Erupted Complex Odontoma Mimicking a Mandibular Second Molar
Almeida LE1*, Andrade MO2, de Oliveira Filho MA2, Trevilatto PC3, Doetzer AD3
1 Department of Surgical Sciences - Oral Surgery, School of Dentistry, Marquette University, USA.
2 Hospital Universitario Evangelico de Curtitiba, Brazil.
3 Pontifícia Universidade Católica do Paraná, Brazil.
*Corresponding Author
Luis Eduardo Almeida DDS, MS, PhD,
School Of Dentistry, 352, Po Box 1881, Milwaukee – 53201-1881, USA.
Tel: 262-271-6198
Fax: (21) 2243 9970
E-mail: almeidabuco@hotmail.com; lealmeida2@yahoo.com
Article Type: Case Report
Received: November 22, 2014; Accepted: December 16, 2014; Published: January 08, 2015.
Citation:Almeida LE, et al., (2015) Erupted Complex Odontoma Mimicking A Mandibular Second Molar. Int J Dentistry Oral Sci. 2(1), 26-28. doi: dx.doi.org/10.19070/2377-8075-150006
Copyright: Almeida LE © 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Complex odontoma (CO) is considered one of the most common odontogenic lesions, composed by a miscellaneous of dental tissue such as enamel, dentin, pulp and sometimes cementum. They may interfere with the eruption of an associated tooth, being more prevalent in the posterior mandible. CO has been rarely reported as erupted, being considered an intraosseous lesion. This is a case report of a 17-year-old male with a benign fibro-osseous lesion consistent with CO that was located at the left second molar region, above the crown of the impacted mandibular second molar tooth. The lesion was surgically removed, and the tooth had to be extracted, since there was no indication that it could erupt naturally or with orthodontic traction. The histopathological examination confirmed the diagnosis of CO and after 6 months complete bone formation was observed radiographically. An early diagnosis will provide a better treatment option, avoiding tooth extraction or a more damaging surgery.
2.Introduction
3.Case Report
4.Discussion
5.References
Keywords
Complex Odontoma; Impacted Tooth
Introduction
Odontoma was first described as a distinguished lesion by Broca in 1866. It is considered a hamartoma or a benign tumor containing
enamel, dentin, pulp and cementum, and account for 22% of all comprising odontogenic tumors [1]. According to the classification of the World Health Organization (WHO, 2005), there are two types of odontoma: compound odontoma and complex odontoma (CO), the first being twice as common as the latter. Compound odontoma resembles a tooth (or multiple tooth-like mass composing the lesion), as the complex odontoma contains tooth tissues in a disorganized manner.
COs are found in the mandible posterior region usually over impacted teeth which can reach up to several centimeters in size. Radiographically, these lesions manifest as a radiopaque solid mass with occasional nodular elements and are surrounded by a fine radiolucent zone separated from the normal bone by a well-defined cortication line [4].
Most cases (83.9%) occur before the age of 30 with a peak in the second decade of life. It is of interest to note that the majority of odontomas in anterior segment of jaw are compound composite in type (61%) whereas the majority in the posterior segment is CO [3]. Clinically CO is a painless, slow-growing lesion that is usually discovered on routine radiographs, or a failed permanent tooth eruption may lead to the diagnosis of this lesion [5].
Erupted odontomas in the oral cavity are rare, and the first case was published in 1980 by Rumel et al. The most common symptoms are pain, swelling, tongue irritation, halitosis, and infection, and most cases presented an impacted tooth associated with the lesion [2]. Hence, we present a case of a CO lesion that was located coronally to the crown of an impacted left mandible second molar.
Case Report
A 17-year-old boy was examined at the maxillofacial clinic of the Evangelic University Hospital of Curitiba, Brazil, complaining over an inflammation and pain at the region of the second inferior molar on the right side of the mandible. He had no significant medical history. Hypodontia, anodontia, and syndromic diseases were unknown in his family. There was no history of dental/maxillofacial trauma or infections. During the intra-oral evaluation, a bone-colored tooth-like mass with rough surface was identified at the posterior region of the first molar, and the second molar was not present clinically (figure 1). On clinical examination, the mandible appeared normal, without expansion of the cortical plates, and covered by normal mucosa. Around this mass, a mild inflammatory process was identified. A panoramic radiograph revealed a round radiopaque mass with an ill-defined borders that was more radiopaque peripherally and more radiolucent centrally, just above the second molar, which was impacted. The mesial root of this tooth was dilacerated, making it impossible to repositionate the tooth with orthodontic traction. The radiopaque mass was located exactly at the second molar site, mimicking its presence (figure 2).
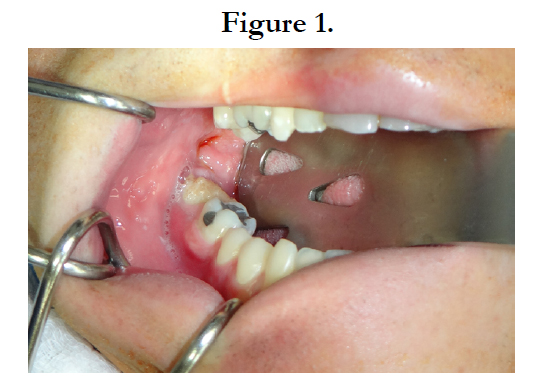

Figure 1.
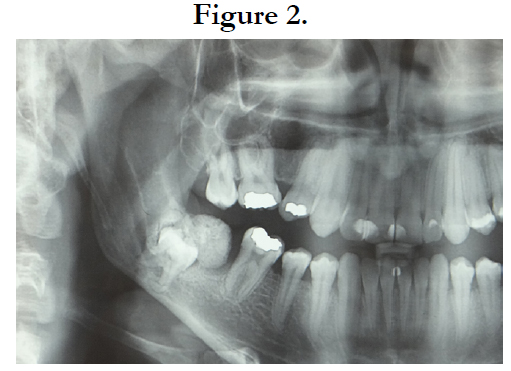

Figure 2.
Surgical excision was performed, the mass was removed (figure 3) and the tooth had to be extracted, since its roots were at the mandible base, and along with the dilacerated mesial root it made it impossible for traction or await for a spontaneous eruption. Removal of the mass was planned under local anaesthesia, a mucoperiosteal flap was raised mesial to tooth 47, and the CO was easily detached. The spherical mass was about 2 cm in diameter with small irregular areas; the specimen was sent for histopathological examination. However, a great amount of vestibular bone was removed to access and extract the 47 tooth. The surgery was concluded with a primary flap closure.
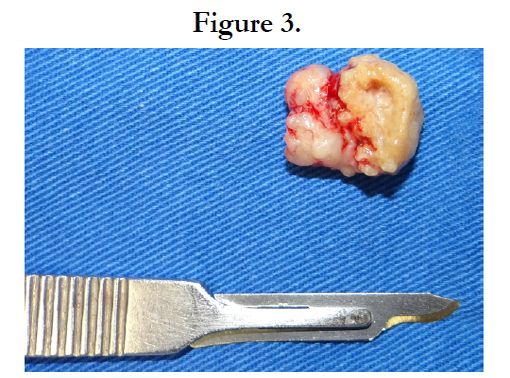

Figure 3.
A histopatological analysis confirmed the suggested diagnosis of CO. The histopathological findings included hard dental tissues arranged randomly, fibrovascular connective tissue, and chronic inflammatory cells. Adjacent areas showed thick, curvilinear, and hypo-cellular bone trabeculae with basophilic outlines and rare osteoblastic rimming in a background of vascular, but sparsely cellular connective tissue (figure 4).
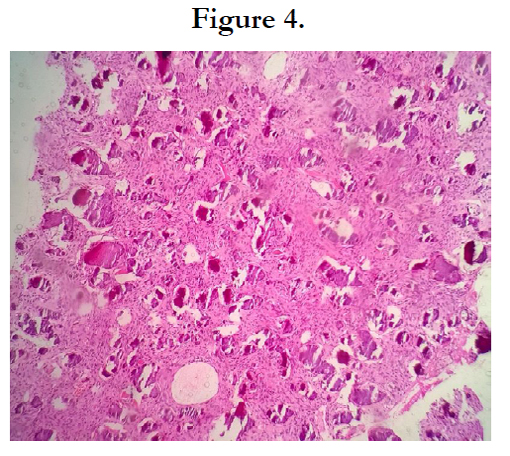
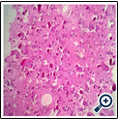
Figure 4.
The follow-up was carried out every three months, being the patient advised over the increased chance of pathological bone fracture. After one year, another panoramic radiograph was taken, and there was no sign of recurrence, and complete bone formation took place at the lesion site (figure 5).
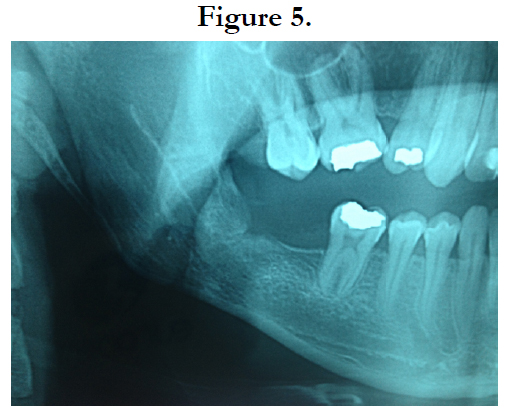

Figure 5.
Discussion
Odontogenic tumors are considered rare, hence, among these tumors, CO has a high incidence and whenever a tooth is oddly missing, its presence should be investigated. CO has an undefined etiology and several theories have been proposed, including infection, local trauma, and genetic mutation. The majority of odontomas in anterior segment of jaw are compound in type (61%) whereas in the posterior segment, they are CO. Interestingly both types of odontomas have a greater occurrence in the right side of jaw [4]. The permanent dentition is affected more frequently than the deciduous dentition, and it seems to be a male-to-female ratio of approximately 1.6:1.4, [6].
In most cases, odontomas are diagnosed in the first two decades of life. Nevertheless, only rarely clinical symptoms of odontomas can be observed. In fact, an odontoma diagnosis is incidental or the result of further exploration because of delayed tooth eruption [5]. Recently, the use of tomographic techniques, cone-beam computed tomography, has been suggested, however, because a lot of the patients with odontoma are children, the use of an extra radiography should be kept to a minimum [3]. Other pathologies should be excluded before surgery, such as osteoid osteoma, cementoblastoma, or cemento-ossifying fibroma which can be ruled out because they usually are not associated with impacted teeth. Malignant lesions generally do not present calcified elements; they exhibit a cystic architecture, and lack a clear border definition [8].
An analysis of several reports [5-7] over the odontoma associated with tooth impaction showed a ratio of maxillary incisors to mandibular molars retained by the presence of odontoma of 1.45:1. In only 5% of cases there was the retention of second mandibular molar, and odontoma is almost its only cause. Approximately half of odontomas arising in the mandibular molar area are associated with impacted teeth [3]. Thus, a delayed mandibular molar eruption may be associated with the occurrence of an odontoma, and should be investigated.
Erupted CO is extremely rare, and the exact mechanism for its eruption is still unclear. Some of the suggested mechanisms include bone remodeling of jaws and growth of odontoma leading to resorption of overlying bone. In this case report, a possible explanation could be the eruptive forces of the impacted tooth, promoting a sequestration of the overlying bone. The CO alone could not erupt, since it lacks periodontal ligament [9].
In conclusion, an experienced surgeon may diagnose a CO through clinical and radiographic evaluation, by identifying specific CO features. In the present case, a rare erupted odontoma was identified clinically and in the radiograph, being later confirmed by histopathologic analysis. The associated tooth unfortunately had to be removed due to its morphology and position. An early diagnosis of CO with tooth impaction is of great importance since it may contribute to a successful treatment, and the smaller the excised lesion is, a less invasive surgery needs to be applied.
References
- Soluk Tekkesin M, Pehlivan S, Olgac V, Aksakallı N, Alatli C (2011) Clinical and histopathological investigation of odontomas: Review of the literature and presentation of 160 cases. J Oral Maxillofac Surg 70(6):1358-61.
- G.Serra-Serra, L. Berini-Aytés, C. Gay-Escoda (2009) “Erupted odontomas:a report of three cases and review of the literature,” Medicina Oral , Patología Oral y Cirugía Bucal 14(6): 1–5 .
- Troeltzsch M, Liedtke J, Troeltzsch V, Frankenberger R, Steiner T et al (2012) Odontoma-associated tooth impaction: accurate diagnosis with simple methods? Case report and literature review. J Oral Maxillofac Surg 70(10):16-20.
- D. Nisha, K. Rishabh, T. Ashwarya, M. Sukriti, ,S. D. Gupta (2011) “An unusual case of erupted composite complex odontoma,” Journal of Dental Sciences and Research 2( 2):1–5.
- Hisatomi M , Asaumi JI, Konouchi H, Honda Y, Wakasa T et al (2002) A case of complex odontoma associated with an impacted lower deciduous second molar and analysis of the 107 odontomas. Oral Dis 8(2):100-5.
- da Silva LF, David L, Ribeiro D, Felino A (2009) Odontomas: A clinicopathologic study in a Portuguese population. Quintessence Int 40(1):61-72.
- Iatrou I , Vardas E, Theologie-Lygidakis N, Leventis M ( 2010) A retrospective analysis of the characteristics, treatment and follow-up of 26 odontomas in Greek children. J Oral Sci 52(3):439-47.
- Martin-Duverneuil N, Roisin-Chausson MH, Behin A, Favre-Dauvergne E, Chiras J (2001) Combined benign odontogenic tumors: CT and MR findings and histomorphologic evaluation. AJNR Am J Neuroradiol 22(5):867- 72.
- Vengal M, Arora H, Ghosh S, Pai KM (2007) Large erupting complex odontoma: a case report. J Can Dent Assoc 73(2):169-73.





