Dermatoglyphics: The Ever Lasting Impressions
Cheena S1*, Parvathi M2
1 Senior Lecturer, Oral Medicine and Radiology Department, Post Graduate Institute of Dental Sciences (MDU), Rohtak, India.
2 Professor and Head of Department, Teerthanker Mahaveer Dental College and Research Centre, Moradabad, Uttarpardesh, India.
*Corresponding Author
Dr. Cheena Singh,
Senior Lecturer, Oral Medicine and Radiology Department,
Post Graduate Institute of Dental Sciences (MDU),
Rohtak, India.
E-mail: Cheenasngh3@gmail.com
Article Type: Review Article
Received: May 17, 2015; Accepted: June 19, 2015; Published: July 07, 2015
Citation:Cheena S, Parvathi M (2015) Dermatoglyphics: The Ever Lasting Impressions. Int J Dentistry Oral Sci. 2(7), 111-114. doi: dx.doi.org/10.19070/2377-8075-1500024
Copyright: Cheena S© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The study of human hand has always been fascinating, not only to anthropologists and physicians, but also to psychologists,
writers, painters and chiromancers. As from cradle to grave until the body decomposes finger prints remain unchanged.
The study of palmar prints and finger prints is known as dermatoglyphics which is now days itself used as an extremely
useful tool for preliminary investigations for premalignant lesions, dental caries, systemic diseases, genetic diseases and
syndromes. This review focuses on the applications of dermatoglyphics in different fields of medical and dental sciences
2.Introduction
3.History
3.1.Embryogenesis of Dermatoglyphic Patterns
3.2.Anatomical Configurations
3.3.Other dermatoglyphic landmarks
3.4.Palmar pattern configuration
3.5.Quantitative Analysis
3.6.Applied aspects in head and neck region
4.Conclusion
5.References
Keywords
Dermatoglyphics; Precancerous Lesion and Conditions of Oral Cavity.
Introduction
Dermatoglyphics is a branch of science, which deals with the study of ridge patterns on finger tips, palms, soles and toes. The skin on the palmar and plantar surfaces of man is not smooth. It is grooved by curious ridges, which form a variety of configurations [1]. Dermatoglyphic (Derma = Skin + Glyphe = Carve) is a collective name for all those integumentary features within the limits to be defined, and it applies also to the division of Anatomy which includes their study. Study of the patterns of the epidermal ridges of fingers, palm and sole can serve as an aid to the diagnosis of many diseases, particularly those caused by chromosomal aberration, which are frequently accompanied by distortion of patterns, and non-genetically determined diseases as well. Diagnosis of Diabetes Mellitus, Schizophrenia, hypertension, etc., can now be aided by dermatoglyphic analysis [2].
It is also a useful diagnostic tool in diagnosis of premalignant lesions and conditions of oral cavity, dental caries, periodontitis, carcinoma of head and neck region, cleft lip and cleft palate, malocclusion.
History
The earliest description of epidermal ridges was published at the end of the 17th century, but the study of finger patterns and their use for personal identification was begun by Francis Galton in 1892. The scientific study of papillary ridges of the hands and feet is credited as the beginning with the work of Joannes Evangelista Purkinje in 1823. William Herschel (1858) was the first to experiment with fingerprints in India. The most extensive description and classification of dermal patterns were made by Harold Cummins in 1926; he called them “dermatoglyphics”[3].
In Germany, Dr. Alexander Rodewald in 2001 diagnosed many congenital abnormalities with 90% accuracy from the features of the hands alone. Dr. Stowens in 2003, Chief of Pathology at St Luke's Hospital in New York, claims to diagnose schizophrenia and Leukemia with 90% accuracy from the patterns on the hands alone [4].
The ridge configurations on the volar surfaces of hand are formed by elevated parallel rows of sweat – gland orifices each about half a millimeter wide. They develop by the third month of fetal life and are under strong but not exclusive genetic control. Environmental fetal influences are evident if we consider the differences which exist between the left and right hands of identical twins. Environmental modifications also can be induced by teratogenic substances [3].
Bonnevie (1929) speculated that fingerprint patterns were dependent upon the underlying arrangement of peripheral nerves.
Cummins (1935), observed the ridge configurations of congenitally malformed hands and proposed, that direction of epidermal ridges was determined by growth forces and contour of volar skin at the time of ridge formation.
Humphrey (1964) studied the early function of the fetal hand and indicated that digital and palmar creases are secondary features, which are related to flexion movements in the developing hand between the seventh and fourteenth weeks of development.
William. J. Babler (1976) indicated that the epidermal ridges first appear in the form of localized cell proliferations around the 10th to 11th week of gestation. These proliferations form shallow corrugations that project into the superficial layer of the dermis. The number of ridges continue to increase, being formed either between or adjacent to existing ridges. It is during this period of primary ridge formation, that the characteristic patterns are formed. At about 14 weeks, the primary ridge formation ceases and secondary ridges begin to form as sweat gland, and develop along the apices of the primary ridges at uniform intervals. At this time, the epidermal ridges first begin to appear on the volar surfaces. The dermal papillae are reported to develop in the valleys between the ridges on the deep surface of the epidermis around the 24th week. Till then, the morphology of primary and secondary ridges appear as a smooth ridge of tissue and thereafter peg like structures, the dermal Papillae, characteristic of the definitive dermal ridges, are progressively formed [4].
Finger tip pattern: Galton (1892) divided the ridge patterns on the distal phalanges of the fingertips into three main groups namely: Arches, Loops and Whorls (Figure 1).
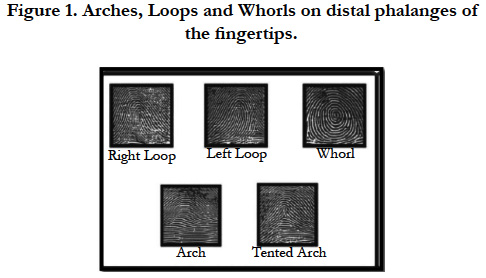
Figure 1. Arches, Loops and Whorls on distal phalanges of the fingertips.
It is the simplest pattern found on fingertips. It is formed by succession of more or less parallel ridges, which traverse the pattern area and form a curve that is concave proximally. The arch pattern is subdivided into two types:
a. Simple arch or plain arch (PA), composed of ridges, that cross the fingertip from one side to the other without recurving. (Figure 1)
b. Tented arch (TA) composed of ridges that meet at a point so that their smooth sweep is interrupted. The point of confluence is called a tri-radius, because ridges usually radiate from this point in three different directions. In the tented arch, the triradius is located near the midline axis of the distal phalanx. The distal radiant of the triradius usually points vertically toward the apex of the fingertip. Ridges passing over this radiant are abruptly elevated and form a tent like pattern and are designated as 'tented arch (Figure 2).
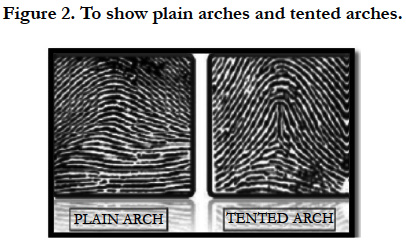
Figure 2. To show plain arches and tented arches.
It is the most common pattern on the fingertip. A series of ridges enter the pattern area on one side of the digit, recurve abruptly, and leave the pattern area on the same side.
• If the ridge opens on the ulnar side, resulting loop is termed as ulnar loop.
• If the ridge opens toward the radial margin it is called a radial loop. A loop has a single triradius or confluence point of ridges. The triradius is usually located laterally on the fingertip and always on the side where the loop is closed. Loops may vary considerably in shape and size. They may be large or small, tailor short, vertically or horizontally oriented, Plain Loop (PL) or Double Loop (DL) (Figure 3). Occasionally, 'Transitional' loops can be found which resemble whorls or complex patterns.
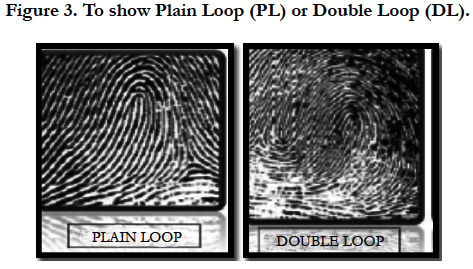

Figure 3. To show Plain Loop (PL) or Double Loop (DL).
It is any ridge configuration with two or more triradii. One triradius is on radial and the other on the ulnar side of the pattern. Henry (1937) limited the designation of the term 'Whorl' to those configurations having ridges that actually encircle a core. He named more complex patterns as "Composites”. The ridges in a Plain (Simple)/whorl (PW) are commonly arranged as a succession of concentric rings or ellipses. Such patterns are described as concentric whorls (Wc). Another configuration spirals around the core in either a clockwise or a counterclockwise direction. This pattern is called a Double (DW) or a spiral whorl (WS). (Figure 4)
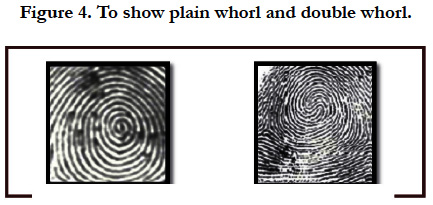
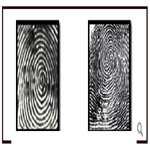
Figure 4. To show plain whorl and double whorl.
According to Manoj Kumar Sharma and Hemlata Sharma The classification of dermatoglyphics has done as below:
• Digital pattern of ridges (Digital Dermatoglyphics).
• Palmar pattern of the ridges (Palmar Dermatoglyphics).
There are three basic dermatoglyphics land marks found on fingertip pattern that are:
• Triradii,
• Cores and
• Radiant.
It is formed by the confluence of three ridge systems. The geometric center of the triradius is designated as a triradial point. It is the meeting point of three ridges that form angles of approximately 120° with one another. The triradial point forms one terminus of the line along which ridges are counted. Sometimes, large patterns are extralimital in nature. These are commonly observed in the hypothenar areas of the palms and the hallucal areas of soles. (Figure 5)
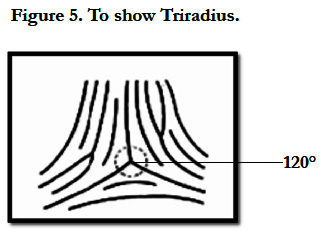
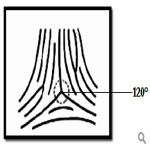
Figure 5. To show Triradius.
It is in the approximate center of the pattern. The core may be of different shapes. In a loop pattern, the core is usually represented by a straight, rod like ridge or a series of two or more such parallel ridges, over which other recurving ridges pass. If a straight ridge is absent in the center of the loop, the innermost recurving ridge is designated as a core. In a whorl, the core can appear as a dot or a short ridge (either straight or bent) or it can be shaped as a circle or an ellipse in the center of the pattern.
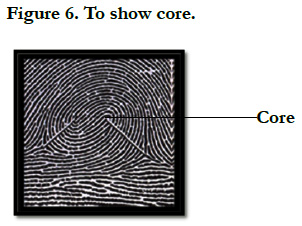
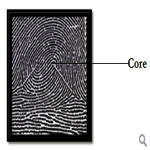
Figure 6. To show core.
These are the ridges that emanate from the triradius and enclose the pattern area. These ridges constitute the 'skeletal' framework of the pattern area.
In order to carry out dermatoglyphic analysis that can be compared in different individuals, the palm has been divided into several anatomically designed areas which includes Thenar areas, First, Second, third and fourth interdigital areas and Hypothenar area.
It is used to indicate the pattern size. The counting is done along a straight line connecting the triradial point to the point of core. The ridges containing the point of core and triradial point are both excluded from the count. Ridges are often counted between two digital triradii. The ridge count most frequently obtained is between triradii a and b, and is referred to as the a-b ridge count. (Figure 7)
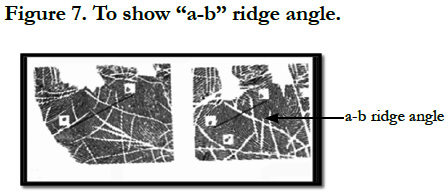

Figure 7. To show “a-b” ridge angle
This angle is formed by lines drawn from the digital triradius (a) to the axial triradius (t) and from this triradius to the digital triradius (d). Sometimes accessory ‘a’ or ‘d’ triradii are present on the palm. (Figure 8)
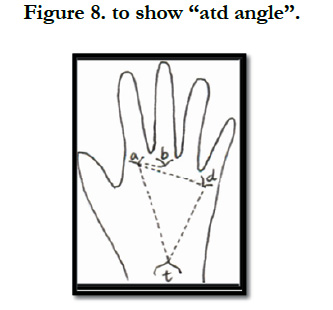

Figure 8. to show “atd angle”.
Tamgire DW et al (2013) conducted a study to evaluate the dermatoglyphics in Oral sub mucous fibrosis patient. This study was conducted on 100 clinically diagnosed OSMF gutkha chewers patients and 100 non - gutkha chewers patients. In these patients, total finger ride count (TFRC) and atd angle was measured and statistically analyzed. There was significant decrease in mean TFRC and ‘atd’ angle for the patients of Oral sub Mucous Fibrosis [2]. Thus, dermatoglyphics help in diagnosis of premalignant lesions like OSMF and leukoplakia.
A Sharma, R Somani (2009) conducted a study on dermatoglyphic interpretation of dental caries of dental caries and its correlation to salivary bacteria interactions on 90 patients and found highly significant difference in loops between the subject (Caries) and control groups, and also observed significant difference between subject and control groups for microbial growth. Similar study was also conducted by Padma K Bhat et al (2011) to detect dental caries among 100 school children aged 6-16 years who were deaf and mute using dermatoglyphics. It was found that frequency of whorls was found to be more in caries group. So, dermatoglyphics can be used as diagnostic tool for diagnosing dental caries.
Mathew L., Hegde A. M., Rai K. (2005) conducted a study on 50 oral cleft children and 50 normal children were collected using the ink method and comparison was done between them. In the present study, we found an increase in the ulnar loop patterns on the distal phalanges of the ten fingers, an increase in the atd angle and an increase in the fluctuating asymmetry of the atd angle in the oral cleft children which indicates the degree of developmental instability of the oral cleft individual. Hence dermatoglyphics is used to determine the usefulness of dermatoglyphics in studying the genetic etiology of oral clefts.
The decrease in frequency of the twinned and transversal ulnar loops on all the fingers with juvenile periodontitis. in rapidly progressive periodontitis, decrease in the frequency of double loops on all fingers and increase in frequency of radial loops in right second digit.
A study was conducted by Elluru Venkatesh et al (2008) [11] to evaluate palmar dermatoglyphics in oral leukoplakia and oral squamous cell carcinoma. The study concluded that dermatoglyphic patterns may have a high role in identifying individuals either with or at risk for developing oral leukoplakia and oral squamous cell carcinoma, hence can be used for identifying high risk groups.
A study was conducted by I.C. Fuller (1973) about role of palmar dermatoglyphics as a medical diagnostic aid. Dermatoglyphics of patients suffering from diabetes, duodenal ulcer, asthma, and various cancers have been contrasted and significant differences in the digital ridge counts, maximum atd angles, and distal palmar loop ridge counts have been found. Attention is drawn to the possibility that prognostic implications of dermatoglyphics might be relevant aid to screening techniques.
S Tikare et al (2010) from their study observed that Dermatoglyphics might be an appropriate marker for malocclusion and further studies are required to elucidate an association between fingerprint patterns and malocclusion.
Conclusion
Fingerprints are constant and individualistic and form the most reliable criteria for identification. Fingerprint patterns are genotypically determined and remain unchanged from birth till death. Positive identification using fingerprints can be established only if 16 to 20 points of similarity exist in the minutiae. As the dermatoglyphics are genetically controlled characteristics, any deviation in dermatoglyphic features indicates a genetic difference between the control and study group population. Dermatoglyphics has moved from obscurity to acceptability as a diagnostic tool.
References
- Soni A, Singh SK, Gupta A (2013) Implications of dermatoglyphics in dentistry. Journal Of Dentofacial Sciences 2(2):27-30.
- Tamgire DW, Fulzele RR, Chimarka VK, Rawlani SS, Sherke AR (2013) Qualitative dermatoglyphic analysis in patients of oral sub mucous fibrosis. J Biomed Res 4(6):241-244.
- Naffah J (1977) Dermatoglyphics Analysis: Anthropological and Medical Aspects. Bulletin of The New York Academy Of Medicine 53(8):681-692.
- Prathibha Ramani, Abhilash PR, Herald J Sherlin, Anuja N, Priya Premkumar, et al. (2011) Conventional Dermatoglyphics–Revived Concept: A Review. Int J Pharm Bio Sci 2(3):446-458.
- Seema Mahajan, Gandhi D, Singh M (2012) Dermatoglyphic - study and review of literature. Int J Med Sci 1(6):191-198.
- Sharma A, Somani R (2009) Dermatoglyphic interpretation of dental caries and its correlation to salivary bacteria interactions. J Indian Soc Pedod Prevent Dent 1(27):17-21.
- Bhat PK, Badiyani BK, Chengappa S, Bhaskar NN (2012) Dermatoglyphics-A new diagnostic tool in detection of dental caries among deaf and mute children. Int J Clin Dent Sci 2(4):80-84.
- Mathew L, Hegde AM, Rai K (2005) Dermatoglyphics Pecularities in Children With Oral Clefts. J Saoc Apedod Prev Dent 23(4):179-182.
- Sharma MK, Sharma H (2012) Dermtoglyphics: A diagnostic Tool to Predict Diabetes. J Clin Diagn Res 6(3):327-332.
- Ravindranath R, Joseph AM, Bosco SI, Rajangam S, Balasubramanya V (2005) Fluctuating Asymetry In Dermatoglyphics Of Non –Insulin Dependent Dabetes Mellitus In Banglore – Based Population. Indian Journal of Human Genetics 11(3):149-115.
- Venkatesh E, Bagewadi A, Keluskar V, Shetti A (2008) Palmar dermatoglyphics in oral leukoplakia and oral squamous cell carcinoma patients. J Indian Academy of Oral Medicine and Radiology 20(3):94-99.





