Cone-Beam Computed Tomography Analysis of Mental and Genial Spinal Foramina in a Thai Population
Ebrahimi M1*, Pripatnanont P2, Omami G3, Tharanon W4
1 PhD Student, Faculty of Dentistry, University of Hong Kong, Hong Kong.
2 Associate Professor, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Prince of Songkla University, Hatyai, Songkhla, Thailand.
3 Clinical Assistant Professor, Oral Diagnosis and Polyclinics, Faculty of Dentistry, University of Hong Kong, Hong Kong.
4 Assistant Professor, Advanced Dental Technology Center, Bangkok, Thailand.
*Corresponding Author
Ebrahimi Mehdi DDS, HGD (OMFS), MSc,
Oral Rehabilitation,
Prince Philip Dental Hospital,
University of HongKong,
34 Hospital road, Sai Ying Pun, Hong Kong.
Tel: +852 2859 0412
E-mail: lahoot05@gmail.com
Article Type: Research Article
Received: January 09, 2015; Accepted: April 27, 2015; Published: April 28, 2015
Citation: Ebrahimi M, Pripatnanont P, Omami G, Tharanon W (2015) Cone-Beam Computed Tomography Analysis of Mental and Genial Spinal Foramina in a Thai Population. Int J Dentistry Oral Sci. 2(4) 65-71. doi: dx.doi.org/10.19070/2377-8075-1500014
Copyright: Omami G© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To investigate frequency, anatomic location, and morphology of mental and genial spinal foramina in a group of Thai population.
Materials and Methods: A total of 107 maxillofacial cone-beam computed tomography scans were collected and analyzed for frequency, anatomic location and morphology of mental and genial spinal foramina. Data were analyzed using Chi-Square test, one-way ANOVA and independent t-test. P values less than 0.05 were accepted as statistically significant. Results: The mental foramen was located at the apex of second premolar in 46%and between apices of premolars 35.8%. Round and oval mental foramina were found in 65% and 21% of patients, respectively. The superior and inferior genial spinal foramina were encountered in 80.3% and 32.7% of patients, respectively. The accessory mental foramen was identified in 6.6% of patients. The average distance from the center of mental foramen to the alveolar and basal borders of mandibular body was 11.70 ± 2.13 and 16.34 ± 3.79mm, respectively.
Conclusion: This study indicates that horizontal position of mental foramen in Thai population is remarkably variable. Cone beam computerized tomography is optimal for delineating diminutive anatomical structures in the anterior mandible. High prevalence rates of superior and inferior genial spinal foramina necessitate comprehensive CBCT screening before surgery in the interforaminal region of the mandible.
2.Introduction
3.Materials and Methods
3.1.Measurements
4.Results
4.1.Horizontal position of the mental foramen
4.2.Vertical position of mental foramen
4.3.Morphology of mental foramen
4.4.Accessory mental foramen
4.5.Dimension of mental foramen
4.6.Exit direction of mental foramen
4.7.Vertical position of superior andinferior genial spinal foramina
6.Discussion
7.Conclusion
8.References
Keywords
Mandible; Anatomy; Tomography; Dental Implant; Surgery.
Introduction
The locations of the mental foramen in relation to the roots apices must be precisely identified preoperatively to avoid damage of the mental nerve and vessels [1-3]. Sensory disturbances of the mental nerve after dental implant placement have been reported in 7% to 10% of cases [4, 5]. Moreover, loss of lip sensation may further be complicated by lip biting, impaired speech, and diminished salivary retention, which have a significant impact on a patient’s lifestyle.
The superior and inferior genial spinal foramina (SGSF, IGSF) and their corresponding bony canals are situated in the midline of the mandible, superior (or at the same level) and inferior to the genial spine respectively. These anatomical landmarks have been reported in 35% to 98% of mandibles [5-12].
Previous reports and reviews on surgical complications in the anterior mandible demonstrated that the presence of neurovascular structures should be carefully assessed before any surgical procedure in that region. As several authors reported on life-threatening hemorrhage in the floor of the mouth subsequent to implant placement in the mental interforaminal region [13-16]. Therefore, some reports have suggested a relationship between such a surgical incident and the presence of genial spinal (lingual) foramina [4, 15, 17, 18].
Conventional radiography of the mandible usually lacks clarity due to superimposition and geometric distortion, and consequently it often fails to demonstrate fine anatomical details. For instance, in a panoramic radiography study, the mental foramen was distally shifted compared to its actual position and magnified by about 23% [19].
Alternatively, recent advances in the 3D imaging modalities have significantly increased the availability of cross-sectional imaging for preoperative assessment of surgical sites. CBCT has superior detectability of the microanatomy of the dento-alveolar complex compared to medical CT because of higher spatial resolution, lower radiation exposure, reduced costs, and compact design. Therefore, CBCT scan would be optimal for visualization of genial spinal foramina.
The aim of this study was to investigate the frequency, anatomic location and morphology of mental and superior and inferior genial spinal foramina in a group of Thai population using CBCT images.
Materials and Methods
Maxillofacial CBCT scan volumes of patients referred to the Advanced Dental Technology Centre (ADTEC, Bangkok, Thailand) in a 2-year period were retrieved and screened for the exclusion criteria of low scan quality (11 cases), jaw deformity/surgery (2 cases), and non-Thai ethnicity (4 cases). The final study population comprised 107 patients (214 sites) (51 male, 55 female, 1 missing gender datum). Ages ranged from 10 to 72 years (mean,41 years) (9 missing age data).
All scans were obtained by I-CAT Cone Beam 3D imaging system (Imaging Sciences International, Inc, Hatfield, PA) with a flat panel detector. The exposure volume was set at 16cm (diameter) x 13cm (height), the voxel size was 0.2mm x 0.2 mm x 0.2 mm, and 14-bit gray scale. The scan was set at 90kV and 5mA, as recommended by the manufacturer. The DICOM files were analyzed in a PC workstation running Microsoft Windows 8 Enterprise (Microsoft Corp, Redmond, WA, USA) using the software (Denti Planversion 1.2 update 2; National Electronics and Computer Technology Center; NECTEC, Bangkok, Thailand).
Mandibular dental status was classified into four groups. Group 1: dentate; Group 2: partial dentate; Group 3: full edentulous; Group 4: mixed dentition. Premolar status was classified into three groups. Group 1: presence of both premolars; Group 2: absence of both premolars; Group 3: absence of one premolar.
All measurements were made by a single observer (M.E.). For assessment of intra-observer reliability and reproducibility, CBCT measurements of 10 patients were repeated twice. No statistically significant difference was detected as all the variations were within the range of standard deviation.
On the reformatted panoramic images, the horizontal position of the mental foramen was classified into 5 positions modified from the Al-Jasser et al [20] Position 1: anterior to the apex of 1st premolar; position 2: at the apex of 1st premolar; position 3: between the apices of premolars; position 4: at the apex of 2nd premolar and position 5: posterior to the apex of 2nd premolar (Figure 1).
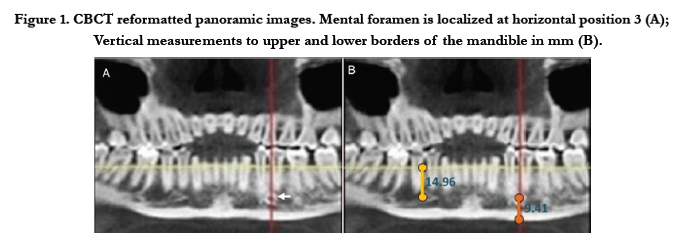
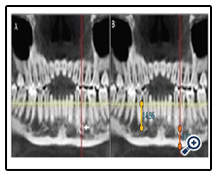
Figure 1. CBCT reformatted panoramic images. Mental foramen is localized at horizontal position 3 (A); Vertical measurements to upper and lower borders of the mandible in mm (B).
Vertical and horizontal dimensions of the mental foramen were measured from the outermost contours of foramen.
The vertical position of the mental foramen was measured in millimeter, from the centre of the mental foramen to the alveolar crest and the inferior border of the mandibular body, respectively.
The morphology of the mental foramen was simply evaluated and classified into three groups; oval, round and others.
On paracoronal images, the exit direction of the mental nerve was evaluated and classified into three types. Type I: upward exit; type II: straight exit; type III: downward exit. The vertical positions of the superior (SGSF) and inferior (IGSF) genial foramina were measured from the respective orifice to the lingual alveolar crest parallel to the long axis of the central incisor.
Data were analyzed using SPSS software for windows version 14. The means of the vertical and horizontal distances of the mental foramina were analyzed using independent T test and one way ANOVA where appropriate. Chi-Square test was used to relate the exit pattern and the horizontal position of mental foramen to gender and sides. P values less than 0.05 were reported as statistically significant.
Results
The position of the mental foramen was observed at the apex of second premolar (position 4), between apices of premolars (position 3), posterior to apex of second premolar (position 5), and at the apex of first premolar (position 2) in 46%, 35.8%, 15.3%, and 2.8% of patients, respectively.
The average vertical distance between the center of mental foramen and the basal border of mandibular body was 11.70 ± 2.13 mm. The average distance was almost similar on both sides (Right side; 11.79 ± 2.12 and left side; 11.67 ± 2.09), however, it was significantly greater in males (12.37 ± 2.46) compared to females (11.14 ± 1.53) (P < 0.001)(Figure 2).
Figure 2. Vertical distances from mental foramen to the lower border of the mandible in according to age (A) and side (B).
The average vertical distance between the center of mental foramen and the alveolar crest was 16.34 ± 3.79mm. The average distances of both sides were almost similar. This distance was greater in males (16.73 ± 3.94) than in females (15.98 ± 3.65) patients but it was not statistically significant (P = 0.12).
The average distance from the center of mental foramen to the root apex of the 1st premolar was 6.81 ± 2.34. This distance was not different on the right (6.75 ± 2.37) or left side (6.88 ± 2.33), but it was significantly greater in males (7.33±2.26) than in females (6.26±2.27)(P = 0.001).
The morphology of mental foramen was round in 65% and oval in 21%. The round shape was more common on the right side (69.2%), however, the oval shape was more common on the left side (25.3%) than on the right side (16.8%). However, there was no gender difference.
Accessory mental foramen (AMF) was found in 6.6% of patients (unilateral, 6.1% and bilateral, 0.5%). AMF was found on the right and left sides in 6.5% and 5.6% of patients, respectively. 3.8% in males and 2.8% in females.
The average horizontal dimension of mental foramen was 3.68 ± 0.76mm. This horizontal dimension was not different between males (3.73±0.76) and female (3.66±0.77). No difference was observed between the two sides.
The average vertical dimension of mental foramen was 3.61 ± 0.70. No side or gender differences were observed.
On cross-sectional CBCT images, the most common exit pattern of mental foramen was upward (74.8%) followed by straight pattern (25.2%). The downward pattern was not appreciated in any case (Figure 3).
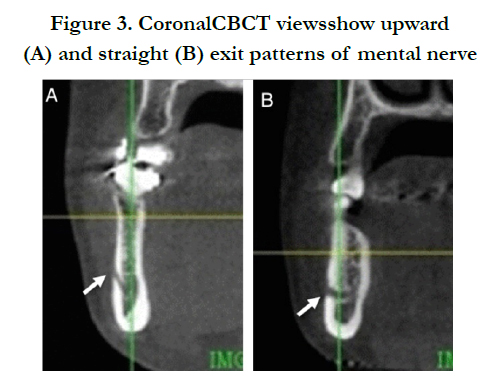
Figure 3. CoronalCBCT viewsshow upward (A) and straight (B) exit patterns of mental nerve
The upward exit pattern was noticed in 75.7% and 73.8% on the left and right sides, respectively. The straight exit pattern was found in 26.2% and 24.3% on the right and left sides, respectively. The upward pattern was more common in males (77.5%) than females (71.8%), however, the straight pattern was more evident in females (28.2%) than males (22.5%)(P > 0.05).
The superior and inferior genial spinal foramina were spotted in 80.3% and 32.7% of subjects, respectively. The mean vertical distances from superior and inferior genial spinal foramen to the lingual alveolar crest were 20.40 ± 3.47mm and 26.21 ± 3.79mm, respectively (Figure 3).
Both distances were greater in males but the differences were not statistically significant. (SGSF in male and female respectively = 20.95±3.78 and 19.97±3.08; IGSF in male and female respectively = 26.25±4.25 and 26.15±3.31).
Discussion
In agreement with our results [19, 21-26], many studies showed the location of the mental foramen aligned with the second premolar as the most common horizontal position (Table 1). However, other studies showed the most common site was between the apices of premolars [27, 28]. Therefore, the horizontal location of the mental foramen is a variable landmark and probably distinctive to race. In accordance with our study; Al-Khateeb et al [11] found the majority of mental foramina in a Jordanian population round in shape. This contrasts with studies on other populations where the most frequent shape was oval [21, 22, 29-32]. In a macroanatomic investigation, the diameter of mental foramen ranged from 2.38 –2.64mm of dry specimens [32], whereas that of AMF ranged from 0.74–0.89mm [33]. In comparison with our results, the diameters of mental foramina were greater (3.68 ± 0.76 x 3.61 ± 0.70), this disagreement is possibly due to differences in measurement protocols as we measured the diameter from the outermost contour of the foramen (Table 1).
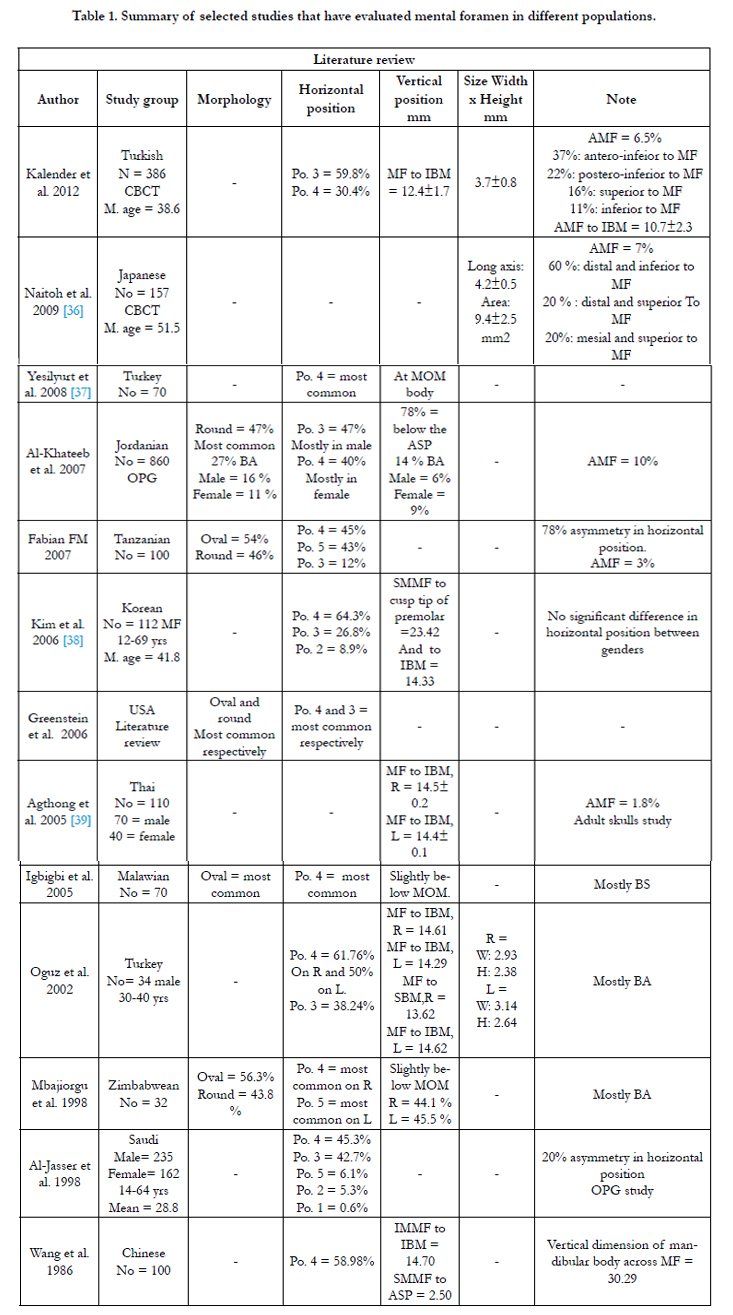

Table 1. Summary of selected studies that have evaluated mental foramen in different populations.
Generally it is more accurate to relate the position of mental foramen to the mandibular body rather than to the teeth, since the later are affected by factors such as malocclusion, attrition, race, and age. Gershenson et al. [34] reported that the location of the mental foramen in relation to the body and teeth depended on age and condition of teeth and periodontal bone. For children, it is closer to alveolar crest prior to tooth eruption then descends during tooth eruption. For edentulous people it is again closer to alveolar crest due to its resorption.
As the mandible in male is bigger than in female, the vertical distances of mental foramen to the upper and lower bony borders should be greater in males. We have found only the vertical distance from mental foramen to the inferior border of mandible in males was significantly greater than in females (Figure 2). In this study the distance of mental foramen to the upper and lower borders of the mandibular body was significantly lesser in patients elder than 60 years (Table 2). This finding is possibly due to alveolar bone loss increased with aging. In edentulous patients and in patients with missing both premolars, the corresponding distances were significantly lesser than when both were present or one was missing. So, as a result of aging or premolars loss, the mental foramen tends to shift toward the upper mandibular border.
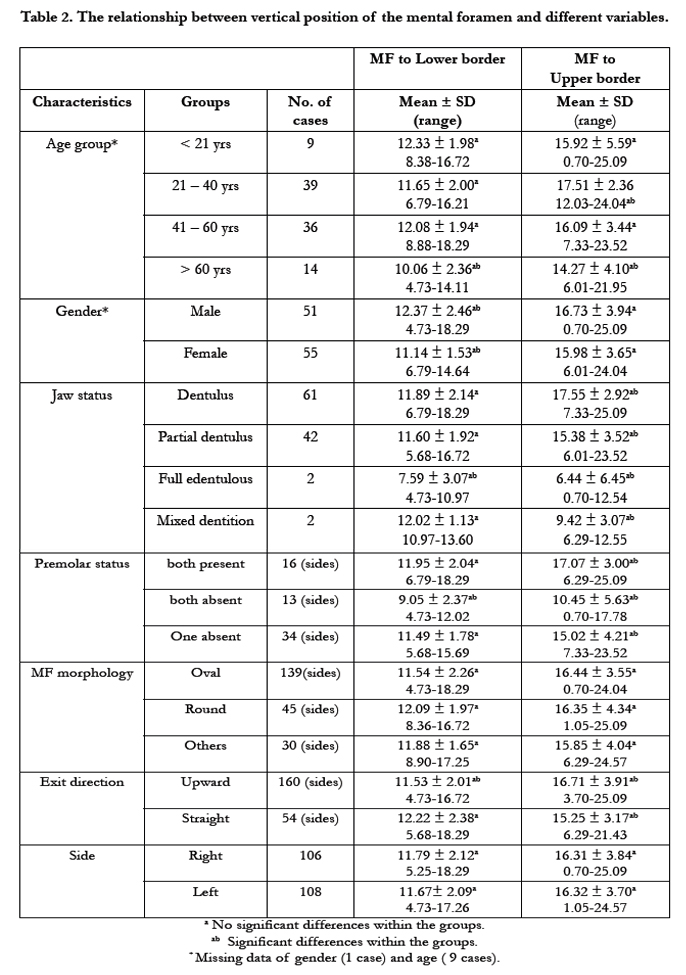
Table 2. The relationship between vertical position of the mental foramen and different variables.
In our study the distance of mental foramen to apices of premolars was remarkably great when compared to other study, [25] as we made the measurements from the center of the foramen rather than its outer rim (Table 1).
The vertical distance of the mental foramen to both upper and lower borders of mandibular body were significantly greater in patients with upward emergence direction compared to straight pattern.
For humans, the mental foramen is usually single, however, accessory mental foramen is occasionally reported. The frequency of AMF is reported to range from 1.4% to 9% with higher rates in Negro and Maori males [1, 2, 33]. The prevalence of AMF in our study was 6.6%. In accordance to Sawyer et al., we found no side difference in occurrence of AFM. The number of AFM may vary from one to three foramina [35]. Only one case in our series presented as double AMF.
Recent studies have indicated that both SGSF and IGSF and their respective canals contain neurovascular bundles, which could be visualized in high-resolution MRI and histological sections [6, 8].
The reported frequency of genial spinal foramina is highly variable (35%-98%) [5-12]. In this study the SGSF and IGSF have been detected in 80.3% and 32.7% of subjects, respectively (Figure 4). The vertical position of SGSF was significantly greater in younger age group (younger than 21 years old) compared to older age groups (P = 0.03), however, this was not the case for IGSF. In older patients these foramina and their corresponding canals were closer to alveolar ridge apparently due to bone resorption. Therefore, existence and locations of these foramina should be carefully considered to prevent perioperative complications, particularly hemorrhage.
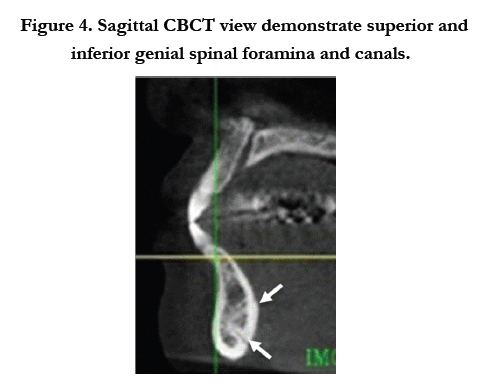

Figure 4. Sagittal CBCT view demonstrate superior and inferior genial spinal foramina and canals.
Conclusion
In conclusion, to best of our knowledge, this study was the first to investigate the radiographic anatomy of mental and genial spinal foramina in Thai population. The mental foramen was more commonly located along second premolar root. Additionally, the frequency of superior genial spinal and inferior genial spinal foramina was remarkably high. This finding necessitates comprehensive preoperative evaluation of the interforaminal region of the mandible.
References
- Kaufman E, Serman NJ,Wang PD (2000) Bilateral Mandibular Accessory Foramina and Canals: A Case Report and Review of the Literature. Dentomaxillofac Radiol 29(3): 170-17 5.
- Kalender A, Orhan K, Aksoy U (2012) Evaluation of the mental foramen and accessory mental foramen in Turkish patients using cone-beam computed tomography images reconstructed from a volumetric rendering program. Clin Anat 25(5): 584–592.
- Yildirim YD, Güncü GN, Galindo-Moreno P, Velasco-Torres M, Juodzbalys G, et al. (2014) Evaluation of Mandibular Lingual Foramina Related to Dental Implant Treatment With Computerized Tomography: A Multicenter Clinical Study. Implant Dent 23(1): 57-63.
- Mardinger O, Chaushu G, Arensburg B, Taicher S, Kaffe I (2000) Anterior loop of the mental canal: an anatomical-radiologic study. Implant Dent 9(2): 120-125.
- Wismeijer D, van Waas MA, Vermeeren JI, Kalk W (1997) Patients’ perception of sensory disturbances of the mental nerve before and after implant surgery: a prospective study of 110 patients. Br J Oral MaxillofacSurg 35(4):254-259.
- Liang X, Jacobs R, Lambrichts I, Vandewalle G, van Oostveldt D, et al. (2005) Microanatomical and histological assessment of the content of superior genial spinal foramen and its bony canal. DentomaxillofacRadiol 34(6): 362-368.
- Jacobs R, Lambrichts I, Liang X, Martens W, Mraiwa N, et al. (2007) Neurovascularization of the anterior jaw bones revisited using high-resolution magnetic resonance imaging. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 103(5): 683-693.
- Vandewalle G, Liang X, Jacobs R, Lambrichts I (2006) Macroanatomical and radiographic assessment of the superior and inferior genial spinal foramina and their bony canals. Int J Oral Maxillofac Implants 21: 581-586.
- Liang X, Jacobs R, Lambrichts I, Vandewalle G (2007) Lingual foramina on the mandibular midline revisited: a macroanatomical study. Clin Anat 20(3): 246-251.
- Pommer B, Tepper G, Gahleitner A, Zechner W, Watzek G (2008) New safety margins for chin bone harvesting based on the course of the mandibular incisive canal in CT. Clin Oral Implants Res 19(12): 1312-1316.
- Al-Khateeb T, Al-HadiHamasha A, Ababneh KT (2007) Position of the mental foramen in a northern regional Jordanian population. SurgRadiolAnat 29(3): 231-237.
- Hu KS, Yun HS, Hur MS, Kwon HJ, Abe S, et al. (2007) Branching patterns and intraosseous course of the mental nerve. J Oral MaxillofacSurg 65(11): 2288-2294.
- Katsumi Y, Tanaka R, Hayashi T, Koga T, Takagi R et al. (2013) Variation in arterial supply to the floor of the mouth and assessment of relative hemorrhage risk in implant surgery. ClinOral Implants Res 24(4): 434–440.
- Givol N, Chaushu G, Halamish-Shani T,Taicher S (2000) Emergency tracheostomy following life-threatening hemorrhage in the floor of the mouth during immediate implant placement in the mandibular canine region. J Periodontol 71(12): 1893–1895.
- Kalpidis CD, Konstantinidis AB (2005) Critical hemorrhage in the floor of the mouth during implant placement in the first mandibular premolar position: A case report. Implant Dent 14(2): 117–124.
- Mason ME, Triplett RG, Alfonso WF (1990) Life-threatening hemorrhage from placement of a dental implant. J Oral MaxillofacSurg 48(2): 201-204.
- Katakami K, Mishima A, Kuribayashi A, Shimoda S, Hamada , et al. (2009) Anatomical characteristics of the mandibular lingual foramina observed on limited cone-beam CT images. Clin Oral Implants Res 20(4): 386–390.
- Choi DY, Woo YJ, Won SY, Kim DH, Kim HJ, et al. (2013) Topography of the lingual foramen using micro-computed tomography for improving safety during implant placement of anterior mandibular region. J CraniofacSurg 24(4): 1403–1407.
- Phillips JL, Weller RN, Kulid JC (1992) The mental foramen: part III. Size and position on panoramic radiographic. J Endod 18: 383-386.
- Al-Jasser NM, Nwoku AL (1998) Radiographic study of the mental foramen in a selected Saudi population. DentomaxillofacRadiol 27(6): 341-343.
- Igbigbi PS, Lebona S (2005) The position and dimensions of the mental foramen in adult Malawian mandibles. West Afr J Med 24(3): 184-189.
- Mbajiorgu EF, Mawera G, Asala SA, Zivanovic S (1998) Position of the mental foramen in adult black Zimbabwean mandibles: a clinical anatomical study. Cent Afr J Med 44(2): 24-30.
- Shankland WE (1994) The position of the mental foramen in Asian Indians. J Oral Implantol 20(2): 118-123.
- Neo J (1989) Position of the mental foramen in Singaporean Malays and Indians. AnesthProg 36(6): 276-278.
- Wang TM, Shih C, Liu JC, Kuo KJ (1986) A clinical and anatomical study of the location of the mental foramen in adult Chinese mandibles. ActaAnat (Basel) 126(1): 29-33.
- Green RM (1987) The position of the mental foramen: a comparison between the southern (Hong Kong) Chinese and other ethnic and racial groups. Oral Surg Oral Med Oral Pathol 63(3): 287-290.
- Moiseiwitsch JR (1998) Position of the mental foramen in a North American, white population. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 85(4): 457-460.
- Santini A, Land M (1990)A comparison of the position of the mental foramen in Chinese and British mandibles. ActaAnat(Basel) 137(3): 208-212.
- Fabian FM (2007) Position, shape and direction of opening of the mental foramen in dry mandibles of tanzanian adult black males. Ital J AnatEmbryol 112(3): 169-177.
- Greenstein G, Tarnow D (2006) The mental foramen and nerve: clinical and anatomical factors related to dental implant placement: a literature review. J Periodontol 77(12): 1933-1943.
- Souaga K, Adou A, Angoh Y (2004) Topographical and morphological study of the mandibular foramen in black Africans from the Ivory Coast. Odontostomatol Trop 27(105):17-21.
- Oguz O, Bozkir MG (2002) Evaluation of location of mandibular and mental foramina in dry, young, adult human male, dentulous mandibles. West Indian Med J 51(1): 14-16.
- Toh H, Kodama J, Yanagisako M, Ohmori T (1992) Anatomical study of the accessory mental foramen and the distribution of its nerve. Okajimas Folia AnatJpn 69(2-3): 85-88.
- Gershenson A, Nathan H, Luchansky E (1986) Mental foramen and mental nerve: Changes with age. ActaAnat (Basel) 126(1): 21-28.
- Sawyer DR, Kiely ML, Pyle MA (1998) The frequency of accessory mental foramina in four ethnic groups. Arch Oral Biol 43(5): 417-420.
- Naitoh M, Nakahara K, Hiraiwa Y, Aimiya H, Gotoh K, et al. (2009) Observation of buccal foramen in mandibular body using cone-beam computed tomography. Folia AnatJpn 86(1): 25-29.
- Yeşilyurt H1, Aydinlioglu A,Kavakli A, Ekinci N, Eroglu C, et al. (2008) Local differences in the position of the mental foramen. Folia Morphol (Warsz) 67(1): 32-35.
- Kim IS, Kim SG, Kim YK, Kim JD (2006) Position of the mental foramen in a Korean population: a clinical and radiographic study. Implant Dent 15(4): 404-411.
- Agthong S1, Huanmanop T, Chentanez V (2005) Anatomical variations of the supraorbital, infraorbital, and mental foramina related to gender and side. J Oral MaxillofacSurg 63(6): 800-804.





