Faculty of Dentistry of Casablanca, Hassan II University of Casablanca,
B.P 9157 Mers Sultan, Casablanca, Morocco.
Tel: 00212 665 012 021
Email: meriemamine@hotmail.com
Received: February 01, 2016; Accepted: February 24, 2016; Published: February 27, 2016
Citation: Meriem Amine et al., (2016) Needs and Demands in Prosthetic Treatment in the Population Followed within the Prosthetic Department of Casablanca’s Dental Consultation and Treatment Center. Int J Dentistry Oral Sci. 03(2), 200-204. DOI : dx.doi.org/10.19070/2377-8075-1600042
Copyright: Meriem Amine© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Patient satisfaction in dental prosthetics starts with a better programmation of the treatment plan, which requires a good knowledge of the real needs and demands of patients regarding prosthetic treatment.
The aim of this study was to describe the needs and demands of prosthetic treatment in the population followed in the prosthetic department within Casablanca’s Dental Consultation and Treatment Center (DCTC).
Material and Methods: A descriptive cross-sectional epidemiological study was conducted in the department of prosthetics of Casablanca’s DCTC using a modified World Health Organization (WHO) questionnaire, 457 patients of both sexes were examined over a 2 months period.
Results: The study showed the following results:
- From a general epidemiological point of view, women are more likely to attend the DCTC than men with a consultation rate of 60%. Most subjects are young with an age range between 35 and 44 years. The establishment of the Medical Assistance Plan of the Economically Deprived at DCTC attracts patients with low economic income.
- Clinical data showed that the function is the main reason behind consultation with 51.6% of applications. More than 65.4% of the subjects have never worn prosthesis in the maxilla and 77.5% in the mandible, mainly because of lack of information or lack of financial resources. Among rehabilated patients, those with removable dentures were most frequently found.
An increased total and partial denture despite interest rates need is noted.
Conclusion: Using the results of this study would help to establish a health program that takes into account the specific request of the population followed the DCTC to meet their important needs dentures.
2.Introduction
3.Materials and Methods
3.1.Ethical approval
4.Results
5.Discussion
6.Conclusions
7.Conflict of interest
8.References
Keywords
Needs and Demands; Prosthetic Dentistry; Edentulous.
Introduction
Oral health is one of the major challenges for the welfare of each individual. It contributes significantly to the quality of life. Poor oral health and tooth loss affect not only the nutritional status and phonetics, but also the overall health of individuals [16]. For centuries, the preservation of the teeth was considered a matter of first concern and the ultimate goal in our profession. But however despite the progress that has been in dentistry, tooth loss is still increasing especially in developing countries.
Edentulism, this serious public health problem is the result of several factors. The late checking up is one of these factors, either because of negligence or limited access to dental care [2].
Another factor exists, the aging of the population, which is one of the most significant events of the twenty-first century [8, 9] .
Since any "health problem" is translated into "health needs", the prosthetic rehabilitation needs are a concern within the population. Identifying these problems and these needs, population’s expressed or diagnosed (demands) is one of the first steps in planning dental treatment.
Few studies have been conducted in Morocco aiming denture demand correlated with identified needs of the population in this area.
The aim of this study is to describe the needs and demands in prosthetics of the population followed within the department of removable and fixed prosthesis in the DCTC of Casablanca.
Materials and Methods
A descriptive and comparative study was performed in the department of removable and fixed prosthesis in the DCTC of Casablanca, over a two months period (February and March 2013).
Including all patients aged over 18 years, followed up and treated in the prosthetic departments during this period.
Patients consulting for temporo-mandibular disorders or loss of maxillary substance were excluded from the study.
Data was collected by a single investigator using a questionnary based on the assessment of the Oral Health by the World Health Organization (WHO).
A preliminary investigation had been conducted on twenty patients before the start of this study. It helps investigator to be more familiar with the conditions of investigation, to validate the criteria that will be used, to identify the potential problems and to avoid errors during coding.
Data were processed using Epi Info 3.5.1 software.
This study was approved by the committee of thesis considered as an ethic committee at our University. Informed consent was obtained from patients participating in the study.
Results
In this study 457 subjects were included, 60% were female. The mean age was 45.9 +/- 15.0 years; 22.8% were aged between 35- 44 years, 21.0% were aged between 45-54 years, 22.1% were aged 55-64 years, while only 6.1% of patients were aged 65-74 ans.
The monthly household income was less than 2800 Morrocan Dirhams (DHM) in 65.6% of patients, between 2800 and 6736 in 29.8% and more than 6736 DHM in 4.6% of patients.
Illiteracy (lack of school education) was reported in 31.9% of subjects, 26.3% had a primary level, secondary level found in 25.6% and only 16.2% had a higher intellectual level.
75.5% of patients had a social security cover. 77.9% were covered by the Plan for Medical Assistance for the Economically Deprived, 11.1% covered by the National Fund of Social Welfare Organizations), 9.3% covered by the National social Security Fund and only 1.7% had another health insurance.
The reason behind consultation was purely functional in 51.6% of subjects, was purely aesthetic in 23% of the cases and in 25. 4% both reasons were combined (Table 1).
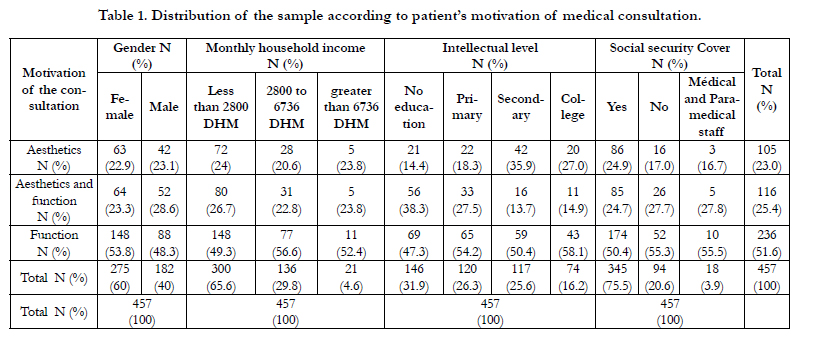

Table 1. Distribution of the sample according to patient’s motivation of medical consultation.
The fixed prosthesis demand was expressed by 55.4% of subjects,43.8% requested rehabilitation using removable prosthesis, while only 0.8% requested an implant supported prosthesis (Table 2).
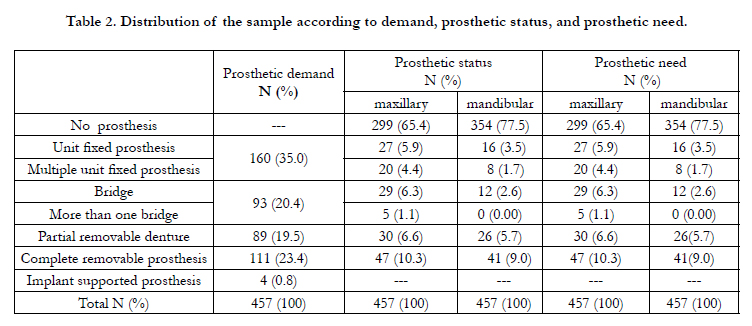
Table 2. Distribution of the sample according to demand, prosthetic status, and prosthetic need.
The distribution of status and prosthetic need in maxilla and mandible is showed in Table 2.
There is a predominance of non-wearing prosthesis with 65.4% in the maxilla and 77.5% in the mandible; followed by the wearing of full dentures with 10.3% in the maxilla and mandible 9%.
Discussion
The study of the population needs and demands is meaningless without an initial study of demographics and socio-economics [16].
The relative youth of the study population highlighted in the results is emphasized in the age pyramid of Casablanca. In addition, young people are more concerned about their appearance and teeth.
Our results showed a disparity in the prosthetic request by sex; female predominance is noted, on one hand accordingly to the distribution of the population of Casablanca in the report of the High Planning Commission; secondly it confirms the results of most of the publications: Paloudier et al., (1987) in France, of Upadhyaya and Humagain (2009) in Nepal, of Djeredou et al., (2003) in Ivory Coast and those of Mbodj EB et al., (2011) in Senegal.
The indication of socio economic level of the population was taken from the report of the High Commissioner for Moroccan planning detailing the socio economic classes according to the monthly household income in Morocco.
Our study revealed the precarious population are consulting in the Department of Prosthodontics (65.6% of subjects have an income less than 2800 DHM monthly).
DCTC apply social tariffs, which attracts low-income populations.
After a review of literature, education is a key factor in prosthesis consultation [2]. The distribution of the study subjects according to the intellectual level shows a predominance of illiterate subjects (31.9%), 26.3% have a primary intellectual level and 25.6% with a secondary intellectual level. Subjects with a higher intellectual level represent a minority with 16.2% of the study population. These results are consistent with the report of the High Planning Commission who noted a high rate of illiteracy among Casablanca’s population with 25%.
In our sample, the functional consultations remain patient’s primary motivation with nearly 51.6%. This is valid for both sexes, and all age categories in the sample regardless of their household income and their intellectual level. The aesthetic and functional motivation comes in second order with a percentage of 25.4%. While the aesthetics remains last with a percentage of 23%.
This shows that the care is requested only in case of obligation, while experiencing a decrease of masticatory function in the study subjects [21].
The prevalence of functional motivation is reported in different studies concerning the prosthetic needs [16-18].
However, other studies reported opposite results when it comes to aesthetic demand [7, 9, 2, 11] which is also linked to age and cultural factors [14].
Regarding the type of prosthesis required, the reason behind consultation, 55.4% of patients received in prosthesis department requested a fixed prosthesis rehabilitation with 43.8% requested rehabilitation by removable prosthesis, and
only 0.8% patients requested implant-supported prosthesis.
Among appliants for fixed prosthesis there was a predominance of single fixed prosthesis with 63.24% against 36.76% for the fixed partial denture.
Based on these results, it appears that more than half of the study sample's chose the fixed prosthesis option despite the high costs of this type of prosthesis and despite the high rate of patients with low incomes. The move towards this type of restoration may be due to its advantages such as aesthetics and durability in time, and the fact that the Medical Assistance Plan of the Economically Deprived support certain types of fixed prosthesis (fixed prosthesis unit) and the quality of services offered within the service of fixed prosthesis.
65.4% of patients were never rehabilitated in the maxilla and 77.5% in the lower jaw.
The main causes why patients do not consult for prosthesis are the lack of information, lack of money, negligence and the impact of cultural considerations [2].
The prosthetic status would be associated with socioeconomic status; a low socioeconomic level is associated with a reduced level of wearing prosthesis in both arches. Vrinda et al., (2012) explained this by the fact that a high socioeconomic level provides better access to dental care.
The prosthetic status is also associated with gender, women wear dentures less than men.
A study conducted by Kuo et al., (2009) on a Taiwanese population combines prosthetic status with age. In his study of a Sudanese population, Khalifa et al., (2012) notes that tooth loss increase with age in females, in a context of low socioeconomic status and low educational level.
In patients who have already been rehabilitated, the total denture is most frequently used, in 10.3% in the maxilla and 9% in the mandible. It is inexpensive and seems more accessible to patients depending on their socio-economic level [6].
The uncompensated edentulous impacts the mastication, nutrition, and on overall health [16], which requires a prosthetic rehabilitation in front of a total loss of teeth, while in case of partially edentulous, chewing is still possible, even in some cases where tooth loss is important [8].
However, about 17.7% are holders of fixed prosthesis in the maxilla and only 7.8% in the mandible.
The low use of fixed prosthesis, is probably due to its high cost, and the lack of support by the mutual insurance companies.
Needs are represented by the level of dental care that the expert considers necessary to restore dental health. It is associated with an individual notion of comfort and quality of life [14].
The need does not necessarily correspond to the demand (expressed need) of prosthetic treatment. It depends on socio-economic, cultural, psychological, individual factors and accessibility of the service [23, 14, 16, 4].
As wearing prosthesis is very low, the additional needs of all categories are important.
The need for prosthesis is associated with socioeconomic level. It would be more important when the socioeconomic level is low and also when the intellectual level is low [4].
The prosthetic needs vary according to gender, it would be more important for men than women, unlike the study conducted by Walter et al., (2001) on a German population and the study of [12] on the Indian population that showed no correlation between the prosthetic need and gender.
In his study of a Saudi population, Al-Ghannam et al., (2002) noted a greater need for full dentures among men and a greater need for fixed partial denture (bridge) in women. Also, prosthetic needs increase with age [13, 23, 9].
Conclusions
Being conducted in a socio-economic crisis and political context (extension of the access to health care), this study shows the paradox between the reality of the oral health status and the need for prosthesis in the population of Casablanca. Using these results, identifying needs in dental prosthesis would help the establishment of a health program in the Greater Casablanca in dental prosthetics.
From this view, we consider that it is necessary to change the need in demand and develop the appropriate mechanisms of respond to this request, taking into account all the factors involved [15].
Conflict of interest
All authors disclose any financial and personal relationships with other people or organizations that could inappropriately influence (bias) their work.
References
- Al-Ghannam NA, Al-Shammery AR, Wyne AH, Khan NB (2002) Prosthetic dental treatment needs in Eastern [corrected] Saudi Arabia. Saudi Med J 23(8): 975-980.
- Djeredou KB, Thiam A, Pesson DM, Bakou OD, Nabe G, et al. (2003) Etude prospective pilote des demandes prothétiques au service de prothèse du CCTOS d'Abidjan. Odonto-Stomatologie Tropicale 103: 4-8.
- Elias AC, Sheiham A (1998) The relationship between satisfaction with mouth and number and position of teeth. J Oral Rehabil 25(9): 649-661.
- Ettinger RL, Beck JD, Jakobsen J (1984) Removable prosthodontic treatment needs: A survey. J Prosthet Dent 51(3): 419-427.
- Galobardes B, Morabia A, Bernstein MS (2000) Statut socio-économique: un facteur de risqué indépendant. Médecine et hygiène 58(2316): 1910- 1913.
- Hescot P, Bourgeois D, Doury J (1997) Oral health in 35-44 year old adults in France. Int Dent J 47(2): 94-99.
- Kayser AF, Witter DJ (1985) Oral functional needs and its consequences for dentulous older people. Community Dent Health 2(4): 285-291.
- Khalifa N, Allen PF, Abu-Bakr NH, Abdel-Rahman ME (2012) Factors associated with tooth loss and prosthodontic status among Sudanese adults. J Oral Sci 54(4): 303-312.
- Kuo HC, Yang YH, Lai SK, Yap SF, Ho PS (2009) The Association between health-related quality of life and prosthetic status and prosthetic needs in Taiwanese adults. J Oral Rehabil 36(3): 217-225.
- Mbodj EB, Diouf M, Faye D, Ndiaye A, Seck MT, et al. (2011) La réhabilitation prothétique : évaluation des besoins dans les cabinets dentaires du Sénégal Bull Soc Pathol Exot 104(5): 355-356.
- Mukatash GN, Al-Rousan M, Al-Sakarna B (2010) Needs and demands of prosthetic treatment among two groups of individuals. Indian J Dent Res 21(4): 564-567.
- Nadgere J, Doshi AG, Kishore S (2010) An Evaluation of Prosthetic Status and Prosthetic Need amongst people living in and around Panvel, Navi-Mumbai-A Survey. Int J of Prosth Dent 1(1): 6-9.
- Napankangas R, Salonen MA, Raustia AM (2001) Treatment need for fixed metal ceramic bridge prostheses in patients treated by dental students in 1984-1996. J Oral Rehab 28(12): 1101-1105.
- Narby B, Kronström M, Söderfeldt B, Palmqvist S (2005) Prosthodontics and the patient: what is oral rehabilitation need? Conceptual analysis of need and demand for prosthodontic treatment. Part 1: a conceptual analysis. Int J Prosthodont 18(1): 75-79.
- Narby B, Kronström M, Söderfeldt B, Palmqvist S (2007) Prosthodontics and the patient. Part 2: Need becoming demand, demand becoming utilization. Int J Prosthodont 20(2): 183-189.
- Naveeda I, Fazal G (2008) Demands, needs, expectations, patterns and reasons among patients for treatment with fixed dental prostheses. JPMI 22(4):313-319.
- Paloudier G, Brodeur JM, Baron P (1987) Approche des facteurs de la consommation prothétique. Prév Bucco-Dent 1(2): 51-57.
- Reddy NS, Reddy NA, Narendra R, Reddy SD (2012) Epidemiological survey on edentulousness. J Contemp Dent Pract 13(4): 562-570.
- Thomas-Weintraub A (1985) Dental needs and dental service use patterns of an elderly edentulous population. J Prosthet Dent 54(4): 526-532.
- Upadhyaya C, Humagain M (2009) The pattern of tooth loss due to dental caries and periodontal disease among patients attending dental department (OPD), Dhulikhel Hospital, Kathmandu University Teaching Hospital (KUTH), Nepal. Kathmandu Univ Med J 7(25): 59-62.
- Vigild M (1987) Denture status and need for prosthodontic treatment among institutionalized elderly in Denmark. Community Dent Oral Epidemiol 15(3): 128-133.
- Shah VR, Shah DN, Parmar CH (2012) Prosthetic Status and Prosthetic Need Among the Patients Attending Various Dental Institutes of Ahmedabad and Gandhinagar District, Gujarat. J Indian Prosthodont Soc 12(3): 161-167.
- Walter MH, Wolf BH, Rieger C, Boening KW (2001) Prosthetic treatment need in a representative German sample. J Oral Rehabil 28(8): 708-716.
- www.hcp.ma/downloads/Demographie-Caracteristiques-demographiques-et-socio-economiques-RGPH-2004_t13063.html





