Bioscaffold Augmentation of the Alveolar Bone: A Pilot Study in the Rabbit to Define the Protocol
King S1*, Klineberg I2, Deshpande S3, Brennan-Speranza TC4, Johansson C5, Voss K6
1 Lecturer, Faculty of Dentistry, The University of Sydney, Australia.
2 Professor, Faculty of Dentistry, The University of Sydney, Australia.
3 Department of Oral Restorative Sciences, Westmead Centre for Oral Health, The University of Sydney, Australia.
4 Department of Physiology and Bosch Institute for Medical Research, The University of Sydney, Australia.
5 Professor, Institute of Odontology, University of Gothenburg, The Sahlgrenska Academy, Sweden.
6 Associate Professor, Faculty of Veterinary Science University, The University of Sydney, Australia.
*Corresponding Author
Dr Shalinie King,
Lecturer, Faculty of Dentistry,
The University of Sydney, Level 6, Sydney Dental Hospital,
2 Chalmers Street, Surry Hills, NSW 2010,
Australia.
Tel: +61 0402 166 671
Fax: +61 2 9351 8333
E-mail: shalinie.king@sydney.edu.au
Article Type : Research Article
Received: July 27, 2015; Accepted: August 17, 2015; Published: September 04, 2015
Citation: King S, et al., (2015) Bioscaffold Augmentation of the Alveolar Bone: A Pilot Study in the Rabbit to Define the Protocol. Int J Dentistry Oral Sci. 2(9), 135-141. doi: dx.doi.org/10.19070/2377-8075-1500029
Copyright: King S© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: The current study aims to establish, for the first time, a model to determine the surgical and tissue processing protocols for testing the use of a synthetic bone graft material to augment the contour and volume of the reduced alveolar ridge.
Materials and Methods: Β-tricalcium phosphate grafts (Vitoss®), 6mm width x 3mm height x10mm length, were placed directly onto decorticated cortical bone on the lateral aspect of the left maxillary diastema of New Zealand white rabbits (n=6). The graft was secured to the underlying bone using an 8mm x 1.4mm titanium screw, covered with a resorbable collagen membrane and the surgical site closed. Tissue blocks were harvested at 3 weeks and 6 weeks. Two non-decalcified sections were scanned using micro tomographic imaging. Four sections were embedded in resin, stained with Pyronin-G and evaluated histologically. Graft vascularisation was examined on one decalcified frozen section labelled with anti-CD31 monoclonal antibody.
Results: All six sites healed well. The micro-CT analysis demonstrated maintenance of the graft height around the central screw. Histological evaluation and anit-CD31 labelling demonstrated woven bone formation and vascular and cellular infiltration within the grafted region. Quantitative analysis demonstrated increased new bone formation at the second time point (0.77 ± 0.42) compared with the first time point (0.48 ± 0.48).
Conclusion: The study concluded that the model was appropriate for testing the use of a synthetic bone graft material for augmentation of a reduced alveolar ridge. The qualitative and quantitative analyses demonstrated evidence of colonisation of the graft by bone forming cells.
2.Introduction
3.Materials and Method
3.1.Micro-CT scanning
3.2.Histology and Histomorphometry
3.3 Immunohistochemistry
4.Results
4.1.Clinical findings
4.2.Micro-CT scanning
4.3.Histology
4.3.Histomorphometry
4.4.Immunohistochemistry
5.Discussion
6.Acknowledgements
7.References
Keywords
Implants; Bone Regeneration; Grafting; Synthetic Grafts; Alveolar Augmentation.
Introduction
The success of endosseous dental implant placement for rehabilitating cases with severe horizontal and vertical ridge resorption depends on the presence of sufficient bone volume. Such cases are encountered in particular in the management of anadontia and hypodontia in Ectodermal Dysplasia (ED) or in long term elderly edentulous patients. Bone grafting to augment bone for oral implant placement has become a routine clinical practice and various grafting materials are available [1]. The material of choice for extensive bone regeneration remains autogenous bone [2]. However, this may be limited by factors such as significant donor site morbidity, unpredictable resorption rates and limited availability and quality of graft material [3].
Allografts (bone harvested from a donor and used on a different individual within the same species) are widely used, however their use is limited by both high and unpredictable resorption rates and increased immunological risks [4]. Xenografts (bone harvested from a donor of a different species) are also used, however poor osteogenic properties are common and increased immunogenic risks and risk of disease transmission is a concern [5]. Based on these limitations and risks there has been a need to develop alloplastic synthetic bone grafting materials.
Calcium phosphate based materials have been widely used in dentistry [6] and orthopaedics [7]. An ultra-porous beta – tricalcium phosphate (β-TCP) produced by Vitoss®-Stryker composed of a low density 90% porous material has been developed [8]. The material has features of both macro and microporosity with pores ranging in size from 1-1000μm in diameter with an average pore size of 100μm. A key feature that impacts on a material’s osteoconductivity is the level of porosity and the pore size. Optimal pore size for facilitation of bone in growth and vascularisation has been reported as being between 150-500 μm [9] and increased bony ingrowth in TCP grafts with pore sizes ranging from 50- 100μm compared to 200-400μm has been demonstrated [10]. The correlation between increased microporosity of a calcium phosphate material and the levels of gene expression related to osteogenic differentiation indicates greater osteoinductive capacity for materials with increased microporosity which has been demonstrated in a sheep model [11].
The Vitoss® material has been approved for clinical use as an autograft extender and has been used successfully to treat spinal fusion in orthopaedics [12]. There is, however, very limited evidence on the use of this material in the oral cavity for alveolar ridge augmentation. A case study reported positive bone regeneration using the Vitoss®-Stryker material soaked in human bone marrow aspirate (BMA) for sinus grafting [13]. For orthopaedic use, the material is generally combined with BMA which is a rich source of growth factors and osteogenic cells. The use of BMA in dental patients has not been used due to the prohibitive cost, and in this study venous blood was used as a substitute for BMA. Comparable expression of most growth factors in BMA and venous blood has been demonstrated [14]. One study in which TCP was used to heal a critical sized defect in the iliac wing in a sheep model demonstrated equal performance of TCP compared with autologous bone and improved performance compared with bone grafted with bone morphogenic protein-2 [11]. This data indicates that calcium phosphate materials may provide acceptable alternatives to autologous bone grafts for bone regeneration.
Improved bone height, and width for localised intra-oral defects can be achieved following treatment of the defects with the combination of a graft material and a barrier membrane [15]. Guided bone regeneration techniques using resorbable membranes are now widely used for regeneration of localised bone defects around dental implants. Reliable protocols to achieve generalised vertical ridge augmentation are yet to be defined [16].
The objectives of this pilot study were to establish a model for testing the use of a synthetic bone graft material to augment the contour of the reduced alveolar ridge. The natural diastema in the New Zealand white rabbit was chosen as the test site, as this site provides a clinical scenario that is similar to that which occurs in severely resorbed jaw bone. Similar to a reduced alveolar ridge the diastema site lacks bony walls, not only requiring the graft to be secured but and also limiting the ready access to bone osteogenic cells and growth mediators. Furthermore, soft tissue wound closure is similarly compromised. A calcium phosphate scaffold combined with venous blood, and protected by a barrier membrane, was placed directly onto decorticated cortical bone on the lateral aspect of the diastema.
The purpose of this investigation was to: 1) establish the surgical and tissue processing protocols for testing a material for bone regeneration of the reduced alveolar ridge, and 2) to establish a protocol for quantitatively and qualitatively analysing the regenerated tissues to assess bone tissue growth within the grafted region and the development of graft vascularisation.
Materials and Method
Six adult female New Zealand white rabbits of approximately the same age and weight were used in the study. The project was approved by the Sydney West Area Health Service Ethics Committee, 2012 (Protocol number 5095).
Each animal received a β-tricalcium phosphate graft (Vitoss®) with 90% porosity which was placed in the left maxillary diastema and prepared to the following dimensions: 10mm long, 6mm wide and 3mm thick (see Figures 1)
The operation was performed under sterile conditions. Anaesthesia was induced with i.v ketamine hydrochloride 100mg/ml (Ketamav 100, Mavlab) and medetomadine 1mg/ml (Domitor, Pfizer). Intubation was not possible for all rabbits; when intubation was not possible anaesthesia was maintained with additional doses of Ketamine. Otherwise, Isofluorane (Aerrane, Baxter) and oxygen were used to maintain aneasthesia. The aneasthesia was reversed with Atipamezole (Antisedan, Pfizer). An Antibiotic (Enrofloxacin) was given subcutaneously at the time of induction.
The surgical site was shaved and the surgical area cleaned with an antiseptic (Betadine®). The surgical procedure commenced with local anaesthesia (Lignocaine®) infiltrated in the buccal tissues. Then a 20mm incision 5mm distal to the papilla was made along the buccal aspect of the alveolar ridge. A mucoperiosteal flap was raised and the underlying bone exposed. A stainless steel round bur in an electric handpiece was used to decorticate the bone to encourage blood flow to saturate the graft material. The graft was then secured to the bone on the buccal aspect using an 8mm x 1.4mm titanium bone tenting screw (BioHorizons) (see Figure 1), and then covered with a 15mmx15mm collagen membrane (MemLok®). Soft tissue closure was achieved by releasing the flap and using 4-5 interrupted absorbable sutures (Vicryl®).
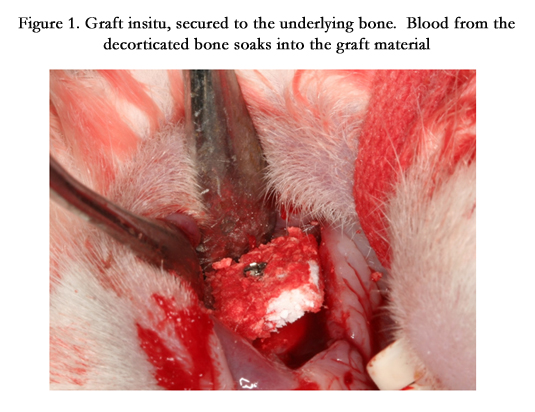
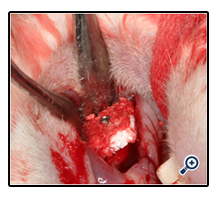
Figure 1. Graft insitu, secured to the underlying bone. Blood from the decorticated bone soaks into the graft material.
The rabbits were provided with an antibiotic (Enroflaxacin 1.2ml s.c) and a non-steroidal anti-inflammatory analgesic (Meloxicam (0.2ml s.c) for four days post operatively.
Three rabbits were euthanased at the 3 week time point and the remaining three at the six week time point. Euthanasia was achieved with Intravenous sodium pentobarbital and death was confirmed by cardiac arrest.
The maxilla was dissected out and sectioned immediately anterior to the molar teeth. The specimens were then immersed in 4% paraformaldehyde for 4 days after which they were transferred to 70% Ethanol
Prior to sectioning the fixed non-decalcified specimens were scanned with a micro-tomographic imaging unit using a cone beam geometry (ZEISS Xradia). Each sample was immersed in 70% ethanol in an airtight cylinder during the scanning process.
For each sample, micro-tomographic slices with an increment of 25 μm were acquired to cover the total length of the samples and 1600 projections were made. Each projection took approximately 2secs with a total scan time of 12 hours. The region, selected on the scout view, represented the graft bone centred around the titanium screw. Measurements were stored in 3D image arrays of high resolution (1024×1024 voxels).
Following micro-CT scanning, the non-decalcified specimens were sectioned on either side of the titanium screw to produce a central tissue block containing the screw and most of the graft material. Four specimens, two from each time point were dehydrated in graded acetone baths (Sigma-Aldrich) and embedded in methyl-methacrylate resin (Sigma-Aldrich) over a period of one month.
One section from each of the non-decalcified resin embedded specimens was made using the Exakt sawing and grinding technique [17] resulting in a thickness of about 15μm. The sections were histologically stained with Toluidine blue mixed in Pyronine G. Finally each section was mounted with a cover-glass prior to qualitative and quantitative (light microscopic) examinations.
Under a microscope, histomorphometric parameters were measured with a digitizing morphometry system coupled to a computer and the morphometry program,Osteomeasure (© 2005 Osteometrics). The region of bone analysed in all samples was in the central graft area, consisting of a 2.0mmx1.5mm grid made up of 4 x 3 500 μm2. The grid was placed over the grafted region and the digitised images were quantified to evaluate the following features: total bone volume/total area, total bone and graft surface/ total area and eroded surface of the graft/total bone surface. All measurements and calculations were referenced to the standard nomenclature [18].
One specimen which consisted of a tissue block sectioned on either side of the central screw from each time point was decalcified in 0.4M Ethylenediaminetetraacetic acid (EDTA) + 1.25% formalin for 1 week before being transferred to a 0.34M EDTA solution for a further two weeks to ensure adequate decalcification. Following this the specimens were placed overnight in a 30% sucrose and phosphate buffered saline (PBS) solution prior to being embedded in optimal cutting temperature medium (OCT), snap frozen in isopentane and then sectioned using the Leica CM 1950 cryostat. These sections were then glued onto glass slides using Chitosan in preparation for immunohistochemistry (IHC).
The slides were then rehydrated in PBS and the cells permeabilised. Unspecific binding was blocked using a 10% Goat serum in PBS. The sections were then incubated overnight at 4°C in a 1:20 dilution of anti -CD31 JC/70A monoclonal antibody, DAKO. Following this the endogenous peroxides were quenched in 3% Hydrogen peroxide at room temperature and the secondary antibody (biotinylated goat-anti-mouse, DAKO) diluted 1:250 in dilution buffer was used. Finally the sections were incubated with Streptavidin-peroxidase (SIGMA #S5512) followed by DAB (DAB substrate kit SK-4100, Vector Laboratories Inc.) and counter stained with Haematoxylin and Eosin. The Ultramount No. 4 (Fronine) mounting media was used and finally the sections were coverslipped prior to light microscopic examination.
Results
The overall postoperative assessment of the rabbits was excellent. All six rabbits were behaviourally healthy and demonstrated normal weight gain. Biologically, the wound healing was very good with only one site showing slight wound dehiscence but no infection.
In this study the micro-CT differentiation of new bone within the grafted region was not sufficiently clear for definitive measurement and quantification. The bone tissue and the graft material had very similar densities, therefore accurate differentiation between the two using grey scale thresholding was not felt to be reliable. The analysis did however demonstrate maintenance of the graft height around the central screw vertically (See Figure 2).
Figure 2. Section from R3, native bone with grafted region laterally. The head of the titanium screw is visible at the bottom of the image. Differentiation between bone tissue and graft material particularly within the grafted region was not clear.
At both the 3 and 6 week time points, the grafted area buccal to the cortical bone was clearly identifiable. The collagen membrane was intact and protecting the site (See Figures 3a and 3b). Histological evaluation demonstrated similar qualitative tissue reactions irrespective of time point. In general macrophages, both darkand light stained and of various sizes and shapes were the most common cells present. Histological evaluation demonstrated darker stained areas of woven bone with large immature osteocytes incorporated (Figure 3c).
Moreover, some graft regions demonstrated smaller areas likely to be calcium precipitate (Figure 3d). Irrespective of time point, loose grafting particles seemed to be internalized and phagocytized by cells. Multinuclear foreign body giant cells were observed as surrounding cell-clusters around the grafting material (Figure 3c and Figure 3d).
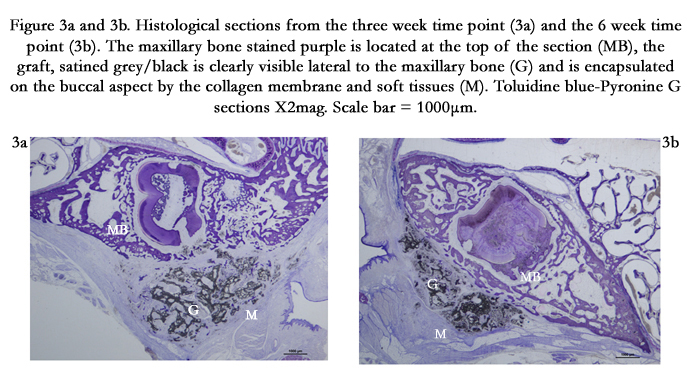
Figure 3a and 3b. Histological sections from the three week time point (3a) and the 6 week time point (3b). The maxillary bone stained purple is located at the top of the section (MB), the graft, satined grey/black is clearly visible lateral to the maxillary bone (G) and is encapsulated on the buccal aspect by the collagen membrane and soft tissues (M). Toluidine blue-Pyronine G sections X2mag. Scale bar = 1000μm.
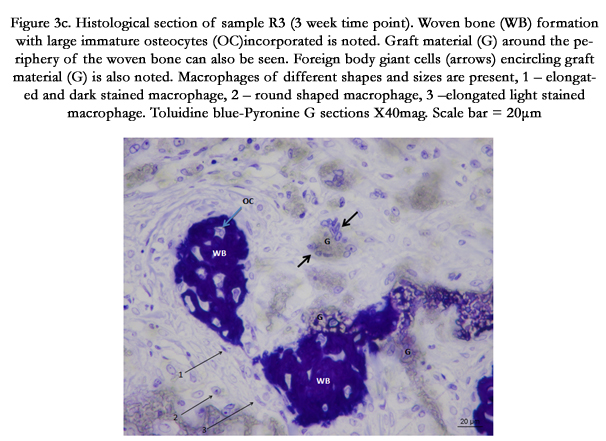
Figure 3c. Histological section of sample R3 (3 week time point). Woven bone (WB) formation with large immature osteocytes (OC)incorporated is noted. Graft material (G) around the periphery of the woven bone can also be seen. Foreign body giant cells (arrows) encircling graft material (G) is also noted. Macrophages of different shapes and sizes are present, 1 – elongated and dark stained macrophage, 2 – round shaped macrophage, 3 –elongated liglight stained macrophage. Toluidine blue-Pyronine G sections X40mag. Scale bar = 20μm
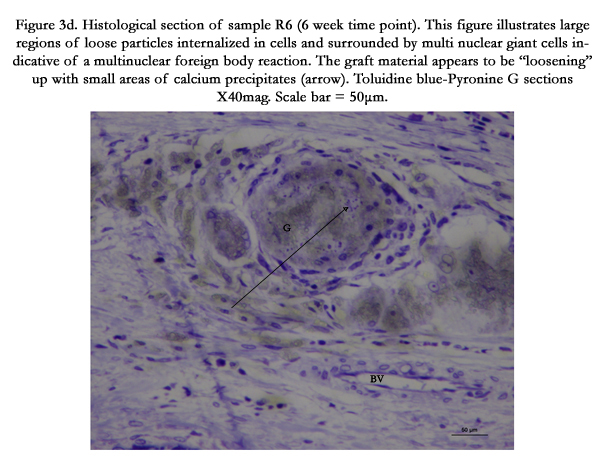
Figure 3d. Histological section of sample R6 (6 week time point). This figure illustrates large regions of loose particles internalized in cells and surrounded by multi nuclear giant cells indicative of a multinuclear foreign body reaction. The graft material appears to be “loosening” up with small areas of calcium precipitates (arrow). Toluidine blue-Pyronine G sections X40mag. Scale bar = 50μm.
Quantitative analysis of a single region of interest 2 x 1.5 mm within the grafted region of each sample demonstrated an increased new bone formation at the second time point (0.79 ± 0.42) compared with the first time point (0.48 ± 0.49), see Table 1. Replacement of the graft by new bone was supported by two findings. First, that the graft surface area (as measured by the eroded surface of the graft) reduced at the 6-week time point compared with the 3-week time point (2799.88 ± 2857.68 Vs 677.90 ± 112.92) and second that the overall volume of the solid material (as measured by the total graft and bone surface) remained stable over the two time points.
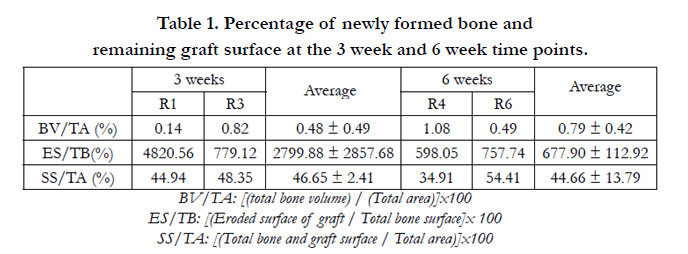

Table 1. Percentage of newly formed bone and remaining graft surface at the 3 week and 6 week time points.
The anit-CD31 labelling demonstrated vascular infiltration of the grafted region thus providing evidence of angiogenesis within the graft (See Figure 4). Only one sample from the second time point was available for light microscopic observations. Unfortunately due to the angled position of the central titanium screw in the specimen from the first time point it was not possible to obtain satisfactory sections from this specimen.
An internal control was used, endothelial staining of identifiable blood vessels in the non-grafted region of the bone was used as a control.
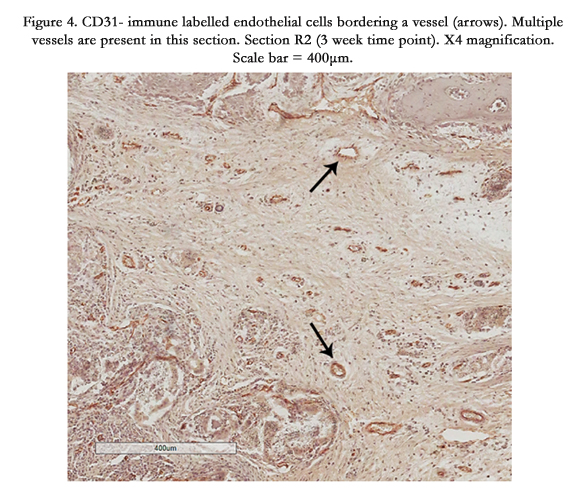
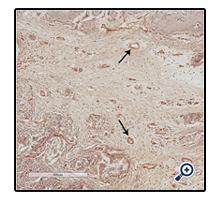
Figure 4. CD31- immune labelled endothelial cells bordering a vessel (arrows). Multiple vessels are present in this section. Section R2 (3 week time point). X4 magnification. Scale bar = 400μm.
Discussion
The synthetic graft material used in this study is already widely used in orthopaedic practice; however, it has not previously been trialled intra-orally. This study aimed to develop a surgical and tissue processing protocol to test this material and its use in an intraoral site that would simulate the clinical conditions associated with regenerating bone on a reduced alveolar ridge.
One concern was whether the graft would be retained in situ and whether soft tissue closure could be maintained. This study has demonstrated excellent postoperative healing of the grafted sites. The rabbits were able to masticate a normal diet (pellets and fresh fruit or vegetables), and the grafts were maintained for the duration of the six week study period. Importantly, this study also demonstrated that there were no adverse effects with the placement of Vitoss® in an intra–oral site for bone regeneration. As this study was a pilot to test the surgical and tissue processing protocols a specific control site was not included. Future studies would need to include a control site where a flap was raised without the placement of a graft material to provide additional valuable information.
A titanium tenting screw was used to maintain the graft and this did create some technical problems in sectioning the tissue blocks as the microtome that was available was not able to section through the titanium screw. This meant that the tissue blocks had to be sectioned coronally on either side of the central screw. Sectioning sagitally through the centre of the graft would have enabled the division of the tissue block into two halves enabling more representative sections of the graft and importantly the ability to use one half for histomorphometry and the other half for IHC analysis. The central screw did however simulate the positioning of a dental implant and future studies could optimise this protocol using a dental implant in this position and sectioning through the implant.
Bone regeneration using TCP as a graft material has been studied in a number of different animal models, however many of these have been performed on intra-osseous defects in long bones [10, 11, 19-21] and results have varied.
Eggli et al [10] placed TCP in cylindrical defects in femoral and tibial defects of the rabbit. They used a TCP with 60% porosity and 5-10% microporosity. In their study upto 85% of the TCP graft material was resorbed at the 6 month end point with the smaller pored TCP (50-100μm pores) showing more rapid tissue ingrowth and graft resorption. Similar findings were made by Buser et al (1998) who used a TCP with 60% porosity in the mini pig model-at the 4 week time point the study demonstrated an inconsistent pattern of bone formation with ceramic particles embedded in fibrous tissue. At the 24 week time point however they were able to demonstrate obvious bone remodelling and complete graft resorption. Likewise, Walsh et al [21], using a rabbit tibial defect packed with Vitoss demonstrated complete graft resorption at 12 weeks with new bone formation within the grafted site. A more recent study [11] has shown promising results in the use of TCP to heal critical sized defects in the iliac crest of the sheep model. The TCP grafted defects showed comparable results to those grafted with autogenous bone. The defects tended to show more peripheral bone deposition compared to the central region with some fibrous tissue noted centrally.
On the other hand in a study [20] using a cylindrical defect in the femoral articular condyle of the rabbit grafted with TCP (80% porosity) early bone regeneration up to week 6 followed by resorption of previously laid down bone at the 12 week time point was reported. This study noted colonization of the defect by large numbers of phagocytic cells which led to this resorption and reduction in new bone volumes between week 6 and week 12. Superficial and central areas of avascular fibrous tissue were noted with the continued deposition of woven bone rather than lamellar bone. The authors did note that the relatively high metabolic rate of the rabbit is likely to influence the graft resorption rate.
However, the intraosseous defect in the long bone does not reflect accurately the clinical situation of regenerating bone in the reduced alveolar ridge. The performance of the material may be different when placed in the maxilla or mandible as evidence suggests that graft location may also affect the behaviour of a given graft material [22].
Intra-orally, a study aiming to augment bone on the lateral aspect of the mandible in the rabbit model [23] used two different types of TCP blocks to augment bone - one material with a porosity of 70% included micropores of 0.5μm and another more dense material with 46% porosity, micropores of 0.2μm and rod shaped structures. Unlike the current study they used an extra oral approach to place the graft. The results for the 70% porous material were disappointing, and although initial bone formation was noted at the 6 week time point there was also considerable fibrous tissue infiltration. At the 24 week time point, there was a collapse in the graft outline with a significant area of the grafted region being occupied by adipose tissue encapsulating residual graft and only a small area of new bone at the base of the graft. Interestingly although the less porous denser TCP material showed less bone infiltration at the 6 week time point at 24 weeks the denser material demonstrated increased bone volume compared to the less dense material. Furthermore the graft maintained its original shape and was proposed as a more suitable material for an onlay graft. The study highlights the importance of a material’s architecture on its ability to alter the rate of resorption and further stresses the importance of a longer (24 week) observation period.
Our study also noted some collapse of the graft area – the height of the graft around the central screw was maintained however towards the periphery the graft reduced in height. This supports the need to alter bone contour and volume supported by an implant or screw.
A study [24] conducted on a canine model aimed for lateral ridge augmentation by creating two-wall defects in the mandibular alveolar ridges bilaterally. One of the materials tested in this study was β-TCP with a porosity of 70%. This was a pilot study performed on 3 animals using three test sites. One site demonstrated excellent bone formation, however two had inconsistent findings of new bone infiltration.
In our study, the quantitative analysis of bone tissue within the grafted region demonstrated promising results. The percentage of new bone within the grafted region was higher at the second time point compared to the first time point 0.48 ± 0.49 compared to 0.79±0.42 and indicates bone tissue formation within the graft over time (See Table 1). The question as to whether the graft is being replaced by bone is confirmed by two findings, first, that the graft surface (as measured by the eroded surface of the graft) is reduced at the second time point 2799.88 ± 2857.68 compared to 677.90 ± 112.92, and second that the overall volume of the solid material within the grafted region as measured by the bone and graft surface, changed very little over time (See Table 1). The residual graft in one animal R1 from the first time point was considerably higher than in all the other cases 4820.56 compared to 779.19 in R3, 598.05 in R4 and 757.74 in R6, suggesting minimal replacement of the graft over time (See Table 1). Interestingly this was the only animal in which some wound dehiscence was noted and highlights the importance of meticulous wound closure in the success of bone tissue regeneration.
Micro-CT images are known to provide useful information on contour and volume of grafted areas. Previous studies [25-27] have shown micro CT images with computer assisted image analysis to be comparable to histomorphometry for measuring bone tissue regeneration. In this study however we were unable to reliably differentiate the new bone within the grafted region from the graft material. Further analyses for determining an accurate threshold selection will be investigated as it has been shown to be important for reliable measurement of a given volume fraction [28].
For successful bone tissue regeneration the synthetic graft needs to be vascularised. Although the graft may initially rely on the surrounding vasculature for the diffusion of nutrients and removal of waste products, long term success requires that the graft develop a vascular bed. The newly developed blood vessels will enable colonisation of the graft by osteogenic cells and eventually replacement of the graft with bone tissue. CD-31 antibody is an established marker of endothelial cells as it binds to a cell adhesion molecule expressed strongly by endothelial cells. A recent study has demonstrated that angiogenesis precedes osteogenesis [29]. Although only one section from the second time point could be used in the immunohistochemical part of the study, it demonstrated positive labelling of endothelial cells. Therefore we were able to demonstrate a successful protocol for staining endothelial cells in this model and to demonstrate angiogenesis within the grafted region. Similar angiogenic invasion into Beta-TCP has been previously reported [30]. The sample size was however insufficient to enable quantitative analysis.
TCP has been used in a number of animal models and in varying formulations; the studies indicate that for a given location the synthetic material may need to be tailor made to suit the application in terms of its physical architecture, including porosity, microporosity, grain size etc. This study has developed an animal model to test these materials for the specific clinical application of regenerating bone in the reduced alveolar ridge. Although preliminary histological and hisomorphometric analyses have been completed afurther study with more samples in each time point and over a longer observation period would allow quantitative analysis with statistical comparisons.
Acknowledgement
We acknowledge the following persons:
Dr Petra Hammarström Johansson (Research Technician, Institute of Odontology, University of Gothenburg), Dr Heide Kloeppel (Anaesthetist, Sydney Veterinary School, The University of Sydney), Dr Terry Whittle (Research Assistant, Faculty of Dentistry, The University of Sydney), Professor David Little (Director, Orthopaedic research unit, Westmead), Ms Alyson Morse (Research Assistant, Orthopaedic research unit, Westmead), Dr Mille Kolind (Research Assistant, Orthopaedic research unit, Westmead), Dr Ross Matthews (Director animal care centre, Westmead Hospital), Mr Andrew Holmes (General Manager, Biohorizons), Dr Tim Barker (Director of Clinical Research, Stryker South Pacific), Dr Tim Barker (Director of Clinical Research, Stryker South Pacific), Ms Jenny Down (Osteoporosis and Bone Programme, The Garvan Institute of Medical Research, Sydney).
References
- Esposito M, Grusovin MG, Coulthard P, Worthington HV (2006) The efficacy of various bone augmentation procedures for dental implants: a Cochrane systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants 21(5): 696-710.
- Pape HC, Evans A, Kobbe P (2010) Autologous Bone Graft: Properties and Techniques. J Orthop Trauma 24(Suppl 1): S36-S40.
- Goldberg VM, Stevenson S, Shaffer JW (1991) Biology of autografts and allografts. In: Bone and Cartilage allografts: Biology and Clinical applications. Am Acad Orthopaedic Surg 3-11.
- Lyford RH, Mills MP, Knapp CI, Scheyer ED, Mellonig JT (2003) Clinical evaluation of freeze dried block allografts for alveolar ridge augmentation: a case series. Int J of Periodontics Restorative Dent 23(5): 417-425.
- Mordenfeld A, Hallman M, Johansson CB, Albrektsson T (2010) Histological and histomorphometrical analyses of biopsies harvested 11 years after maxillary sinus floor augmentation with deproteinized bovine and autogenous bone. Clin Oral Implants Res 21(9): 961-970.
- LeGeros RZ (2008) Calcium phosphate-based osteoinductive materials. Chem Rev 108(11): 4742-4753.
- Cameron HU (1992) Tricalcium phosphate as a bone graft substitute. Contemp Orthop 25(5): 506-508.
- Erbe EM (2000) Attributes of Vitoss synthetic cancellous bone void filler, an ultraporous betatricalcium phosphate scaffold [abstract]. International Workshop on Bone Substitutes (AO Foundation - Association for the Study of Internal Fixation). Davos, Switzerland.
- Daculsi G, LeGeros RZ, Heughebaert M, Barbieux I (1990) Formation of carbonate-apatite crystals after implantation of calcium phosphate ceramics. Calcif Tissue Int 46(1): 20-27.
- Eggli PS, Muller W, Schenk RK (1988) Porous Hydroxyapatite and Tricalcium Phosphate Cylinders with Two Different Pore Size Ranges Implanted in the Cancellous Bone of Rabbits: A Comparative Histomorphometric and Histologic Study of Bony Ingrowth and Implant Substitution. Clin Orthop Relat Res (232): 127-138.
- Yuan H, Fernandes H, Habibovic P, de Boer J, Barradas AM, et al. (2010) Osteoinductive ceramics as a synthetic alternative to autologous bone grafting. Proc Natl Acad Sci USA 107(31): 13614 - 13619.
- Epstein NE (2006) A Preliminary Study of the Efficacy of Beta Tricalcium Phosphate as a Bone Expander for Instrumented Posterolateral Lumbar Fusions. J Spinal Disord Tech 19(6): 424-429.
- Smiler DG, Soltan M, Lee JW (2007) A Histomorphogenic Analysis of Bone Grafts Augmented With Adult Stem Cells. Implant Dent 16(1): 42-53.
- Smiler DG, Soltan M, Soltan C, Matthews C (2010) Growth Factors and Gene Expression of Stem Cells: Bone Marrow Compared With Peripheral Blood. Implant Dent 19(3): 229-240.
- Lundgren AK, Sennerby L, Lundgren D (1997) An experimental rabbit model for jaw-bone healing. Int J Oral Maxillofac Surg 26(6): 461-464.
- Rocchietta I, Fontana F, Simion M (2008) Clinical outcomes of vertical bone augmentation to enable dental implant placement: a systematic review. J Clin Periodontol 35(8 Suppl): 203-215.
- Donath K, Breuner G (1982) A method for the study of undecalcified bones and teeth with attached soft tissues. The Säge-Schliff (sawing and grinding) technique. J Oral Pathol 11(4): 318-326.
- Dempster DW, Compston JE, Drezner MK, Glorieux FH, Kanis JA, et al. (2013) Standardized nomenclature, symbols, and units for bone histomorphometry: A 2012 update of the report of the ASBMR Histomorphometry Nomenclature Committee. J Bone Miner Res 28(1): 2-17.
- Buser D, Hoffmann B, Bernard JP, Lussi A, Mettler D, et al. (1998) Evaluation of filling materials in membrane -protected bone defects. A comparative histomorphometric study in the mandible of miniature pigs. Clin Oral Implants Res 9(3): 137-150.
- Hing KA, Wilson LF, Buckland T (2007) Comparative Performance of three bone graft substitutes. Spine J 7(4): 475-490.
- Walsh WR, Vizesi F, Michael D, Auld J, Langdown A, et al. (2008) Beta- TCP bone graft substitutes in a bilateral rabbit tibial defect model. Biomaterials 29(3): 266-271.
- Constantz BR, Barr BM, Ison IC, Fulmer MT, Baker J, et al. (1998) Histological, chemical, and crystallographic analysis of four calcium phosphate cements in different rabbit osseous sites. J Biomed Mater Res 43(4): 451-461.
- Ono D, Jimbo R, Kawachi G, Ioku K, Ikeda T, et al. (2011) Lateral bone augmentation with newly developed β-tricalcium phosphate block: an experimental study in the rabbit mandible. Clin Oral Implants Res 22(12):1366-1371.
- von Arx T, Cochran DL, Hermann JS, Schenk RK, Buser D (2001) Lateral ridge augmentation using different bone fillers and barrier membrane application. A histologic and histomorphometric pilot study in the canine mandible. Clin Oral Implants Res 12(3): 260-269.
- Lu M, Rabie AB (2004) Quantitative assessment of early healing of intramembranous and endochondral autogenous bone grafts using micro-computed tomography and Q-win image analyzer. Int J Oral Maxillofac Surg 33(4): 369-376.
- Vinci R, Rebaudi A, Cappare P, Gherlone E (2011) Microcomputed and histologic evaluation of calvarial bone grafts: A pilot study in humans. Int J of Periodontics Restorative Dent 31(4): e29-e36.
- Dayer R, Brennan TC, Rizzoli R, Ammann P (2010) PTH improves titanium implant fixation more than pamidronate or renutrition in osteopenic rats chronically fed a low protein diet. Osteoporos Int 21(6): 957-967.
- Hara T, Tanck E, Homminga J, Huiskes R (2002) The influence of microcomputed tomography threshold variations on the assessment of structural and mechanical trabecular bone properties. Bone 31(1): 107-109.
- Moreira DC, Sá CN, Andrade MG, de Bittencourt TCB, de Almeida Reis SR, et al. (2013) Angiogenesis and Osteogenesis at Incorporation Process of Onlay Bone Graft. J Oral Maxillofac Surg 71(12): 2048-2057.
- Henno S, Lambotte JC, Glez D, Guigand M, Lancien G, et al. (2003) Characterisation and quantification of angiogenesis in β-tricalcium phosphate implants by immunohistochemistry and transmission electron microscopy. Biomaterials 24(19): 3173-3181.





