Dermatoglyphics as a Non-Invasive Anatomical Marker in Early Childhood Caries
Wahdan M. Elkwatehy1*, Abdel Razek A Sheta2
1 Faculty of Dentistry, Department of Public Health and Preventive Dentistry, Mansoura University (Egypt) and Umm Al-Qura University (KSA).
2 Faculty of Medicine, Department of Anatomy & Embryology; Tanta University (Egypt) & Faculty of Dentistry, Umm Al-Qura University (KSA).
*Corresponding Author
Wahdan M Elkwatehy,
Faculty of Dentistry, Department of Public Health and Preventive Dentistry,
Mansoura University (Egypt) and Umm Al-Qura University, Saudi Arabia.
Tel: 00966582396965
Fax: 582396965
E-mail: wahdanelkwatehy@yahoo.com
Received: October 12, 2016; Accepted: November 21, 2016; Published: November 23, 2016
Citation: Elkwatehy WM, Abdel Razek A Sheta (2016) Dermatoglyphics as a Non-Invasive Anatomical Marker in Early Childhood Caries. Int J Dentistry Oral Sci. 3(11), 366-371. doi: dx.doi.org/10.19070/2377-8075-1600074
Copyright: Elkwatehy WM© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background/Aim: Dermatoglyphics is supposed to be influenced by genetic and environmental factors and so also dental caries. Therefore, the present investigation was undertaken to find out a possible relation between some quantitative and qualitative dermatoglyphic variables and early childhood caries (ECC).
Materials and Methods: The study was conducted on 200 children in age group of 3 to 6 years from two private kindergarten, Egypt, and divided into 2 equal groups i.e. caries active group (n=100) and caries free group (n=100). The caries active group included children with dmft index = 4 or more and caries free group consist of normal, healthy children without any dental caries. The finger prints of both hands were taken using a stamp pad method then qualitative and quantitative data of dermatoglyphics were analyzed.
Results: There was increase in frequency of whorls and decrease in frequency of loops in caries active group when compared to caries free group which was statistically significant (p = 0.000). The total finger ridge counts of whorls was higher in caries active children while total finger ridge counts of loops and the atd angles were higher in caries free children. The differences were statistically significant (p = 0.000).
Conclusion: Early childhood caries susceptibility of an individual increased with increased frequency of whorl pattern but it decreased with increased frequency of loop pattern and increased atd angle.
2.Introduction
3.Aim of the Work
4.Materials and Methods
4.1.Study Design
4.2.Method of Collection of Data
4.3.Qualitative Dermatoglyphic Analysis
5.Quantitative Dermatoglyphic Analysis
5.1.Ridge Count of the Fingers
5.2.‘atd’ Angle
6.Statistical Analysis
7.Results
8.Discussion
9.Conclusion
10.Recommendation
11.Acknowledgements
12.References
Keywords
Dermatoglyphics; Finger Prints; Early Childhood Caries.
Introduction
Dermatoglyphics refers to study of the intricate dermal ridge configurations on the skin covering the palmar and plantar surfaces of hand and feet. It is a branch of physical anthropology, medicine and genetics. Dermatoglyphic patterns are assumed to be genetically controlled although the exact mechanism of inheritance is still unknown [1]. After their complete formation, they are unaffected by the environment, and this explains their unique role as an ideal marker for individual identification and the study of populations, as well as detection of defects due to intra-uterine irregularities in the early weeks of pregnancy. However it is still at infancy in the world of dentistry where the co-relation of dental conditions with that of dermatoglyphic patterns is done [2-5].
Dental caries represents a common disease of the teeth, and is prevalent worldwide. The etiology of dental caries is multifactorial with genetic predisposition blamed as one [6]. Different studies have been conducted by various investigators to find out the relation between dermatoglyphic pattern variations and dental caries [7-13].
Atasu et al., [7] studied dermatoglyphic configurations in caries free students and the students with extensive caries and found there was significant difference in dermatoglyphic patterns in these two groups as caries free students had more ulnar loops on the fingertips and the students with extensive caries had more whorls on the finger tips.
Sharma and Somani [8] found highly significant difference in loops between the subject (Caries) and control groups, and also observed significant difference between subject and control groups for microbial growth.
Bhat et al., [9] conducted a study to evaluate dermatoglyphic peculiarities and caries experience of deaf and mute children. They observed that the frequency of whorls was more in caries group and the frequency of the loop was more in caries free group. Another study was done by Madan et al., [10] determine the genetic aspect involved in the occurrence of dental caries through a costeffective means. They observed that Handprints of caries free children, especially females, showed maximum ulnar loops. The caries group showed maximum occurrence of whorls which were more prevalent in females on the left hand 3rd digit than in males where the whorls were found on the right hand 3rd digit, and also low total ridge count, especially in males.
Dermatoglyphics is a simple and inexpensive clinical test and research tool. The economical and feasible nature of this diagnostic tool may be used in screening of a variety of pathologies. Genetically predisposed individuals can be segregated, counseled accordingly and motivated to change the lifestyle. The expenses associated with genetic cytomarker studies may thus be prevented. With the help of simple tool, the frequency of developing serious diseases in later life may be prevented or postponed thereby extending the longevity of an individual [11].
As dermatoglyphic patterns developed at birth and there after remain unchanged for life, also, scanning or recording of their permanent impressions can be accomplished rapidly, inexpensively, conveniently and without causing any trauma to the patient or hospitalization [4]. So, dermatoglyphic may sometimes play a significant role in the diagnosis of dental diseases like caries. Therefore, the present study was conducted in vivo to establish a unique correlation between the dermatoglyphics patterns and its relation to early childhood caries.
Aim of the Work
The present study was undertaken to evaluate the significances of dermatoglyphics in predicating the susceptibility of individual to develop early childhood caries.
Materials and Methods
The present study was conducted in two private kindergartens, Kfr Elshikh, Egypt. Written informed consent was obtained from the parents and respective kindergarten authorities.
The present study was a case control study. The sample consisted of 200 children aged between 3 and 6 years, divided into two groups of 100 children each. The dmft score was evaluated to select the experimental group which included children with dmft score = 4 or more and control group which contained children with no caries. The present study did not include the dermatoglyphics of children with syndromes as they may show a peculiar pattern of development of dermal ridges.
Firstly, hands were thoroughly cleaned and allowed to dry. After this, right hand four digits were guided by the researcher to the ink stamp pad and pressed firmly against the bond paper. Also, the palm of clean dried hands were smeared with the ink and pressed against the paper to show the palmar ridges and inter digital areas. The paper was stabilized on a hard smooth surface board. Sometimes impressions were recorded 3 times, to reach the most satisfactory and readable one. Then this was done also for the thumb of the same hand. The same procedure was repeated for the left hand. These dermatoglyphic patterns were analyzed with the help of a magnifying glass (6 xs).
The frequency of true patterns of loops, whorls and arches (Figure 1) were counted on the fingertips of all the 10 digits of children with dental caries and caries free children. They were assessed for increase or decrease in frequencies. Fingerprint patterns in the present study included three main types: whorls, loops, and arches. Under these major types, other subtypes were also noticed and considered normal anatomical variations. The whorl is distinguished by its concentric design. In arches, the dermal ridges pass from one margin of the digit to the other with a gentle, distally bowed sweep. In loops, the ridges curve around only one extremity of the pattern forming the head of the loop. Loops can be further divided into ulnar and radial types: ulnar loop when the loop opens to the ulnar margin of the hand and radial loop when the loop opens to the radial margin. A triradius is located at the meeting point of three opposing ridge system. This marks the edge of the loop pattern as it possesses only one triradius. In arch pattern, there is no triradius while whorls usually have two triradii.
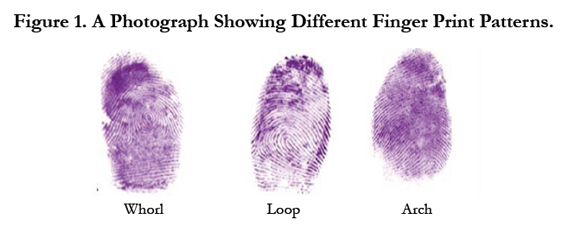

Figure 1. A Photograph Showing Different Finger Print Patterns.
Quantitative Dermatoglyphic Analysis
Ridge counts for each fingertip were calculated from the number of primary epidermal ridges that intersected or touched the straight line drawn from the central core of the fingerprint pattern to the bifurcation of the triradius (Figure 2). The count on the ten fingers of each individual is then summed up to give a single mean value of the total ridge count. Consistent with standard methods, fingertips with an arch pattern were assigned a ridge count of zero. Fingertips with a loop pattern have a ridge count equal to the number of ridges crossing the single straight line. For fingertip patterns with two triradial points e.g., whorls, the following ridge counting protocol was used according to Kahn et al., [12]: ridge count = ridges crossing the longer line + half of ridges crossing the shorter line.
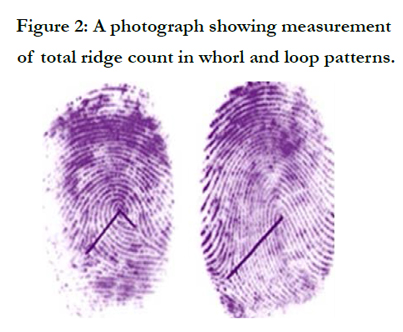

Figure 2: A photograph showing measurement of total ridge count in whorl and loop patterns.
The ‘atd’ angle is a trait of the palm that reveals the position of three triradii-‘a’ and ‘d’, usually located on distal palm just inferior to the 2nd and 5th fingers, respectively and ‘t’ whose location can vary on the proximal palm from just distal to the wrist, up to the center of the palm. The atd angles (Figure 3) were measured for each palm print by drawing two straight lines through the ‘a’ and ‘t’ triradii and the ‘d’ and ‘t’ triradii and measuring the resulting angle. The atd angles were compared and assessed for increase or decrease between the groups [13].
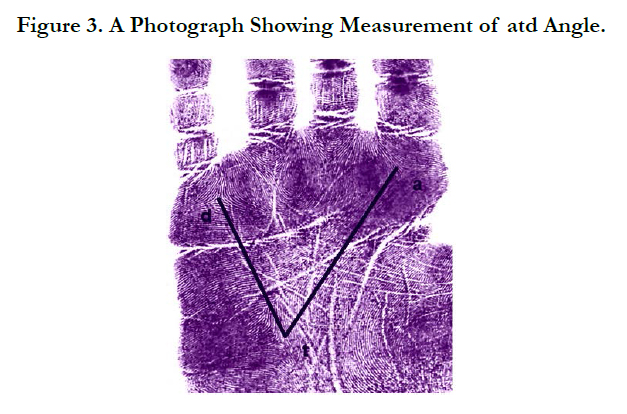

Figure 3. A Photograph Showing Measurement of atd Angle.
Statistical Analysis
The collected data were organized, tabulated and statistically analyzed using SPSS software statistical computer package, version 22. The qualitative data was presented as frequencies and compared by Chi square test, the quantitative data was presented as mean and standard deviation (SD) and compared by independent student t test. The differences between the two groups were considered significant at P < 0.05.
Results
The comparison of frequency of loops, whorls and arch pattern for both groups is shown in Table 1 and Graph 1. Caries active group had an increased frequency of whorls and a decreased frequency of loops while Caries free group had a decreased frequency of whorls and increased frequency of loops. When both groups were compared, there were statistically significant differences (p = 0.000).
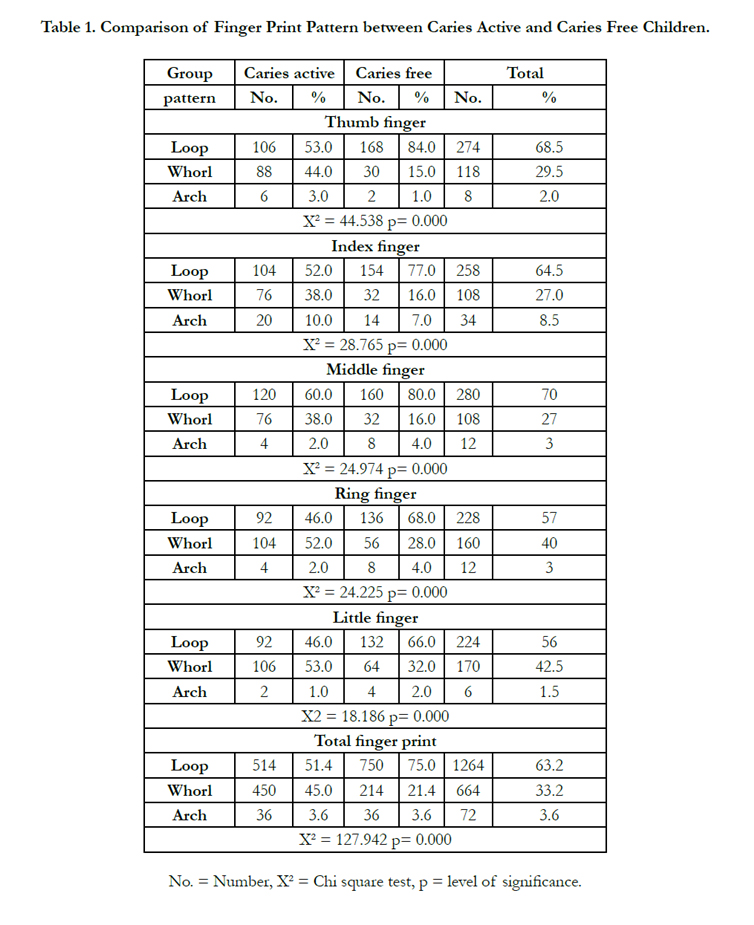

Table 1. Comparison of Finger Print Pattern between Caries Active and Caries Free Children.
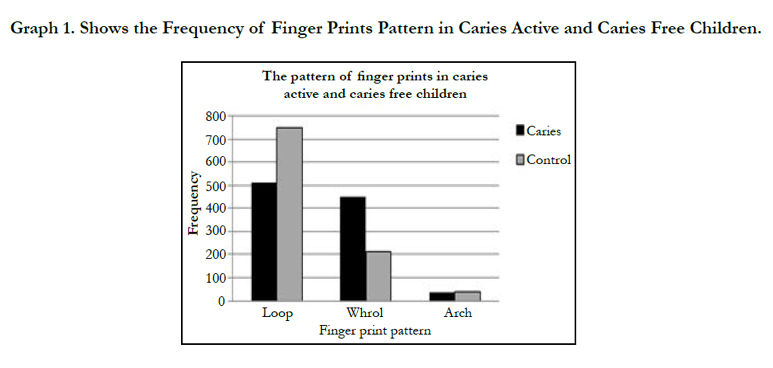
Graph 1. Shows the Frequency of Finger Prints Pattern in Caries Active and Caries Free Children.
The comparison of mean values of total finger ridge count for loops and whorls and the mean atd angle for both groups is shown in Table 2. The mean value of loops in caries active group was 5.89 ± 1.15 and that for caries free group was observed to be 8.26 ± 1.05. The mean value of whorls in caries active group was observed to be 8.11 ± 1.08 and that for caries free group it was 4.73 ± 0.94. The mean value of atd angle in caries active group was noticed to be 49.93 ± 5.01 and that for caries free group it was 53.06 ± 4.55. When both groups were compared, there were high statistically significant differences (p = 0.000) as regards the mean values of loops and whorls ridge counts and atd angle.
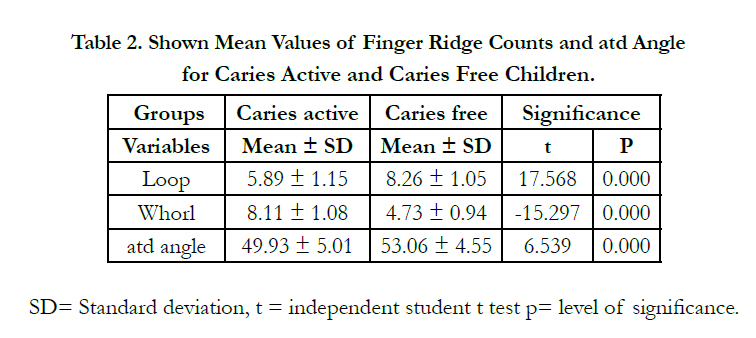
Table 2. Shown Mean Values of Finger Ridge Counts and atd Angle for Caries Active and Caries Free Children.
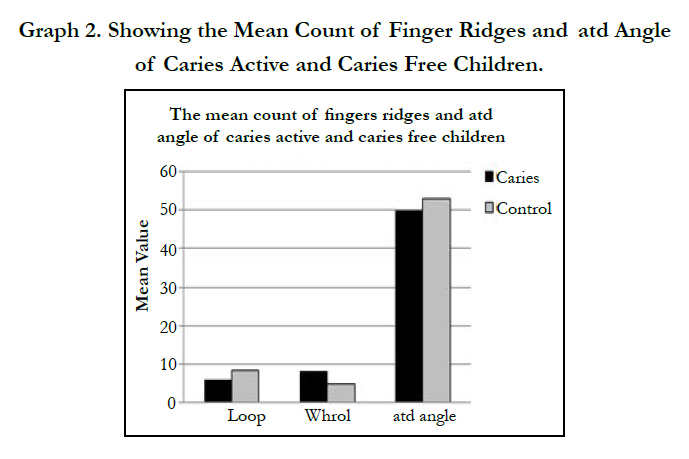
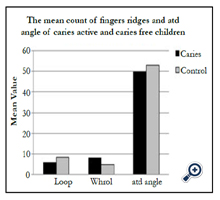
Graph 2. Showing the Mean Count of Finger Ridges and atd Angle of Caries Active and Caries Free Children.
Discussion
Dental caries is a chronic, complex, multifactorial disease for which a number of causative agents like host and environmental factors have been proposed. There are numerous host factors for dental caries that are genetically determined [14, 15]. The pattern of dental caries has been found to be similar in members of the same family over several generations and hence, inheritance of this susceptibility is suspected. Genetic variations in the host factors may contribute to increased risks for dental caries. The dermatoglyphic patterns can be used as an oral health marker, which can determine the genetic predisposition of children to dental caries [7, 16]. The type of fingerprints is unique and is based on the genetic constitution of each individual. These dermal patterns once formed remain constant throughout life and also are considered to be unique for a person [17, 18].
In the present study when the 400 hand prints of 200 children were analyzed (Table 1), it was found that there was an increased frequency of loops (63.2%) among this study population followed by whorls (33.2%) and arches (3.6%). These findings are consistent with the previous studies [14, 19] regarding frequency of dermatoglyphic patterns in a population.
The results of the present study indicate that, Caries active group showed increased frequency of whorls as compared to frequency of whorls present in caries free group and also showed that caries active group had a decreased frequency of loops as compared to loops present in caries free group (Table 1). These results are coinciding with the results obtained by Atasu et al., [7] and Vijender et al., [20].
Also, there was highly statistically significant total finger ridge count of whorls in caries active children while there was highly statistically significant total finger ridge count of loops in caries free children (Table 2). These results were agreed with the results concluded by Sengupta et al., [11].
The results of the present study showed statistically significant difference between caries active and caries free children as regards atd angle where the atd angle was larger in caries free (53 ± 4.55) than caries active children (49.9 ± 5.01) (Table 2). These results were corroborated with the findings of previous studies which stated that the caries free children had larger atd angle than that of the children with extensive caries [6, 7]. On the other hand these results were disagreed with the results obtained by Navit et al., [14] where they found that the mean atd angle in caries free children and children with ECC was almost similar (Mean atd angle for children with ECC was 44.60 and caries free children was 44.80). The disparity of result could be due to the variation in sample size and methodology employed. The sample size for the present study included 200 children of 3-6 years whereas in the study performed by Navit et al., [21] a sample size was 100 children. Also, the size of the atd angle may be affected with the spreading of fingers while recording the pattern [7].
Basically, the pattern of the skin lines on the finger is formed during the second trimester of the intrauterine life and it does not change for any individual during the life. It has been reported that the epidermal ridges of the fingers, the palms and facial structures like lip, alveolus, palate and tooth bud are formed from the same embryonic tissue (ectomesenchyme) during the same embryonic period (6-9 weeks) [22]. The genetic constitution whether normal or abnormal is deciphered during this period and is reflected by dermatoglyphics. Thus, with genetic information, the susceptibility for caries due to abnormality in the tooth structures like alterations in dental hard tissues like structure of dental enamel, tooth eruption and development may be reflected in the dermatoglyphics namely whorl and loop patterns [2, 7, 18]. Hence, dermatoglyphics could be an indicator of genetic susceptibility of an individual to early childhood caries.
Conclusions
From the present study it was found that there was a significant association between fingerprint patterns and early childhood caries. Studies done earlier support that dermatoglyphic pattern is linked with early childhood caries which might be a valuable, noninvasive anatomical tool which could be used for screening for early childhood caries and for guiding future research. This may further seek to introduce of more preventive, early diagnosis and effective treatment strategies in patients with early childhood caries.
Recommendation
Further extensive research and studies in the field of dermatoglyphic have to be done in order to determine and to evaluate the significance of these variations in the dermatoglyphic features of patients with early childhood caries.
Acknowledgements
The authors wish to thank the authority of kindergartens and children parents for their cooperation.
References
- Galton F (1892) Finger prints. McMillan: London.
- Soni A, Singh SK, Gupta A (2013) Implications of Dermatoglyphics in Dentistry. 2(2): 27-30.
- Prabha L, Thenmozhi R. (2014) A Short Review on Dermatoglyphics. J Pharm Sci Res. 6(4): 200-202.
- Prabhu N, Issrani R, Mathur S, Mishra G, Sinha S (2014) Dermatoglyphics in Health and Oral Diseases-A Review. JSM Dent; 2(4): 1044-1448.
- Devi MP, Shah S, Ravindra SV, Bajantri N, Singh D (2015) Skin Carvings: Predictive Diagnosis in Modern Era. IJSS Case Reports & Reviews. 1(10): 75-80.
- Anitha C, Konde S, Raj N S, Kumar NC, Peethamber P (2014) Dermatoglyphics: a genetic marker of early childhood caries. J Indian Soc Pedod Prev Dent. 32(3): 220-224.
- Atasu M (1998) Dermatoglyphic findings in dental caries: a preliminary report. J Clin Pediatr Dent. 22(2): 147-149.
- Sharma A, Somani R (2009) Dermatoglyphic interpretation of dental caries and its correlation to salivary bacteria interactions – An in vivo study. J Indian Soc Pedod Prev Dent. 27(1): 17-21.
- Bhat PK, Badiyani B K, Aruna CN, Chengappa S, Bhaskar NN (2011) Dermatoglyphics – A new diagnostic tool in detection of dental caries among deaf and mute children. Int J Clin Dent Sci. 2(4): 80-84.
- Madan N, Rathnam A, Bajaj N (2011) Palmistry A tool for dental caries prediction!. Indian J Dent Res. 22(2): 213-218.
- Sengupta AB, Bazmi BA, Sarkar S, Kar S, Gosh C, et al., (2013) Cross sectional study of dermatoglyphics and dental caries in Bengalee children. Journal of Indian Soc Pedod Prev Dent. 31(4): 245-248.
- Kahn HS, Ravindranath R, Valdez R and Venkat K (2001) Fingerprint ridge-count difference between adjacent fingertips (dR45) predicts upperbody tissue distribution: evidence for early gestational programming. American J Epidemiol. 153 (4): 338-344.
- Holt SB (1979) Epidermal ridge counts. Coll Antropol. 3(1): 97-106.
- Hassel TM (1995) Genetic influences in caries and periodontal diseases. Oral Biol Med. 6(4): 319-342.
- Nariyama M1, Shimizu K, Uematsu T, Maeda T (2004) Identification of chromosomes associated with dental caries susceptibility using quantitative trait locus analysis in mice. Caries Res. 38(2): 79-84.
- Cummins (1929) Revised methods of interpretation and formulation of palmar dermatoglyphics. Am J Phy Anthr. 12(3): 415- 502.
- Campbell ED (1998) Fingerprints and palmer dermatoglyphics. Efingerprints net.
- Abhilash PR, Divyashree R, Patil SG, Gupta M, Chandrasekar T, e al., (2012) Dermatoglaphyics in patient with dental caries: A study on 1250 individuals. J Contmp Dent Pract. 13(3): 266-274.
- Ahmed I, Yasin I (2010) Dermatoglyphic pattern study. AMPC. 4(2):107- 110.
- Vijender V, Tarannum T, Pathak A (2015) Dermatoglyphics Interpretation of Dental Caries: An In Vivo Study. Int J Dent Med Res. 1(6): 54-56.
- Navit S, Chadha D, Khan SA, Singh RK, Johri N, et al., (2015) The Mystery of Handprints: Assesment and Correlation of Dermatoglyphics with Early Childhood Caries A Case-Control Study. J Clin Diagn Res. 9(10): 44 – 48.
- Lin CH, Liu JH, Osterburg JW, Nicol JD (1982) Fingerprint comparison I: Similarity of fingerprints. J Foren Scie. 27(2): 290 - 304.





