The Supple Elucidation of Neutral Zone by Tissue Conditioners - A Case Report
Dubey PK1*, Sethuraman R2
1 Consultant Prosthodontist, The Dental Evolution, Varanasi (U.P.), India.
2 Professor, Department Of Prosthodontics, K.M. Shah Dental College And Hospital, Vadodara, Gujarat, India.
*Corresponding Author
Dr. Pavan Kumar Dubey,
Consultant Prosthodontist,
The Dental Evolution, S-8/211-1k, Sudhakar Road,
Khajuri, Varanasi (U.P.), 221002,
India.
E-mail: drpavan26@gmail.com
Article Type : Case Report
Received: July 30, 2015; Accepted: August 26, 2015; Published: September 10, 2015
Citation: Dubey PK, Sethuraman R (2015) The Supple Elucidation of Neutral Zone by Tissue Conditioners -A Case Report. Int J Dentistry Oral Sci. 2(9), 155-157. doi: dx.doi.org/10.19070/2377-8075-1500032
Copyright: Dubey PK© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Tissue conditioners are indicated to condition the abused tissue, whereas soft liners are indicated to give a cushioning effect to relieve and protect vulnerable tissues. However they also prove their utility in the fabrication of stable dentures by recording the physiologic muscle movement of tongue and cheek muscle, hence customarily establishing the neutral zone of edentulous arch.
2.Introduction
3.Neutral zone
4.Tissue conditioners
4.1.Indications for the use of tissue conditioners
4.2.Contraindications
4.3 The major uses of these tissue conditioning materials include
4.3 Procedure for Applying Tissue Conditioners
4.4 Care and Maintenance
5.Summary and Conclusion
6.Case Report – Determination Of Neutral Zone Using Tissue Conditioner
7.References
Keywords
Tissue Conditioning; Denture Stability; Neutralization of Forces.
Introduction
The stable position of the teeth represents equilibrium of all the forces acting on them. If that position of equilibrium namely the neutral zone, is not found, the resulting dentition will not last long and will not be esthetically pleasing and the patients use of functional efficiency, maximum length of use and pleasing esthetics will not have been met. The role of tissue conditioners proves to be very accurate for determining the desired space named neutral zone. Before we employ this material we must have sufficient information about this material as to ascertain their odds and evens.
Neutral zone
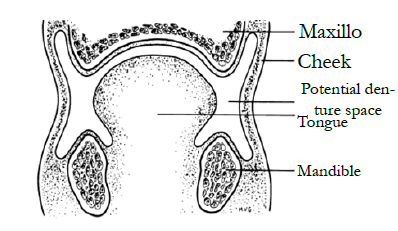
Neutral Zone is defined as that area in the mouth where, during function, the forces of the tongue pressing outward are neutralized by the forces of the cheeks and lips pressing inwards.
Russel (1959) [1] who termed it as “Reciprocal space”, Robert (1960) [2] called it the “Potential space”, Heath (1970) [3] as “Denture space” Bates (1984) as “Reciprocal zone”, Mathew (1961) [4] as “Zone of minimum conflict” and Fenn (1986) [5] termed it “Zone of neutral muscular forces”.
Figure
The soft tissues that form the internal and external boundaries of the denture space exert forces which greatly influence the stability of the dentures. The central thesis of the neutral-zone approach to complete dentures is to locate that area in the edentulous mouth where the teeth should be positioned so that the forces exerted by muscles will tend to stabilize the denture rather than unseat it [6]. Heath (1970) [3] has demonstrated that there is a difference in the shape of the denture space and resultant arch form at rest as compared to the denture space and arch form established by function. The neutral zone is that area in the mouth where, during function, the forces of the tongue pressing outward are neutralized by the forces of the cheeks and lips pressing inward. Since these forces are developed through muscles contraction during the various functions of chewing, swallowing and speaking, they vary in magnitude and direction in different individuals and in different periods of life. The way these forces are directed against the dentures will either help to stabilize them or will tend to dislodge them.
Tissue conditioners
They are elastomer polymers used in the prevention of chronic soreness from denture and preservation of supporting structures. They are made resilient by addition of alcohol type plasticizers or by co-polymerisation with the monomer unit. The hydrophilic polymer is a mixture of polyethylene glycol with diacetins [7]. Plasticized resin materials are the largest group of resilient liners; they are either cold-cure or heat-cure systems, and frequently they depend on the addition of plasticizer for their resilience. A plasticizer eventually leaches out, leaving the material hard and often fissured, thereby promoting staining. Vinyls have short-comings similar to those of resins because they may harden in service gradually. Lower resistance to abrasion also is a problem and may contribute to the poor fit of dentures.
Thin atrophic mucosa underlying denture base, ridge atrophy or resorption, presence of deep anatomical undercuts, chronic bruxers or patients with bruxing tendencies, reduced tolerance level of the mucosa for occlusal loads under denture,acquired or congenital defects which require obturation, presence of bony protruberances, retention of implant retained overdentures.
• Relief areas
• Xerostomia
• Obturators to enhance retention
• Denture opposing natural dentition
• Tissue treatment
• Temporary obturator
• Baseplate stabilization
• To diagnose the outcome of resilient liners
• Liners in surgical splints
• Trial denture base
• Functional impression material
- The following steps should be considered while applying a tissue conditioner on a denture. Preparation of the dentures: The tissue part of the denture base, which crosses an undercut, should be reduced. The tissue surface of the denture, which covers the crest of the ridge, should be reduced by 1 mm. It should be remembered that the dentures should allow sufficient room for the placement of the tissue conditioner in order to promote the recovery of displaced and traumatized tissues.
- Mixing and Placement of the Tissue Conditioner:- Tissue conditioners are available as three component systems.
- 1. Polymer (Powder)
- Monomer (Liquid)
- Liquid plasticizer (Flow control).
Tissue conditioners should not be cleaned by scrubbing with a hard brush in order to prevent tearing of the material [8]. The use of soft brush under running water is recommended. The greatest virtue of tissue conditioners is their versatility and ease of use. Their biggest flaw is that they are so easily misused. Their longevity against wear is very limited and they tend to harden and roughen within 4 to 8 weeks due to the loss of plasticizer. Hence, they require close observation.
Summary and Conclusion
The neutral zone philosophy is based on the concept that for each individual patient there exists within, the denture space, a specific area where the function of the musculature will not unseat the denture, and at the same time where the forces generated by the tongue are neutralized by the forces generated by the lips and cheeks. Furthermore, denture stability is as much or more influenced by tooth position and flange contour as to any other factor. Regardless of the method of treatment, any part of the dentition out of harmony with the neutral zone will result in instability, interference with function, or some degree of discomfort or will bother the patient. Thus the neutral zone must be evaluated as an important factor before one rates any changes in arch form or alignment of teeth.
Case Report – Determination Of Neutral Zone Using Tissue Conditioner
After recording the centric relation at desired vertical dimension, the lower occlusal rim has been reduced from both the buccal and lingual aspects ensuring the adequate space for the flow of tissue conditioner.
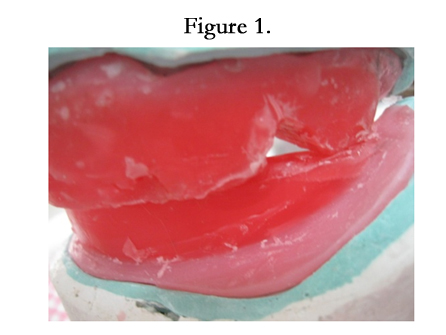
Figure 1
Patient is instructed to perform all the movements with special emphasis to the puckering movements ensuring the molding of tissue conditioner in the neutral zone. The material is allowed to set and the occlusal rims are taken out from the mouth.


Figure 2
The records are secured by beading and boxing of the mounted cast and then
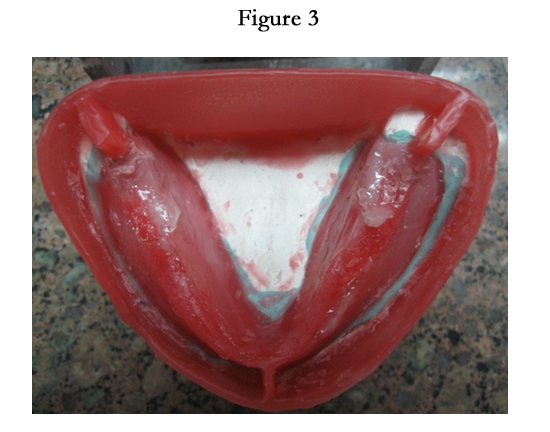

Figure 3
Plaster of Paris is poured on either side of the lower occlusal rims after applying separating media and markings are made to form the index.
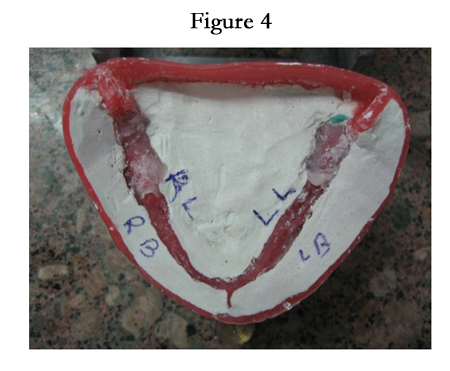

Figure 4
Teeth arrangement is done using these indices as guide on either side.


Figure 5
References
- Russel AF (1959) The reciprocal lower complete denture. J Prosthet Dent 9(2): 180-190.
- Roberts AF (1960) The effect of outline and form upon denture stability and retention. Dent Clin North Am 293-303.
- Heath R (1970) A study of the morphology of the denture space. Dent Pract 21: 109.
- Mathew MH, Wain AE (1961) The full denture problems. Br Dent J 61(5): 401-418.
- Fenn RB, Liddelow KP, Gimson AP (1986) Clinical Dental Prosthesis. CBC publishers and distributers.
- Beresin VE, Schiesser FJ (1976) The neutral zone in complete dentures. J Prosthet Dent 36(4): 356-367.
- Riggs PD, Parker S, Braden M, Kalachandra S (2002) Development of butyl elastomer/methacrylate monomer systems as denture soft lining materials. Biomaterials 23(3): 915-920.
- Brozek R, Koczorowski R, Rogalewicz R, Voelkel A, Czarnecka B, et al. (2011) Effect of denture cleansers on chemical and mechanical behavior of selected soft lining materials. Dent Mater 27(3): 281-290.





