The Erosion Properties of Chlorine Dioxide and Hydrogen Peroxide on Bovine Teeth
Ablal MA1*, Jarad FD2, Adeyemi AA3
1 Department of Health Services research, Liverpool University Dental School, Pembroke Place, Liverpool, L3 5PS, UK.
2 Senior Clinical Lecturer/ Honorary Consultant in Restorative Dentistry, Liverpool University Dental Hospital, Pembroke Place, Liverpool, L3 5PS,UK.
3 NIHR ACL and Honorary STR in Periodontology, Liverpool University Dental School, Pembroke Place, Liverpool, L3 5PS, UK.
*Corresponding Author
Dr. Ablal MA BDS, MDentSci, PhD, MFDS RCSEd,
Department of Health Services research, Liverpool University Dental
School, Pembroke Place, Liverpool, L3 5PS, UK.
Tel: +44(0) 151 706 5622
E-mail: mabilal2003@yahoo.co.uk
Article Type: Research Article
Received: January 09, 2015; Accepted: February 02, 2015; Published: February 10, 2015.
Citation: Ablal MA, Jarad FD, Adeyemi AA (2015) The Erosion Properties of Chlorine Dioxide and Hydrogen Peroxide on Bovine Teeth. Int J Dentistry Oral Sci. 2(2) 42-46. doi: dx.doi.org/10.19070/2377-
8075-1500010
Copyright: Ablal MA© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objectives: The aim of this study was to assess the erosion potential of chlorine dioxide and hydrogen peroxide on bovine teeth.
Methods: Sixty bovine crowns were ground and polished to give flat surfaces. The crowns were subjected to heavy staining cycles then equally divided into 3 treatment groups; chlorine dioxide (ClO2), hydrogen peroxide (H2O2), and deionised water (H2O). Specimens in each group were immersed in 150 ml of the treatment for seven 2 min cycle in addition to an extra 30 min cycle. Specimens were gently dried after each 2 min cycle to take quantitative light-induced fluorescence (QLF) images while non- contact light profilometry (NCLP) scans were performed at the end of the seven 2 min and the extra 30 min cycles.
Results: ClO2 specimens showed a significant increase in %ΔF only after the first 2 min cycle (p < 0.05); however, a significant increase in %ΔF within H2O2 specimens was found at the end of the seven recommended treatment cycles (p < 0.05).
Conclusion: Chlorine dioxide does cause enamel erosion but to a lesser extent than that caused by hydrogen peroxide.
2.Introduction
3.Materials and Methods
4.Experimental Groups
4.1 Group 1: Chlorine dioxide (ClO2)
4.2 Group 2: Hydrogen peroxide (H2O2)
4.3 Group 3: Deionised water (H2O)
4.4 Statistical Analysis
5.Results
5.1 pH
5.2 Quantitative Light - Induced Fluorescence Data
5.3 Non - Contact Light Profilometry Data
6.Discussion
7.Conclusion
8.Acknowledgement
9.References
Keywords
Bovine enamel; Erosion; QLF; Fluorescence; NCLP; Mean step height
Introduction
Tooth discolouration is a common phenomenon that occurs due to extrinsic and/or intrinsic staining. The number of tooth whitening agents is on the increase to compensate for the increasing demand among a large number of people wanting whiter teeth. Peroxide bleaching, mainly hydrogen peroxide, is the commonly practised technique for whitening discoloured teeth. The safety, effectiveness, and various side effects of those products on intraoral structures have been widely investigated. Some of their associated and commonly reported potential side effects are erosion and porosity [1,2]. Low pH created by bleaching agents subjects teeth and oral tissues to an acidic environment for a period of time that could be considered sufficient to cause such side effects [3].
Investigations on the effects of pH on dental enamel suggested that low pH and high acid concentrations can cause enamel erosion [4]. In addition, possible alterations in the enamel organic matrix promoted by nonspecific and potentially reactive free radicals might result in decreased fracture toughness [3]. Chlorine dioxide tooth whitening* (Frontier Pharmaceutical Incorporation, New York, USA) has been considered as a ‘safer’ method for whitening teeth in shorter periods thereby avoiding the adverse effects usually associated with the use of peroxides [5]. Chlorine dioxide was first used in the form of Labarraque solution for bleaching non - vital teeth [6]. Currently, it is been used by non - dental establishments to whiten teeth.
Currently there is little in the literature to support the use of chlorine dioxide as a tooth whitening agent or to prove its safety for use on dental hard tissues. Only one article discussed the dangers of chlorine dioxide as a bleaching material and its subsequent side effects [7]. In the UK, a legal action was taken against a man who practised the use of chlorine dioxide and caused detrimental effects to the dentition of the 23 - year - old Stephanie Ramezan [8].
Dioxiwhite™ is marketed in the UK as tooth whitening agent. Its gel utilises chlorine dioxide as its active tooth whitening ingredient. Chlorine dioxide has strong oxidising properties and whitens teeth in a similar way to that reported with 35% hydrogen peroxide [9].
The main aim of this study was to assess, in vitro, whether chlorine dioxide has a dental erosion potential using quantitative light - induced fluorescence (QLF) and non - contact light profilometry (NCLP) in the assessment of dental erosion.
Materials and Methods
Sixty extracted bovine incisors devoid of intrinsic stains, cracks, and fractures were selected and had their roots separated. All crowns were ground and polished using 350 - grit and 1200 - grit SiC sandpaper (Wet and Dry Sandpaper, 151 Products Limited, Manchester, UK) under copious amounts of water until flat enamel surfaces were obtained. Each crown was then embedded in green impression compound material (Kerr Dental, USA) making approximately 2.5 x 2.5 x 1.8 cm blocks. These set of crowns were then subjected to the following extrinsic staining cycles:
The 60 blocks were attached to a total of 3 beakers containing staining fluids in the following sequence: a. 150 ml of artificial saliva (Table 1), b. 150 ml of chlorehexidine mouthwash (Chlorhexidine Gluconate 0.2%. v/w, ECOLAB, England) and c. 150 ml of tea (PG tips, UK). Artificial saliva was prepared in the laboratory and the tea solution was prepared by brewing 4 tea bags in boiling water and allowing the infusion to cool over a period of 30 min. The blocks were gently agitated (150 rpm, Bibby Sterilin, UK) for 2 min cycles in each staining solution until the stain intensity appeared unchanged on visual inspection (a total of 10 staining cycles). Subsequently, specimens were left overnight in deionised water allowing for stain maturation [10].
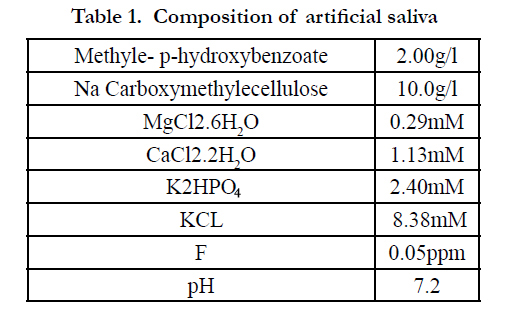

Table 1. Composition of artificial saliva
The blocks were then equally assigned to the following three experimental groups (n = 20 per group):
- Chlorine dioxide (Frontier Pharmaceutical Incorporation, NY, USA).
- Hydrogen peroxide (Fisher Scientific Ltd, UK) (positive control).
- Deionised water (negative control).
- Windows of 3 x 3 mm were created on each specimen using acid - resistant clear nail varnish (Maxfactor®, Procter and Gamble, Weybridge, UK) and allowed to bench - dry overnight.
- Baseline QLF™ images and NCLP scans were performed for all specimens.
- The pH of the three experimental materials was tested in triplicate and a mean pH value obtained.
The mounted crowns were subjected to a whitening regimen according to the manufacturer recommendations. They were bleached by the application of a 2 - 3 mm thickness of the gel and then exposed to an activating light source for 2 min. Seven treatment cycles were performed with an additional eighth cycle where ClO2 was left on the specimens for 30 min. After each cycle, specimens were washed with deionised water spray and a gentle air jet drying then left to further dry for 15 min.
Specimens in this group were treated with 35% (H2O2) at room temperature (21 ± 2°C). They were completely covered by the solution (150 ml) for seven, 2 min cycles in addition to the extra 30 min cycle. After each cycle, specimens were removed, rinsed with deionised water spray, dried with a gentle air jet and left to further dry for 15 min.
Specimens were immersed in deionised water (150 ml) following the same regimen for the two bleaching agents. After each cycle, they were gently air jet dried then left to further bench - dry for 15 min.
After each treatment cycle, QLF images were taken for all specimens. NCLP scans were performed at the end of cycle 7 and the extra 30 min cycle.
The results were analysed using SPSS statistical package (Version 15, SPSS Inc., Chicago, USA). Changes with values of p < 0.05 or less were considered statistically significant. Continuous variables were expressed as mean ± SD. Post hoc Tamhane test was performed to identify significantly different group means when ANOVA test was significant [11]. Paired t - test was carried out between baseline and each subsequent cycle.
The data in Figure 1 shows the pH values of the 3 experimentalmaterials. At baseline the pH values of ClO2 and H2O2 in conjunction with H2O were 3.35, 2.10, and 6.40, respectively.
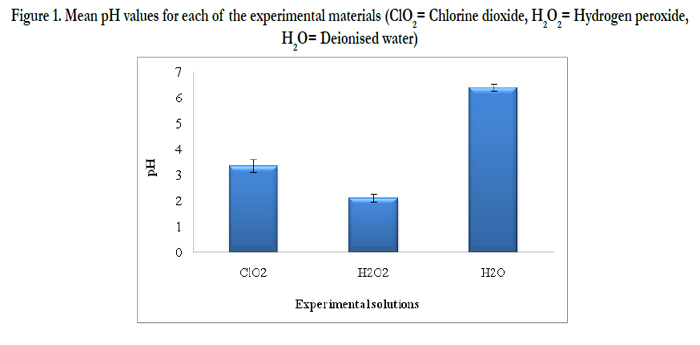
Figure 1. Mean pH values for each of the experimental materials (ClO2= Chlorine dioxide, H2O2= Hydrogen peroxide, H2O= Deionised water)
There was no significant difference in the change in mean fluorescence loss (% fluorescence loss) results when ClO2 and H2O2 were compared after the first three (C1 - C3) treatment cycles (p > 0.05). However, the next two cycles (C4 and C5) showed a significant increase in % fluorescence loss between the two treatments (p < 0.05). This increase in % fluorescence loss became highly significant as the treatment application continued for the rest of recommended cycles and the further 30 min cycle (p < 0.001) (Figure 2).
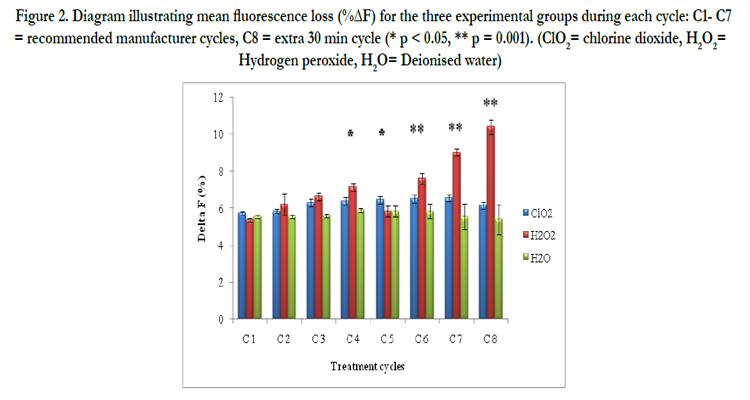
Figure 2. Diagram illustrating mean fluorescence loss (%ΔF) for the three experimental groups during each cycle: C1- C7 = recommended manufacturer cycles, C8 = extra 30 min cycle (* p < 0.05, ** p = 0.001). (ClO2= chlorine dioxide, H2O2= Hydrogen peroxide, H2O= Deionised water)
In the ClO2 group, the within group analysis showed a significantincrease in % fluorescence loss from baseline to cycle 1 (p <0.05). The subsequent cycles (C2 - C7) and the 30 min cycle, however, showed no significant difference in % fluorescence loss (p > 0.05). In contrast, H2 O2 specimens showed no significant difference (p > 0.05) in % fluorescence loss levels after the first six treatment cycles after which % fluorescence loss levels were significantly different (p = 0.001). However, this difference in % fluorescence loss was less significant (p = 0.05) when the application extended for the extra 30 min cycle.
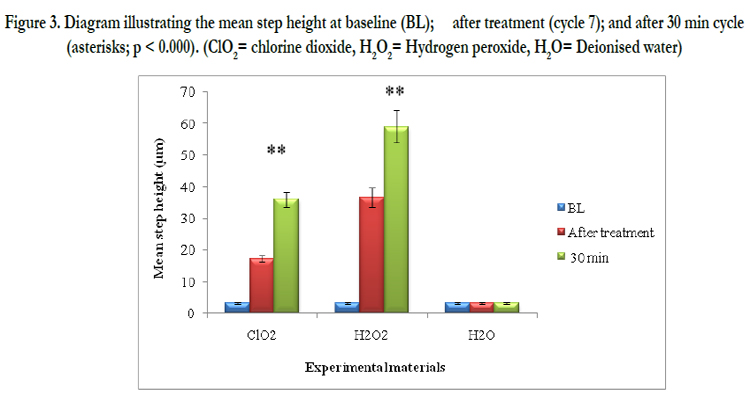

Figure 3. Diagram illustrating the mean step height at baseline (BL); after treatment (cycle 7); and after 30 min cycle (asterisks; p < 0.000). (ClO2= chlorine dioxide, H2O2= Hydrogen peroxide, H2O= Deionised water)
Specimens in both treatment groups showed a highly statistical significant increase in the mean step height after the recommended 7 and the extra 30 min cycles (p = 0.001) (Figure 3). However, the mean step height within the H2 O2 group was significantly greater than that for the ClO2 specimens (p = 0.000).
Discussion
Despite the controversy regarding their adverse effects; pulpal irritation [12,13], micro - leakage of restorations [14], reduced bond strength of resin materials [15,16] as well as external root resorption on teeth surface [17], peroxide bleaching remains the most commonly practised technique for whitening discoloured teeth. The low pH of these bleaching materials, manifesting itself in surface structure changes, is a major concern [18-20]. Enamel erosion occurs below the critical pH [21]. In the current study, the tested bleaching materials had pH values below the critical pH (2.10 and 3.35 for H2O2 and ClO2, respectively). However, ClO2 had a slightly higher pH indicating less erosive tendency than that of H2O2. Additionally, the intra- oral temperature was reported to be a factor that might affect the pH [22]. This study was carried out at room temperature which varied particularly on a warm or a cool day and further studies are needed to investigate this effect. Despite their whitening effect, peroxide bleaching side effects cannot be avoided either during or after the bleaching procedure. Depending on what concentration used, either high or low and the period of exposure, enamel demineralisation is inevitable [23]. H2O2 is capable of changing the apatite structure and the PO3- 4 is replaced with diperoxo (H4O4) ligands which are believed to be weaker [24,25].
Chlorine dioxide whitening gel used in the this study had a concentration similar to 35% hydrogen peroxide and, for the purpose of comparison of their effect, similar application regimen was used. QLF results showed that by the end of the seven 2 min application cycles, there was only 0.8% fluorescence loss as compared with fluorescence loss of 3.7% within the H2O2 group. Extending the application period to 30 min did not result in further increase in % fluorescence loss among ClO2 specimens while those treated with H2O2 had a slight increase in fluorescence loss by 1.4% (Figure 2). The less mineral loss from ClO2 specimens, expressed by the reduction in % fluorescence loss values, could be the result of the post - cycles air jet drying used to partly remove the gel from the treated surfaces and to partially dry them. Despite been carefully performed, using gentle air jet was able to remove demineralised surface layers because of their low mechanical properties. Consequently and after each cycle, this continuously may have caused the removal of the highly demineralised surface layer responsible for the reduced fluorescence loss and the exposure of the more mineralised subsurface layers. On the other hand, the increased % fluorescence loss among the H2O2 specimens could be the result of the dissociated hydrogen ions causing etching - like effect on the enamel surfaces as follows:
• Hydrogen peroxide dissociates into water and oxygen
2H2O2 → 2 H2O + O2
• Water then ionises to make four hydrogen and 2 hydroxyl ions
2 H2O → 2H+ + 2OH–
The effect of direct attack by those H+ ions is to combine with the carbonate and / or phosphate releasing all of the ions from that region of the enamel crystal surface leading to direct surface etching [26].
NCLP results were similar to those of QLF as ClO2 specimens had a mean surface loss of 17.2 μm at the end of cycle 7 as compared with 36.6 μm surface loss caused by H2O2 application. Surface loss increased after the 30 min application for both treatments reaching a mean of 36.0 μm and 58.9 μm for ClO2 and H2O2 specimens, respectively (Figure 3). Enamel surfaces had to be ground and polished to facilitate NCLP scanning. Such process was not without an impact as it usually results in the removal of the potentially protective salivary pellicle known to act as a diffusion barrier by its selective permeable nature against destructive acids [27,28]. Furthermore, grinding results in the removal of the highly mineralised prismless enamel at the surface layer facilitating acid penetration to the deeper, less mineralised layers [29]. It would have been advantageous to test enamel without changing the morphology of teeth surface.
Another factor that may contribute to the profound erosion effect by the two treatments is the structural differences between human and bovine enamel. It has been mentioned that due to their higher porosity as compared with human enamel, bovine teeth are less resistant to acid diffusion and therefore, lesions tend to increase rapidly [30].
A further post - treatment recommended by the manufacturer was the application of the WhiteLasting™ Maintenance Gel containing calcium hydroxyapatite and fluoride (< 1% and > 0.5%, < 0.5% and > 0.1%, respectively). This step is to be repeated by the subject at home once or twice a day for the following 7 days. The present study was designed to observe the effect of chair-side application on enamel when bleaching materials were in contact with the tooth substance for a maximum period of 30 min. Therefore, this final step was not performed and whether it enhances remineralising bleached tooth surfaces or not requires further investigation.
Conclusion
Within the limitations of this study chlorine dioxide does cause enamel erosion but to a lesser extent than that caused by hydrogen peroxide. Therefore, its application for domestic or professional use should be with caution and under supervision.
Acknowledgement
The authors would like to thank Frontier Pharmaceutical Incorporation for supplying the chlorine dioxide material tested in this study. Special thanks also go to the Libyan government for funding this study. The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
- RBT Price,M Sedarous,GS Hiltz (2000) The pH of tooth-whitening products. J Can Dent Assoc 66(8):421-426.
- LH Greenwall, GA Freedman, VV Gordan, VB Haywood, M Kelleher, et al. (2001) The bleaching materials In: Bleaching techniques in restorative dentistry: an illustrated guide. Martin Dunitz Ltd: London 31-60
- JA Rodrigues , RT Basting , MC Serra , AL Rodrigues Júnior (2001) Effects of 10% carbamide peroxide bleaching materials on enamel microhardness. Am J Dent 14(2):67-71.
- JA Hughes , NX West , DM Parker , MH van den Braak , M Addy (2000) Effects of pH and concentration of citric, malic and lactic acids on enamel, in vitro. J Dent 28(2): 147-52.
- Eric Montgomery, R (2010) "chlorine dioxide tooth whitening compositions". United States Patent; www.patentstorm.us/patents/6958144/ fulltext.html.
- JE Garretson (1895) A system of oral surgery.(6th Ed), JB Lippincott: Philadelphia. 230-32.
- LH Greenwall (2008) The dangers of chlorine dioxide tooth bleaching. Aesthetic Dentistry Today 2(4):21-3.
- Hall C. Salon uses industrial bleach to whiten teeth (2007) www.telegraph.co.uk/news/uknews/1541445/Salon-uses-industrial-bleach-towhiten-teeth.html
- F Lippert, GR Burnett (2008) In vitro dietary stain build-up on smooth and roughened teeth; GlaxoSmithKline Consumer Healthcare, Weybridge, United Kingdom.
- IA Pretty, WM Edgar, SM Higham (2001) The use of QLF to quantify in vitro whitening in a product testing model. Br Dent J 191(10): 566-69.
- BR Kirkwood, JAC Sterne (2003) Comparison of two means: confidence intervals, hypothesis t test and P-values In: Essential Medical Statistics (2nd Ed). Blackwell Science 58-70.
- W Buchalla , T Attin (2007) External bleaching therapy with activation by heat, light or laser--a systematic review. Dent Mater 23(5):586-96.
- CA Costa , H Riehl , JF Kina , NT Sacono , J Hebling (2010) Human pulp responses to in-office tooth bleaching. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109(4): e59-64.
- GA Crim (1992) Post-operative bleaching: effect on microleakage. Am J Dent 5(2): 109-12.
- AN Stokes , JA Hood , D Dhariwal , K Patel (1992) Effect of peroxide bleaches on resin-enamel bonds. Quintessence Int 23(11):769-71.
- VC Patusco , G Montenegro , MA Lenza , A Alves d e Carvalho (2009) Bond strength of metallic brackets after dental bleaching. Angle Orthod 79(1):122-6.
- I Rotstein , S Friedman , C Mor , J Katznelson , M Sommer, et al .(1991) Histological characterization of bleaching-induced external root resorption in dogs. J Endod 17(9):436-41.
- C Zantner , N Beheim-Schwarzbach , K Neumann , AM Kielbassa (2007) Surface microhardness of enamel after different home bleaching procedures. Dent Mater 23(2): 243-50.
- RF Mondelli , JF Azevedo , PA Francisconi , SK Ishikiriama , J Mondelli (2009) Wear and surface roughness of bovine enamel submitted to bleaching. Eur J Esthet Dent 4(4): 396-403.
- B Azrak , A Callaway , P Kurth , B Willershausen (2010) Influence of bleaching agents on surface roughness of sound or eroded dental enamel specimens. J Esthet Restor Dent 22(6): 391-9.
- RP Barron , RP Carmichael , MA Marcon , GK Sàndor (2003) Dental erosion in gastroesophageal reflux disease. J Can Dent Assoc 69(2): 84-9.
- Y Li (1998) Tooth bleaching using peroxide-containing agents: current status of safety issues. Compend Contin Educ Dent 19(8):783-6.
- RT Basting , AL Jr Rodrigues , MC Serra (2003)The effects of seven carbamide peroxide bleaching agents on enamel microhardness over time. J Am Dent Assoc: 34(10):1335-42.
- V Cavalli , CA Arrais , M Giannini , GM Ambrosano (2004) High-concentrated carbamide peroxide bleaching agents effects on enamel surface. J Oral Rehab: 31(2):155-9.
- F García-Godoy , MJ Hicks (2008) Maintaining the integrity of the enamel surface: the role of dental biofilm, saliva and preventive agents in enamel demineralization and remineralization. J Am Dent Assoc 139 :25S-34S.
- JD Featherstone, A Lussi (2006). Understanding the chemistry of dental erosion In: A Lussi. Dental erosion: from diagnosis to therapy. pp 66 -76. Basel, Karger, Switzerland
- C Ganss, J Klimek, N Schwarz (2000) A comparative profilometric in vitro study of the susceptibility of polished and natural human enamel and dentine surfaces to erosive demineralization. Arch Oral Biol 45(10): 897-902.
- A Cheung , Z Zid , D Hunt , J McIntyre (2005) The potential for dental plaque to protect against erosion using an in vivo-in vitro model--a pilot study. Aust Dent J 50(4): 228-34.
- J Xue , W Li , MV Swain (2009) In vitro demineralization of human enamel natural and abraded surfaces: a micromechanical and SEM investigation. J Dent 37(4): 264-72.
- R Schilke , JA Lisson , O Bauss , W Geurtsen (2000) Comparison of the number and diameter of dentinal tubules in human and bovine dentine by scanning electron microscopic investigation. Arch Oral Biol 45(5):355-61.





