Current Status of Cardiovascular Tissue Engineering
Miyachi H1, Shoji T1, Sugiura T1, Fukunishi T1, Miyamoto S1, Breuer CK1, Shinoka T1,2*
1 The Tissue Engineering Program and Center for Cardiovascular and Pulmonary Research, Nationwide Children’s Hospital, Columbus, OH, USA.
2 Department of Cardiothoracic Surgery, The Heart Center, Nationwide Children’s Hospital, Columbus, OH, USA.
*Corresponding Author
Toshiharu Shinoka MD, PhD,
Professor, Department of Surgery, Ohio State University and Director,
Cardiovascular Tissue Engineering Program, Department of Cardiothoracic Surgery,
The Heart Center, Nationwide Children's Hospital 700 Children's Drive,
T2294, Columbus, OH 43205, USA.
Tel: 614-722-3103
Fax: 614-722-3111
E-mail: Toshiharu.shinoka@nationwidechildrens.org
Received: September 08, 2015; Accepted: October 12, 2015; Published: October 16, 2015
Citation: Shinoka T et al., (2015) Current Status of Cardiovascular Tissue Engineering. Int J Clin Ther Diagn. S3:001, 1-10. doi: dx.doi.org/10.19070/2332-2926-SI03001
Copyright: Shinoka T© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The development of vascular and heart valve surgeries have contributed to improve outcomes in patients with cardiovascular disease. However, there are drawbacks, such as risk of infection and lack of growth potential. Tissue engineered vascular graft (TEVG) and tissue engineered heart valve (TEHV) hold great promise to address these drawbacks as the ideal TEVG and TEHV is easily implanted, biocompatible, non thrombogenic, durable, degradable, and ultimately remodels into nativelike tissue. In general, the TEVG and/or TEHV concept consists of scaffold, cells for scaffold seeding, and a subsequent remodeling process driven by cell accumulation and proliferation, and/or biochemical and mechanical signaling. Despite rapid progress in the field over the past decade, small-diameter arterial TEVG and TEHV have not been translated into clinical applications successfully. To successfully utilize TEVGs and TEHVs clinically, further elucidation of the mechanisms for TEVG and TEHV remodeling and further translational research outcome evaluations will be required.
2.Tissue engineered vascular graft
2.1 Scaffolds
2.2 Cell
2.3 Signaling
2.4 Clinical studies for TEVG
3.Tissue engineered heart valve
3.1 The source of scaffold for TEHV
3.2 Cell sources and drug delivery
4.Summary and future perspective
5.References
Introduction
Atherosclerosis is a leading cause of death worldwide and includes coronary artery disease (CAD), aortic disease, peripheral artery disease (PAD), and cerebral vascular disease [1]. Atherosclerotic lesions are treated with either angioplasty or surgery with medication. In the CAD, coronary artery bypass grafting (CABG) is a common surgery, whereas numerous other atherosclerotic diseases require different vascular grafts. For example, vascular grafts are also employed in pediatric heart operations for congenital heart disease. For most CABG procedures, the main source of graft is autologous tissue harvested from either arteries, such as internal mammary artery or the saphenous vein. Autologous tissue grafts or synthetic vascular grafts such as expanded polytetrafluoroethylene (ePTFE; Goretex) or poly (ethylene terephthalate) (PET, Dacron) are also commonly used as vascular grafts [2, 3]. Despite the ready availability and clinical efficacy of these grafts, these materials have some drawbacks. Autologous tissue grafts are in short supply, thus making it difficult to perform multiple or repeat operations. Whereas, small-diameter (< 6mm) synthetic vascular grafts do not have a supply tissue, but display poor patency rates related to thrombosis and stenosis [4]. Another important consideration in these synthetic grafts is their lack of growth capacity, which is of particular concern for pediatric patients. The inability for natural graft growth necessitates reoperation with patient growth, and with it the inherent increased risk for morbidity and mortality. To address these challenges, the concept of tissue engineered vascular graft was generated, and the notion is in the spotlight.
Tissue engineered vascular graft
The definition of tissue engineering is the fabrication of alternative materials for the purpose of restoring biological and physiologic function at the site of defect or injury and eventually become integrated with a patient’s native tissue [5]. The basic concept of tissue engineering has 3 components: (1) a tissue-inducing scaffold material, (2) isolation and use of cells or cell substitutes, and (3) the integration of the isolated cells/substitutes and scaffold via a seeding technique [4, 6]. All three factors are interdependent and vital to the formation of highly organized neotissue. With regard to the integration of cells and scaffold, humoral and mechanical biological signaling is an important factor in the scaffold remodeling process. The ideal tissue engineered vascular graft (TEVG) would integrate with the patient’s native vessel to restore physiologic function and thus include: the ability to grow, to remodel, to respond to vasoactive hormones, and to rebuild after injury.
One key factors for successful TEVG fabrication is the choice of biomaterials used for the scaffolds. Currently, either synthetic or biological polymers can be used as scaffold materials for TEVG. These materials should enable neovessel development with less immune response, provide sufficient mechanical support to surrounding tissues, and biodegrade after neovessel formation.
In pursuit of ideal scaffolds, hundreds of synthetic polymers have been developed for TEVG purposes. Polyglycolic acid (PGA), Polylactic acid (PLA), and Poly (ε-caprolactone) (PCL) are the most widely used synthetic degradable polymers in animal models [7-9]. These polymers have different degradation rates, determined by initial molecular weight, exposed surface area, crystallinity, and ratio of monomers. The degradation periods of PGA, PLA, and PCL are 2-3 weeks, 6-12 months, and 12 weeks respectively [4, 10]. Additionally, combining these materials with other synthetic polymers can provide better mechanical properties and degradation rates. Copolymers, such as poly (L-lactide-co-ε-caprolactone) (PLCL or PCLA) and poly (L-lactic-co-glycolide) (PLGA) have already proposed and investigated by us and other researchers [11, 12]. Besides PLCL and PLGA, Polyhydroxyalkanoates (PHA), and comprising polyethylene glycol and a polycarbonate of dihydroxyacetone (MPEGPDHA) have been reported for use in synthetic scaffolds [13, 14]. Standard processing methods for these degradable polymer tissue scaffolds have included gas foaming, salt leaching, phase separation, freeze drying, 3D printing, and nanofiber electro spinning. Slow degradation of polymers enables the graft to better retain mechanical properties, but simultaneously make it more difficult for cellular infiltration and proliferation into grafts, therefore causing a delay in tissue remodeling. The electro spinning technique has been proposed as a promising method of fabricating vascular grafts (Figure 1). These ultrathin fibers have diameters in the range of 3 nm to 5 μm, and can be tailored to resemble the ECM structure, which is composed mainly of collagen and elastin fibrils [15]. As such, electro spun small-diameter scaffolds have displayed a high patency rate in addition to having good surgical and mechanical properties in an arterial graft model [8, 16].
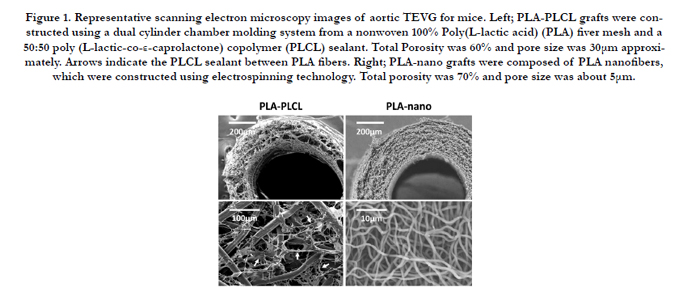

Figure 1. Representative scanning electron microscopy images of aortic TEVG for mice. Left; PLA-PLCL grafts were constructed using a dual cylinder chamber molding system from a nonwoven 100% Poly(L-lactic acid) (PLA) fiver mesh and a 50:50 poly (L-lactic-co-ε-caprolactone) copolymer (PLCL) sealant. Total Porosity was 60% and pore size was 30μm approximately. Arrows indicate the PLCL sealant between PLA fibers. Right; PLA-nano grafts were composed of PLA nanofibers, which were constructed using electrospinning technology. Total porosity was 70% and pore size was about 5μm.
The two main forms of biological scaffolds are decellularized tissues and ECM or ECM-like components, such as collagen or elastin. Decellularized tissue, often xenogenic, ought to contain an intact and structurally organized ECM. The decellularization process, which removes most cellular antigenic components, can be achieved through a combination of physical agitation, chemical surfactant removal and nucleotide remnants. Decellularized tissues lack cellular components and DNA, but have proper biocompatibilities and mechanical properties, similar to that of natural ECM. A well-known decellularized tissue is the small intestinal submucosa (SIS). The small-diameter SIS grafts implanted to ovine carotid and femoral arteries had similar mechanical properties to normal arteries [17] and SIS-fibrin hybrid scaffold implanted to carotid arteries showed high patency in sheep models [18]. However, the decellularization process can potentially place physical and chemical stress to the ECM, and adversely affect its biomechanical properties causing tissue deterioration which can lead to degenerative structural graft failure [19]. Additionally, further drawbacks of decellularized tissues include the inability to make modification to ECM content and architecture, and risk of viral and prion transmission from donor tissue.
Niklason et al. have reported a unique and interesting method of fabricating decellularized tissue for small-diameter arterial graft using biodegradable PGA scaffold [20, 21]. Allogenic aortic SMCs are cultured onto a PGA scaffold in a bioreactor, the engineered vessels were then decellularized, and seeded with autologous EPCs and ECs on the graft lumen. This engineered vessel had mechanical properties much like the human saphenous vein and gradually remodeled gradually, but a large drawback to this method id that it require long culture times.
ECM and ECM-like components are another biological scaffold type. These biological scaffolds are composed of natural ECM parts. Weinberg and Bell reported the first TEVG, using a collagen gel as a natural-material scaffold seeded with SMC and EC [22]. However, this TEVG lacked sufficient mechanical strength, and had to be integrated with a Dacron mesh to be evaluated in vivo. As an alternative to collagen, TEVG based on ovine SMC and EC embedded in fibrin gels have been developed. Similar to collagen, fibrin gels can achieve high seeding efficiency and uniform cell distribution [23]. Furthermore, when fibrin gels are combined with PLA and seeded autologous arterial-derived cells, the resulting endothelialized vessels have been successfully implanted in the carotid arteries of sheep [24].
TEVG requires viable cells for neotissue formation. The main components of a blood vessel are endothelial cells (ECs) in intima and smooth muscle cells (SMCs) in media. In addition, because of advancements in technology, stem cells have also attracted further attention for their potential use in TEVG. TEVG cellular incorporation can often provide the signals needed for tissue remodeling and rebuilding.
ECs possess a variety of physiological functions and synthesize many active substances, such as nitric oxide, fibronectin, heparan sulfate, interleukin-1, tissue plasminogen activator, and various growth-promoting factors [25]. The most important function is promotion of thromboresistance in TEVG. In 1978, Herring et al, introduced a technique for ECs seeding on non-biodegradable prosthetic materials. ECs were harvested from venous tissue by scarping the luminal surface [26]. Furthermore, implantation of EC-seeded ePTFE grafts resulted in significantly better outcomes compared to a non-seeded control group. According to these studies, the presence of a confluent EC monolayer on the luminal surface of a TEVG greatly enhances its thromboresistance and prevents the development of neointimal hyperplasia. On the other hand, the ECs composed pseudointima formed on synthetic TEVG was reported to function less than 10% of physiologic levels as compared with EC of native vessels. Additionally, EC have limited capacity for regeneration [27] and there is significant seeded EC loss that occurs in the first 24 hours of exposure to pulsatile flow, up to 95%, in an animal model [28]. Thus, it is thought that seeded ECs are mainly a means to prevent acute thrombosis. The mechanism for endothelialization of TEVG are proposed as followings; 1) seeded ECs, 2) the migration of ECs inward across the anastomosis from the native vessel, 3) the deposition of circulating endothelial progenitor cell (EPCs) onto the inner surface of synthetic TEVG [20, 29], and 4) ECs coverage from the ingrowth of capillaries through porous grafts (transmural endothelialization) [30]. EPCs are attractive sources of endothelialization, since they have the advantage of easy isolation via non-invasive sampling of peripheral blood. However, it remains controversial that there are adequate amounts of EPCs in peripheral blood to cover the luminal surface of TEVG as an endothelium.
It is widely accepted notion that in addition ECs, SMCs and fibroblasts are also essential to produce a stable intima. The ECM that ultimately defines the mechanical properties of a vessel are predominantly comprised of SMCs. In the 1980s-1990s, researchers reported TEVG seeding with SMCs, showed rapid neotissue formation when compared with unseeded control [31] and displayed physiological and mechanical functions comparable to native human vessels [32].
Recently, researchers have reported on the use of mesenchymal stem cells (MSCs), embryonic stem (ES), and induced pluripotent stem (iPS) cells for TEVG. The theoretical advantage to using stem cells as a cell source is that stem cells can be differentiated into mature cells with proper conditions and make it possible to obtain functional cells for tissue regeneration. Hashi et al, revealed not only that MSCs produced well-organized layers of ECs and SMCs, but also that MSCs have antithrombogenic properties [7], thus opening new possibilities for MSC use in TEVG.
BM-MNCs have undergone the most successful translation in human studies of TEVG. It was previously believed that the stem cell fraction within the seeded BM-MNCs population differentiated into the mature vascular cells of developing neovessel. However, we have revealed that the number of seeded cells in the graft decreased rapidly in the first few days after TEVG implantation, ultimately resulting in the absence of all BM-NMCs within 1 week post-implantation [33]. BM-MNCs contain an abundance of cytokines that can enhance neovessel development. Therefore more recently, it is believed that seeded BM-NMCs likely act in a paracrine manner to recruit additional host cells that work together to form neovessels. Some animal studies have demonstrated that TEVG seeded with BM cells may be a reasonable therapeutic option [34, 35]. We have suggested that BM-MNCs seeded TEVG are safe and effective to use in some arterial animal model and pediatric patients undergoing extracardiac total cavopulmonary connection procedures [36, 37]. Although several studies showed that BM-MNCs contribute to neovessel development and prevents thrombus and stenosis, the precise mechanism remains to be fully elucidated.
ES cells are pluripotent cells derived from early embryos. Shen et al, had developed a TEVG seeded with ECs derived from mouse ES cell. However, research on human ES cells is limited, since there are political and ethical concerns. On the other hand, iPS cell research is promising, because it does not have to consider the political and ethical problems associated with ES cell harvest, nor require immunosuppressive therapy. We have reported experience with iPS cell sheeted TEVG, and the cells also may function in a paracrine manner to induce neovascular formation. However, a number of obstacles must still be overcome prior to the implementation of iPS cells in TEVG applications [38].
Both biochemical and biological mechanical signaling are thought to be important factors in the scaffold remodeling process.
The former includes protein adsorption, complement activation, macrophage adhesion, giant cell formation, and ECM remodeling. It is known that an integrin on inflammatory cells plays a crucial role in the recognition of biomaterials, and absorbed proteins, such as albumin, fibrinogen, and others, modulate host inflammatory cell interactions and adhesion [39]. Macrophage adhesion occurs in response to chemokines and other chemoattractants, especially when wound healing and foreign body reactions are induced [40]. Furthermore, foreign body giant cells can release degradation mediators between the cell membrane and biomaterial surfaces. M-2 macrophages play an important role in ECM remodeling. As synthetic TEVG are implanted into the host, macrophages infiltrate actively formed ECM, and this milieu has shown to stimulate monocyte polarization into the M-2 anti-inflammatory phenotype [41]. M-2 macrophages have the ability to secrete chemotactic cytokines while simultaneously partially degrading ECM material in order to facilitate new tissue in-growth.
Blood vessels remodel in response to continually changing hemodynamic and metabolic conditions. In particular, shear stress and cyclic mechanical loading due to blood flow and pressure are important. Some investigators have demonstrated that ECs alter their production of many substances, expression of adhesion molecules, and growth factors in response to imposed shear stress both in vivo and in vitro [42, 43]. SMC growth response correlates with cyclic mechanical loading magnitudes. As a result, cyclic stretch influences both SMC synthetic and contractile phenotypes [44].
We have performed the first human clinical trial evaluating the use of TEVGs in congenital heart surgery [45]. We subsequently implanted 25 TEVGs as conduits for extra-cardiac total cavopulmonary connection with follow-up out through nine years [37] (Figure 2). There was no graft-related mortality and no evidence of aneurysm, graft rupture, graft infection, or ectopic calcification. Approximately 16% of patients had graft stenosis and underwent successful percutaneous angioplasties.
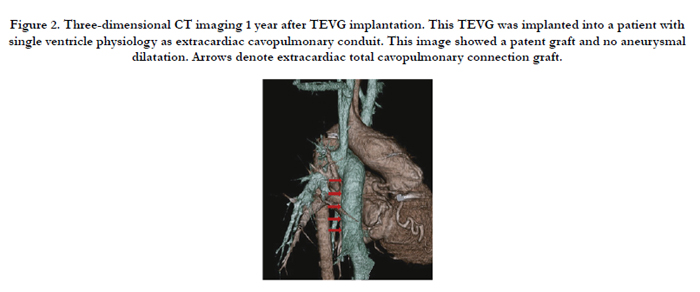

Figure 2. Three-dimensional CT imaging 1 year after TEVG implantation. This TEVG was implanted into a patient with single ventricle physiology as extracardiac cavopulmonary conduit. This image showed a patent graft and no aneurysmal dilatation. Arrows denote extracardiac total cavopulmonary connection graft.
L’Heureux et al. reported a new fabrication method called sheet-based tissue engineering in 1998 [46]. Sheets of living fibroblasts grown from cells extracted from patient biopsy samples were wrapped around a stainless steel mandrel and cultured. Subsequently, the inner plies were devitalized by air-drying, and ECs seeded into the lumen. The outer plies were living, and formed an adventitia equivalent. In the first clinical report, they have documented early (0-3 months) safety results for the first six patients implanted with arteriovenous shunt grafts for hemodialysis access [47]. They subsequently reported the 6 month follow-up data of the TEVGs implantation for first 10 patients and patency was 63% (5/8). However, two of the nine implanted grafts experienced early structural failure [48]. Subsequently, they developed an additional TEVG which differed by proactively isolating ECs and fibroblasts and storing it at -80°C for several months. Prior to implant, the TEVG was rehydrated, and its lumen seeded with living autologous endothelial cells to provide an antithrombogenic lining [49]. However, in 3 implants, 2 required interventions for stenosis (both eventually failed) and 1 patient died due to infectious causes [50]. It is clear, that further improvements will be needed in the future to use TEVG for chronic hemodialysis access usage as marketable products.
There are high hurdles to overcome regarding TEVG usage for arteries. The arterial TEVG must be durable enough to endure the arterial pressure, which differs from low venous pressure. Much research has been conducted in this area and has produced various TEVGs, Here, we introduce some arterial TEVG studies in large animal models.
As previously mentioned, electrospinning is promising method for fabricating synthetic TEVG for arteries. Mrowczynski et al. reported results of 22 porcine carotid artery replacements with a biodegradable electrospun PCL TEVG [51]. The one month patency rate was 78% (7/9) for electrospun PCL nanofiber grafts, compared with 67% (4/6) for the ePTFE control graft, but thePCL groups showed higher neo endothelialization percentage than the ePTFE group (86% vs 58%). Long-term follow-up is required, but this simple fabrication method is attractive.
Row et al investigated SMC and EC seeded SIS-Fibrin grafts that were implanted as left common carotid artery conduits in 20 sheep, and the patency was 100% (18/18, 2 died of reasons unrelated to the implants). The surprisingly successful patency rate is valuable in pre-clinical animal model, but the graft’s viability in a clinical setting is yet to be determined. Possible limitations to this particular graft are its seemingly expensive costs and the complex fabrication method to create the TEVG is complicated and the cost seems to be expensive.
Hymacyte (Hymacyte Incorporated, RTP, NC) developed a TEVG to function as a readily available off-the-shelf access method for large and small diameter graft applications [2]. The tissue manufacturing process of this tissue utilizes cadaveric SMCs to seed a PGA scaffold, cultured under radial strain. Subsequently, the TEVG is chemically decellularized prior to implantation [32]. In a series of large animal experiments, these decellularized TEVGs were implanted as coronary and peripheral arterial bypass in canines, and arteriovenous shunt in baboons. For the bypass procedures, the TEVG was seeded with autologous ECsto avoid acute thrombosis. The Hymacyte TEVG showed good patency (7/8 in baboon arteriovenous shunt and 5/6 in canine bypass model), and is currently undergoing clinical trials for hemodialysis access applications.
Mahara et al. have developed a decellularized, small caliber (2mm inner-diameter), and long (20-30cm) ostrich carotid artery graft modified with a novel heterobifunctional peptide composed of a collagen-binding region and the integrin a4b1 ligand expressed on ECs and EPCs. Subsequently, ECs and EPCs were seeded, and six grafts were transplanted in the femoral-femoral artery crossover bypass method to pigs. At 20 days the patency rate was 80% (5/6) [52].
Despite certain TEVGs showing promising results as arterial grafts, there are limitations regarding their use. Currently, TEVGsare commercially unavailable. Further studies will be required to obtain long-term patency rates and consistently safe outcome. Future arterial TEVGs need to be viable not only technically but also economically. The tissue engineering concept will fail to successfully translate to patients suffering from cardiovascular disease if the cost to utilize arterial TEVG clinically exceeds current medical costs. In addition, many cardiovascular diseases are time sensitive, and it currently takes several months for TEVGs to be produced. Patients requiring hemodialysis access, peripheral revascularization, and coronary artery bypass surgery may not have these valuable weeks or months to spare and wait for a new TEVG to be produced.
Tissue engineered heart valve
Heart valve malfunction constitutes a significant part of heart disease, and results in substantial morbidity and death worldwide [53]. Heart valve malfunction can be due to congenital heart disease (approximately 1% of newborns), or the deposition of mineralized calcium [54-56]. The treatment of heart valve malfunction requires surgical or interventional repair or replacement. Currently, the mechanical and bioprosthetic heart valve are used as clinically state-of-the-art of artificial valves [57, 58]. Mechanical heart valves have excellent durability, but are composed of foreign materials that may cause inflammation, infection and thromboembolic complications. Therefore, it requires anticoagulation therapy to prevent thromboembolism. Bioprosthetic heart valves, primarily composed of fixed porcine leaflets or bovine pericardium, are less thrombogenic, but are prone to calcification and progressive deterioration, particularly when implanted in younger individuals [58, 59]. Additionally, both mechanical and bioprosthetic heart valves share the disadvantage of representing nonviable structures that lack capacity to grow, remodel, regenerate or repair, especially in infant’ patients [60, 61]. As an alternative, the tissue engineered heart valve (TEHV) is a promising approach to overcome these drawbacks [6] as tissue engineering is a potential means of providing viable autologous cells or tissue [62].
In general, TEHVconsists of an unseeded or autologous cellseeded three-dimensional (3D) biocompatible and/or biodegradable scaffold. The TEHV provides a 3D template for specific tissues to develop into neotissue from their cellular components. The 3D scaffold provides an environment for cell attachment and tissue proliferation like a TEVG [63]. Cells seeded onto a TEHV, in vitro or in vivo, can develop into neotissue that will eventually replace the scaffold. We first introduced the concept of a TEHV in 1995 [64, 65]. We developed a polyglactin woven mesh, sandwiched between 2 non-woven polyglycolic acid (PGA) mesh sheets, to reconstruct right posterior pulmonary heart valve leaflets by myofibroblast and EC seeding. Subsequently, much ongoing research is being conducted to find the ideal TEHV.
To mimic heart valve organization, we must understand the structure of native heart valve. Semilunar valves in human (pulmonic and aortic valves) consist of three semicircular leaflets (cusps) attached to a fibrous annulus called the root [66]. The aortic valve cusps are supported by the aortic valve annulus and commissures. Cusp thickness is generally less than 1mm, and is typically thicker at the base and tip. The flexible valve leaflets (cusps) are composed of three distinct layers of the extracellular matrix (ECM): the fibrosa, spongiosa, and ventricularis [67, 68] (Figure 3). The fibrosa is located nearest the aorta and is composed of circumferentially oriented fibrillary collagens (Type I and III), which is associated with mechanical properties such as stiffness and strength of the cusp [69]. The spongiosa middle layer, consists of proteoglycans interspersed with collagen fibers. The layer works as a cushioned interface between fibrosa and ventricularis layers and has two functions; to provide valve integrity and facilitate its movement. The ventricularis, composed of alignedelastic fibers interspersed with short collagen fiber, enables valve extension and recoil under diastolic and systolic pressures. These layers are composed of valvular interstitial cells (VIC) within a collagen, elastin and glycosaminoglycan (GAG) matrix. The VICs that have features of both SMCs and fibroblasts are called myofibroblast [70]. The cusps are covered with a layer of ECs [71]. To date, several TEHVs that mimic the native valve have been developed. However, TEHVs that display sufficient mechanical performance, biological integrity, less inflammatory and immunogenic responses, encouragement of cell attachment and migration, and long-term durability have yet to be developed.
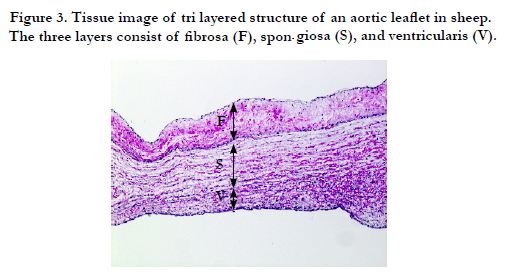
Figure 3. Tissue image of tri layered structure of an aortic leaflet in sheep. The three layers consist of fibrosa (F), spongiosa (S), and ventricularis (V).
Scaffold design, which includes material selection, goes a long way to define a TEHV’s success. Native heart valve structure consists of a spongy middle layer sandwiched between two laminar anisotropic fibrous layers. To mimic native heart valve structure, many scaffold designs have been proposed. Mainly two types of scaffold designs have been developed and evaluated; 1) biologicaland 2) synthetic-based materials. The former are decellularized native heart valve scaffolds from allogeneic/xenogeneic sources, and are fabricated with biological materials such as collagen, elastin, fibrin, alginate or chitosan, etc. The latter are artificial scaffolds fabricated from syntheticpolymers [66, 72].
The main sources of decellularized heart valve are xenogeneic valves from pigs, sheep, and cows, as allogeneic valves are in short supply. The advantage to using decellularized heart valves is being able to keep native valve structure and while preserving natural ECM complexity and integrity. ECM serves as heart valve structural support and a receiver for signaling factors, such as cell attachment, migration, and proliferation. With this in mind, ECM may be the appropriate scaffold choice for tissue repair and reconstruction [73]. There have been many different approaches to decellurize valve tissues and the list includes; chemical reagents, ionic detergentsand chelating agents, biological reagents, and physical methods, such as temperature, force, pressure, and non-thermal irreversible electroporation [74 - 85]. However, xenogenic material are prone to problems such as potential immunogenic reactions and the transmission of disease from animal to human [86, 87]. In particular, donor’ collagen may potentially have immunogenic response to recipient [88]. Moreover, the best known transmitted xenogenic diseases are caused by the porcine endogenous retrovirus (PERV) [89] and bovine spongiform encephalopathy (BSE) [90] which can cause Creutzfeld-Jakob disease. Decellularized tissue scaffolds modified by crosslinkers, such as glutaraldehyde or pentagalloyl glucose, to sterilize xenogenic valves minimize disease transmission, and reduce immunogenicity. Alternative fixation procedures such as dye-mediated photo-oxidation [91], carbodiimide/hydroxysuccinimide treatment [92], or ethanol/glycerol treatments followed by freeze-drying [93] are currently being investigated. In general, decellularization performed with a combination of reagents has shown advantages over single-agent treatments. Despite the many decellularization approaches, the clinical outcomes of decellularized xenogenic heart valves have been disastrous. According to the SynerGraft trial, 4 decellularized porcine heart valves were implanted as right ventricular outflow tract in four children. However, all four grafts failed due to a lack of durability and strong inflammatory response [19]. Contrastingly, favorable results have been reported with decellularized allogenic valves with respect to immunological responses, durability and overall clinical performance [94]. With regard to decellularized scaffolds relying on host recellularization, allogenic heart valves have proven to be far superior to xenogenic heart valves. However, the xenogenic heart valves have the distinct advantage of being in plentiful supply and research on its development continues.
Ozaki et al. recently showed that an original reconstruction method using autologous pericardium had favorable mid-term results [95, 96]. They treated pericardium with a 0.6% glutaraldehyde solution for 10 minutes, implanted the pericardium, and the tissue reformed manually as leaflets. The advantages of allogenic materials are their smaller immunogenic reactions and the absence of potential xenogenic disease transmission. In addition, the method demonstrated by Ozaki, may be able to overcome the general supply disadvantage that allogenic materials typically present.
Decellularized heart valve and heart valve scaffolds fabricated with biological materials share characteristics in that they both contain biological materials such collagen, elastin, fibrin, alginate or chitosan, etc. Thus, they have advantages in terms of cell adhesion, migration, proliferation and differentiation, but their drawbacks are the same as decellularized scaffolds and display vulnerable mechanical properties.
The advantages of synthetic-based scaffold include less immunogenicity and thrombogenicity [97]. Additionally scaffold absorbability, durability, and mechanical properties are controlled more easily. However, the disadvantages are that we cannot fully mimic the native tissues’s complex structure and function. Polyglycolic acid (PGA) and polylactic acid (PLA) synthetic polymer scaffolds were among the first investigated [65, 98]. After that, various synthetic materials have been proposed and reported, such as; poly-hydroxyalkanoates (PHAs) and poly-4-hydroxybutyrate (P4HB) [99, 100], poly-hydroxyoctanoate (PHO; member of the PHA family) [101], PGA and P4HB [102], poly (D,L-lactide-co-caprolactone) (PLCL) and poly (D,L-lactideco- glycolide) (PLGA) [103], and polyglycerol sebacate (PGS) [104]. In general, there are 3 TEHV scaffold types, and they include; 3D porous scaffolds, fibrous scaffolds, and hydrogels. The techniques to fabricate 3D porous scaffolds include particulate leaching, solvent casting, gas foaming, high internal phase emulsion, microfabrication, solid free-form (SFF) and 3D printing [105-107]. Currently, these techniques enable the fabrication of a variety of porous 3D scaffolds, with differing properties such as interconnectedness, homogeneity, and varying pore sizes. These pores allow nutrients and water to reach vascular cells and enable TEHV growth. Fibrous scaffolds fabrication techniques include electrospinning, phase separation, and self-assembly. Electrospinning is the most commonly used technique to fabricate tissueengineered scaffolds due to its versatility, polymer applicability, easy handling, and cost-effectiveness. Structurally similar to ECM, hydrogels are hydrophilic polymer chain networks with high water contents, and generally show high permeability to oxygen, nutrients and water-soluble metabolites. Tesng et al. explored trilayer poly (ethylene glycol) diacrylate (PEGDA) hydrogel quasilaminates that corresponded to the three layers of a native heart valve [108]. However, hydrogels have weak mechanical properties and their stiffness further decreases with cell seeding.
A combination of synthetic and biological scaffolds have also been investigated. Chitosan-modified PCL porous scaffolds were fabricated to improve attachment of fibroblast cells to a TEHV [109]. A composite scaffold composed of PLCL, PLGA and type 1 collagen has been tested to determine their efficacy in a TEHV. Other investigators have applied P4HA to mold PGA mesh into valve-shaped scaffolds [102, 110]. Additionally, PGA/PLLA composite fibrous scaffolds were studied to evaluate post-implant characteristics in heart valves [111], whereas PGS-PCL hybrid scaffolds have been studied to evaluate biodegradation and mechanical properties [112]. However to date, synthetic heart valves have yet to be applied in clinical setting.
Table 1 shows the recent large animal and clinical TEHV data. Although some TEHVs, based on decellularized biological-based materials are widely and commercially available, synthetic-based material TEHVs are not yet clinically available.
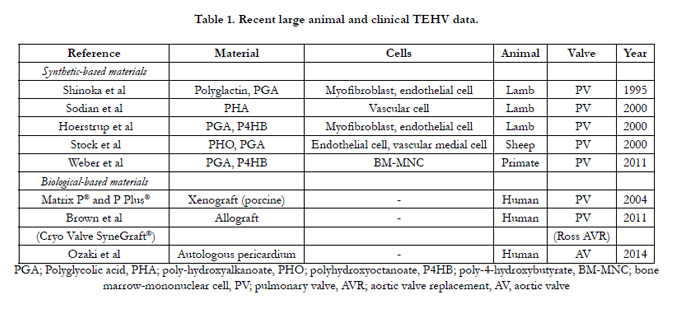

Table 1. Recent large animal and clinical TEHV data.
Since we investigated the TEHV seeded with fibroblast and ECs in 1995 [65], cells of various origins have been used for tissue engineered heart valves, such as adipose-derived cells [113], valve interstitial cells [114], peripheral vascular cells [65, 115], bone marrow stem cells, progenitor cells from blood or amniotic fluid, and umbilical cord vascular cells. These cells have been researched for their potential ability to recellularize, proliferate, or construct new heart valve tissue indirectly through chemical mediators, such as growth factors. However some cell sources, such as valve interstitial cells and peripheral vascular cells, necessitate the sacrifice of intact structures of donor organisms. Additionally, cell sources, such as progenitor cells from amniotic fluid and umbilical cord vascular cells, have low clinical feasibility due to their extremely limited supply. In contrast, bone marrow stem cells are an attractive alternative, as they are a source of hematopoietic cells and cells that can differentiate into non-hematopoietic cells, such as those of adipocytic, chondrocytic, or osteocytic lineages. These stem-like cells are currently referred to as marrow stromal cells (MSCs) and have several advantages; 1) It is easy to obtain as they can be collected by a simple puncture of the iliac crest under local anesthesia, 2) they show an extensive proliferation capacity in vitro, and 3) they have the potential to differentiate into various tissues [72]. Indeed, MSC derived human cells differentiate into a myofibroblast-like phenotype [116]. As such, the tissue engineering concept suggests that a favorable microenvironment will guide cellular differentiation towards phenotypes that are appropriate for autologous tissue replacement.
In the TEHV development process, growth factors are crucial for regulating cell migration and differentiation into the scaffold. In decellularized aortic heart valves, heparin-vascular endothelial growth factor (VEGF) coatings had an antithrombotic effect and induced adhesion, proliferation and migration of EPCs onto the scaffold [117]. When compared to unmodified decellularized scaffolds, decellularized valves modified with TGF-β loaded polyethylene glycol (PEG) nanoparticules, showed superior biocompatibility, biomechanical properties, and ECM microenvironments [118]. On the other hand, granulocyte colony-stimulating factor administration accelerated heart valve deterioration similar to that of observed in non- decellularized xenogenic biological valves [119]. Therefore, further research for additional growth factors will be needed to obtain desirable results.
Summary and future perspective
Patients with cardiovascular disease often require various vascular graft implantations and/or heart valve replacements. With regards to TEVGs, patients utilize autologous grafts and nonbiodegradable synthetic grafts, but suitable donor tissue for autologous graft is in short supply and synthetic grafts (particularly, small-diameter grafts) display lower patency rates, higher risks of infection, and the inability to grow or remodel. TEVGs hold great promise to resolve these problems. The rapid rise and development of tissue engineering for the past decade has enhanced the clinical feasibility of TEVGs. Investigators have focused on electrospinning technology because it enables scaffold constructs to be composed of either biodegradable synthetic polymers or biological polymers that resemble vascular tubes or flat sheets, and produced in a rapid, reliable, and cost effective manner [120, 121]. However, electrospun arterial TEVGs for artery have yet to be implanted in clinical trials.
On the other hand, using mechanical or biological hearts valves as state-of-the-art heart valve treatments are common worldwide and have improved life expectancies. However, there are some negative side effects in both types of heart valves. Mechanical heart valves require long-term anticoagulation treatment and biological heart valves lack durability and are potentially prone to calcification. In pediatric patients, both valves lack growth potential. To overcome these drawbacks, different TEHV concepts have been developed, which have the potential to remodel, regenerate, and grow into functional tissue constructs. Fabricated scaffolds should have appropriate three-layered structure/morphology, mechanical properties, and be able to regenerate functional ECM. Both biological-based and synthetic-based materials have good TEHV concepts, but each have their respective disadvantages. Biological-based materials have small pore sizes and low porosity, thus limiting cell survivability. Synthetic-based materials cannot fully mimic the trilayered structure of native heart valves, and to date have not display sufficient mechanical properties. Therefore, more research is needed to develop optimal scaffolds that can be applied in clinically.
To be widely accepted, TEVGs and TEHVs should be less invasive, cost effective, time saving, and readily available off-the-shelf. Although scaffold technology has progressed rapidly toward clinical use, cell culturing and seeding processes have several limitations, as they are technically complicated and have high costs. Bone marrow cells are a promising and attractive cell source as they are technically convenient to obtain. Patients must wait several weeks or months for TEVG and TEHV implantations requiring cell harvests, as approaches to collect cultured and conditioned cells requires time. Therefore, to successfully and safely utilize TEVGs and TEHVs clinically, more multidisciplinary, translational research will be have to be conducted.
References
- Herman JM, Hoffman JP, Thayer SP, Wolff RA (2015) Management of the Primary Tumor and Limited Metastases in Patients With Metastatic Pancreatic Cancer. J Natl Compr Canc Netw 13(5): e29-36.
- Dahl SL, Kypson AP, Lawson JH, Blum JL, Strader JT, et al. (2011) Readily available tissue-engineered vascular grafts. Sci Transl Med 3(68): 68ra9.
- Kurobe H, Maxfield MW, Breuer CK, Shinoka T (2012) Concise review: tissue-engineered vascular grafts for cardiac surgery: past, present, and future. Stem Cells Transl Med 1(7): 566-571.
- Tara S, Rocco KA, Hibino N, Sugiura T, Kurobe H, et al. (2014) Vessel bioengineering. Circ J 78(1): 12-19.
- Vacanti JP, Langer R (1999) Tissue engineering: the design and fabrication of living replacement devices for surgical reconstruction and transplantation. Lancet 354(Suppl 1): SI32-34.
- Langer R, Vacanti JP (1993) Tissue engineering. Science 260(5110): 920- 926.
- Hashi CK, Zhu Y, Yang GY, Young WL, Hsiao BS, et al. (2007) Antithrombogenic property of bone marrow mesenchymal stem cells in nanofibrous vascular grafts. Proc Natl Acad Sci USA 104(29): 11915-11920.
- Pektok E, Nottelet B, Tille JC, Gurny R, Kalangos A, et al. (2008) Degradation and healing characteristics of small-diameter poly (epsilon-caprolactone) vascular grafts in the rat systemic arterial circulation. Circulation 118(24): 2563-2570.
- de Valence S, Tille JC, Mugnai D, Mrowczynski W, Gurny R, et al. (2012) Long term performance of polycaprolactone vascular grafts in a rat abdominal aorta replacement model. Biomaterials 33(1): 38-47.
- Naito Y, Shinoka T, Duncan D, Hibino N, Solomon D, et al. (2011) Vascular tissue engineering: towards the next generation vascular grafts. Adv Drug Deliv Rev 63(4-5): 312-323.
- Roh JD, Nelson GN, Brennan MP, Mirensky TL, Yi T, et al. (2008) Smalldiameter biodegradable scaffolds for functional vascular tissue engineering in the mouse model. Biomaterials 29(10): 1454-1463.
- Thevenot PT, Nair AM, Shen J, Lotfi P, Ko CY, et al. (2010) The effect of incorporation of SDF-1alpha into PLGA scaffolds on stem cell recruitment and the inflammatory response. Biomaterials 31(14): 3997-4008.
- Gogolewski S, Jovanovic M, Perren SM, Dillon JG, Hughes MK (1993) Tissue response and in vivo degradation of selected polyhydroxyacids: polylactides (PLA), poly (3-hydroxybutyrate) (PHB), and poly (3-hydroxybutyrate- co-3-hydroxyvalerate) (PHB/VA). J Biomed Mater Res 27(9): 1135-1148.
- Zawaneh PN, Singh SP, Padera RF, Henderson PW, Spector JA, et al. (2010) Design of an injectable synthetic and biodegradable surgical biomaterial. Proc Natl Acad Sci USA 107(24): 11014-11019.
- Pham QP, Sharma U, Mikos AG (2006) Electrospinning of polymeric nanofibers for tissue engineering applications: a review. Tissue Eng 12(5):1197-1211.
- Wang S, Mo XM, Jiang BJ, Gao CJ, Wang HS, et al. (2013) Fabrication of small-diameter vascular scaffolds by heparin-bonded P(LLA-CL) composite nanofibers to improve graft patency. Int J Nanomedicine 8: 2131-2139.
- Hiles MC, Badylak SF, Lantz GC, Kokini K, Geddes LA, et al. (1995) Mechanical properties of xenogeneic small-intestinal submucosa when used as an aortic graft in the dog. J Biomed Mater Res 29(7): 883-891.
- Row S, Peng H, Schlaich EM, Koenigsknecht C, Andreadis ST, et al. (2015) Arterial grafts exhibiting unprecedented cellular infiltration and remodeling in vivo: the role of cells in the vascular wall. Biomaterials 50: 115-126.
- Simon P, Kasimir MT, Seebacher G, Weigel G, Ullrich R, et al. (2003) Early failure of the tissue engineered porcine heart valve SYNERGRAFT in pediatric patients. Eur J Cardiothorac Surg 23(6): 1002-1006.
- Quint C, Kondo Y, Manson RJ, Lawson JH, Dardik A, et al. (2011) Decellularized tissue-engineered blood vessel as an arterial conduit. Proc Natl Acad Sci USA 108(22): 9214-9219.
- Sundaram S, Niklason LE (2012) Smooth muscle and other cell sources for human blood vessel engineering. Cells Tissues Organs 195(1-2): 15-25.
- Weinberg CB, Bell E (1986) A blood vessel model constructed from collagen and cultured vascular cells. Science 231(4736): 397-400.
- Swartz DD, Russell JA, Andreadis ST (2005) Engineering of fibrin-based functional and implantable small-diameter blood vessels. Am J Physiol Heart Circ Physiol 288(3): H1451-1460.
- Koch S, Flanagan TC, Sachweh JS, Tanios F, Schnoering H, et al. (2010) Fibrin-polylactide-based tissue-engineered vascular graft in the arterial circulation. Biomaterials 31(17): 4731-4739.
- Vane JR, Anggard EE, Botting RM (1990) Regulatory functions of the vascular endothelium. N Engl J Med 323(1): 27-36.
- Herring M, Gardner A, Glover J (1978) A single-staged technique for seeding vascular grafts with autogenous endothelium. Surgery 84(4): 498-504.
- Walles T, Gorler H, Puschmann C, Mertsching H (2004) Functional neointima characterization of vascular prostheses in human. Ann Thorac Surg 77(3): 864-868.
- Rosenman JE, Kempczinski RF, Pearce WH, Silberstein EB (1985) Kinetics of endothelial cell seeding. J Vasc Surg 2(6): 778-784.
- Asahara T, Murohara T, Sullivan A, Silver M, van der Zee R, et al. (1997) Isolation of putative progenitor endothelial cells for angiogenesis. Science 275(5302): 964-967.
- Clowes AW, Kirkman TR, Reidy MA (1986) Mechanisms of arterial graft healing. Rapid transmural capillary ingrowth provides a source of intimal endothelium and smooth muscle in porous PTFE prostheses. Am J Pathol 123(2): 220-230.
- Yue X, van der Lei B, Schakenraad JM, van Oene GH, Kuit JH, et al. (1988) Smooth muscle cell seeding in biodegradable grafts in rats: a new method to enhance the process of arterial wall regeneration. Surgery 103(2): 206-212.
- Niklason LE, Gao J, Abbott WM, Hirschi KK, Houser S, et al. (1999) Functional arteries grown in vitro. Science 284(5413): 489-493.
- Roh JD, Sawh-Martinez R, Brennan MP, Jay SM, Devine L, et al. (2010) Tissue-engineered vascular grafts transform into mature blood vessels via an inflammation-mediated process of vascular remodeling. Proc Natl Acad Sci USA 107(10): 4669-4674.
- Noishiki Y, Tomizawa Y, Yamane Y, Matsumoto A (1996) Autocrine angiogenic vascular prosthesis with bone marrow transplantation. Nat Med 2(1): 90-93.
- Matsumura G, Hibino N, Ikada Y, Kurosawa H, Shin'oka T (2003) Successful application of tissue engineered vascular autografts: clinical experience. Biomaterials 24(13): 2303-2308.
- Kurobe H, Tara S, Maxfield MW, Rocco KA, Bagi PS, et al. (2015) Comparison of the biological equivalence of two methods for isolating bone marrow mononuclear cells for fabricating tissue-engineered vascular grafts. Tissue Eng Part C Methods 21(6): 597-604.
- Hibino N, McGillicuddy E, Matsumura G, Ichihara Y, Naito Y, et al. (2010) Late-term results of tissue-engineered vascular grafts in humans. J Thorac Cardiovasc Surg 139(2): 431-436.
- Hibino N, Duncan DR, Nalbandian A, Yi T, Qyang Y, et al. (2012) Evaluation of the use of an induced puripotent stem cell sheet for the construction of tissue-engineered vascular grafts. J Thorac Cardiovasc Surg 143(3): 696-703.
- Brodbeck WG, Colton E, Anderson JM (2003) Effects of adsorbed heat labile serum proteins and fibrinogen on adhesion and apoptosis of monocytes/macrophages on biomaterials. J Mater Sci Mater Med 14(8): 671-675.
- Esche C, Stellato C, Beck LA (2005) Chemokines: key players in innate and adaptive immunity. J Invest Dermatol 125(4): 615-628.
- Badylak SF, Gilbert TW (2008) Immune response to biologic scaffold materials. Semin Immunol 20(2): 109-116.
- Topper JN, Cai J, Falb D, Gimbrone MA Jr (1996) Identification of vascular endothelial genes differentially responsive to fluid mechanical stimuli: cyclooxygenase-2, manganese superoxide dismutase, and endothelial cell nitric oxide synthase are selectively up-regulated by steady laminar shear stress. Proc Natl Acad Sci USA 93(19): 10417-10422.
- Bao X, Lu C, Frangos JA (1999) Temporal gradient in shear but not steady shear stress induces PDGF-A and MCP-1 expression in endothelial cells: role of NO, NF kappa B, and egr-1. Arterioscler Thromb Vasc Biol 19(4):996-1003.
- Halka AT, Turner NJ, Carter A, Ghosh J, Murphy MO, et al. (2008) The effects of stretch on vascular smooth muscle cell phenotype in vitro. Cardiovasc Pathol 17(2): 98-102.
- Shin'oka T, Imai Y, Ikada Y (2001) Transplantation of a tissue-engineered pulmonary artery. N Engl J Med 344(7): 532-533.
- L'Heureux N, Paquet S, Labbe R, Germain L, Auger FA (1998) A completely biological tissue-engineered human blood vessel. FASEB J 12(1): 47-56.
- L'Heureux N, McAllister TN, de la Fuente LM (2007) Tissue-engineered blood vessel for adult arterial revascularization. N Engl J Med 357(14): 1451-1453.
- McAllister TN, Maruszewski M, Garrido SA, Wystrychowski W, Dusserre N, et al. (2009) Effectiveness of haemodialysis access with an autologous tissue-engineered vascular graft: a multicentre cohort study. Lancet 373(9673): 1440-1446.
- Wystrychowski W, Cierpka L, Zagalski K, Garrido S, Dusserre N, et al. (2011) Case study: first implantation of a frozen, devitalized tissue-engineered vascular graft for urgent hemodialysis access. J Vasc Access 12(1):67-70.
- Wystrychowski W, McAllister TN, Zagalski K, Dusserre N, Cierpka L, et al. (2014) First human use of an allogeneic tissue-engineered vascular graft for hemodialysis access. J Vasc Surg 60(5): 1353-1357.
- Mrowczynski W, Mugnai D, de Valence S, Tille JC, Khabiri E, et al. (2014) Porcine carotid artery replacement with biodegradable electrospun poly-ecaprolactone vascular prosthesis. J Vasc Surg 59(1): 210-219.
- Mahara A, Somekawa S, Kobayashi N, Hirano Y, Kimura Y, et al. (2015) Tissue-engineered acellular small diameter long-bypass grafts with neointima- inducing activity. Biomaterials 58: 54-62.
- Murray CJ, Richards MA, Newton JN, Fenton KA, Anderson HR, et al. (2013) UK health performance: findings of the Global Burden of Disease Study 2010. Lancet 381(9871): 997-1020.
- Jain R, Rentschler S, Epstein JA (2010) Notch and cardiac outflow tract development. Ann N Y Acad Sci 1188: 184-190.
- Marijon E, Celermajer DS, Tafflet M, El-Haou S, Jani DN, et al. (2009) Rheumatic heart disease screening by echocardiography: the inadequacy of World Health Organization criteria for optimizing the diagnosis of subclinical disease. Circulation 120(8): 663-668.
- Tanaka K, Sata M, Fukuda D, Suematsu Y, Motomura N, et al. (2005) Age-associated aortic stenosis in apolipoprotein E-deficient mice. J Am Coll Cardiol 46(1): 134-141.
- Hammermeister KE, Sethi GK, Henderson WG, Oprian C, Kim T, et al. (1993) A comparison of outcomes in men 11 years after heart-valve replacement with a mechanical valve or bioprosthesis. Veterans Affairs Cooperative Study on Valvular Heart Disease. N Engl J Med 328(18): 1289-1296.
- Vongpatanasin W, Hillis LD, Lange RA (1996) Prosthetic heart valves. N Engl J Med 335(6): 407-416.
- Pibarot P, Dumesnil JG (2009) Prosthetic heart valves: selection of the optimal prosthesis and long-term management. Circulation 119(7): 1034-1048.
- Boloori Zadeh P, Corbett SC, Nayeb-Hashemi H (2014) In vitro calcification study of polyurethane heart valves. Mater Sci Eng C Mater Biol Appl 35: 335-340.
- Grunkemeier GL, Rahimtoola SH (1990) Artificial heart valves. Ann Rev Med 41(1): 251-263.
- Dohmen PM, da Costa F, Yoshi S, Lopes SV, da Souza FP, et al. (2006) Histological evaluation of tissue-engineered heart valves implanted in the juvenile sheep model: is there a need for in-vitro seeding? J Heart Valve Dis 15(6): 823-829.
- Teebken OE, Bader A, Steinhoff G, Haverich A (2000) Tissue engineering of vascular grafts: human cell seeding of decellularised porcine matrix. Eur J Vasc Endovasc Surg 19(4): 381-386.
- Shinoka T (2002) Tissue engineered heart valves: autologous cell seeding on biodegradable polymer scaffold. Artif Organs 26(5): 402-406.
- Shinoka T, Breuer CK, Tanel RE, Zund G, Miura T, et al. (1995) Tissue engineering heart valves: valve leaflet replacement study in a lamb model. Ann Thorac Surg 60(6 Suppl): S513-516.
- Dohmen PM, Konertz W (2009) Tissue-engineered heart valve scaffolds. Ann Thorac Cardiovasc Surg 15(6): 362-367.
- Falk V, Walther T, Schwammenthal E, Strauch J, Aicher D, et al. (2011) Transapical aortic valve implantation with a self-expanding anatomically oriented valve. Eur Heart J 32(7): 878-887.
- Schoen FJ (2008) Evolving concepts of cardiac valve dynamics: the continuum of development, functional structure, pathobiology, and tissue engineering.Circulation 118(18): 1864-1880.
- Sacks MS, David Merryman W, Schmidt DE (2009) On the biomechanics of heart valve function. J Biomech 42(12): 1804-1824.
- Hajdu Z, Romeo SJ, Fleming PA, Markwald RR, Visconti RP, et al. (2011) Recruitment of bone marrow-derived valve interstitial cells is a normal homeostatic process. J Mol Cell Cardiol 51(6): 955-965.
- Combs MD, Yutzey KE (2009) Heart valve development: regulatory networks in development and disease. Circ Res 105(5): 408-421.
- Neuenschwander S, Hoerstrup SP (2004) Heart valve tissue engineering.Transpl Immunol 12(3): 359-365.
- Badylak SF (2002) The extracellular matrix as a scaffold for tissue reconstruction. Semin Cell Dev Biol 13(5): 377-383.
- Cox B, Emili A (2006) Tissue subcellular fractionation and protein extraction for use in mass-spectrometry-based proteomics. Nat Protoc 1(4): 1872-1878.
- Giusti S, Bogetti ME, Bonafina A, Fiszer de Plazas S (2009) An improved method to obtain a soluble nuclear fraction from embryonic brain tissue. Neurochem Res 34(11): 2022-2029.
- Lumpkins SB, Pierre N, McFetridge PS (2008) A mechanical evaluation of three decellularization methods in the design of a xenogeneic scaffold for tissue engineering the temporomandibular joint disc. Acta Biomater 4(4):808-816.
- Booth C, Korossis SA, Wilcox HE, Watterson KG, Kearney JN, et al. (2002) Tissue engineering of cardiac valve prostheses I: development and histological characterization of an acellular porcine scaffold. J Heart Valve Dis 11(4): 457-462.
- Funamoto S, Nam K, Kimura T, Murakoshi A, Hashimoto Y, et al. (2010) The use of high-hydrostatic pressure treatment to decellularize blood vessels. Biomaterials 31(13): 3590-3595.
- Yang B, Zhang Y, Zhou L, Sun Z, Zheng J, et al. (2010) Development of a porcine bladder acellular matrix with well-preserved extracellular bioactive factors for tissue engineering. Tissue Eng Part C Methods 16(5): 1201-1211.
- Klebe RJ (1974) Isolation of a collagen-dependent cell attachment factor. Nature 250(463): 248-251.
- Tarone G, Galetto G, Prat M, Comoglio PM (1982) Cell surface molecules and fibronectin-mediated cell adhesion: effect of proteolytic digestion of membrane proteins. J Cell Biol 94(1): 179-186.
- Hopkinson A, Shanmuganathan VA, Gray T, Yeung AM, Lowe J, et al. (2008) Optimization of amniotic membrane (AM) denuding for tissue engineering. Tissue Eng Part C Methods 14(4): 371-381.
- Lee RC, Kolodney MS (1987) Electrical injury mechanisms: electrical breakdown of cell membranes. Plast Reconstr Surg 80(5): 672-679.
- Lehr EJ, Rayat GR, Chiu B, Churchill T, McGann LE, et al. (2011) Decellularization reduces immunogenicity of sheep pulmonary artery vascular patches. J Thorac Cardiovasc Surg 141(4): 1056-1062.
- Sasaki S, Funamoto S, Hashimoto Y, Kimura T, Honda T, et al. (2009) In vivo evaluation of a novel scaffold for artificial corneas prepared by using ultrahigh hydrostatic pressure to decellularize porcine corneas. Mol Vis 15:2022-2028.
- Martin U, Kiessig V, Blusch JH, Haverich A, von der Helm K, et al. (1998) Expression of pig endogenous retrovirus by primary porcine endothelial cells and infection of human cells. Lancet 352(9129): 692-694.
- Simpson E (1998) Minor transplantation antigens: animal models for human host-versus-graft, graft-versus-host, and graft-versus-leukemia reactions. Transplantation 65(5): 611-616.
- Lynn AK, Yannas IV, Bonfield W (2004) Antigenicity and immunogenicity of collagen. J Biomed Mater Res B Appl Biomater 71(2): 343-354.
- Wilson CA, Wong S, Muller J, Davidson CE, Rose TM, et al. (1998) Type C retrovirus released from porcine primary peripheral blood mononuclear cells infects human cells. J Virol 72(4): 3082-3087.
- Knight R, Collins S (2001) Human prion diseases: cause, clinical and diagnostic aspects. Contrib Microbiol 7: 68-92.
- Carnagey J, Hern-Anderson D, Ranieri J, Schmidt CE (2003) Rapid endothelialization of PhotoFix natural biomaterial vascular grafts. J Biomed Mater Res B Appl Biomater 65(1): 171-179.
- Wissink MJ, van Luyn MJ, Beernink R, Dijk F, Poot AA, et al. (2000) Endothelial cell seeding on crosslinked collagen: effects of crosslinking on endothelial cell proliferation and functional parameters. Thromb Haemost 84(2): 325-331.
- Cheung DT, Weber PA, Grobe AC, Shomura Y, Choo SJ, et al. (2001) A new method for the preservation of aortic valve homografts. J Heart Valve Dis 10(6): 728-734.
- Brown JW, Ruzmetov M, Eltayeb O, Rodefeld MD, Turrentine MW (2011) Performance of SynerGraft decellularized pulmonary homograft in patients undergoing a Ross procedure. Ann Thorac Surg 91(2): 416-422.
- Ozaki S, Kawase I, Yamashita H, Nozawa Y, Takatoh M, et al. (2014) Aortic valve reconstruction using autologous pericardium for patients aged less than 60 years. J Thorac Cardiovasc Surg 148(3): 934-938.
- Ozaki S, Kawase I, Yamashita H, Uchida S, Takatoh M, et al. (2015) Aortic Valve Reconstruction Using Autologous Pericardium for Aortic Stenosis.Circ J 79(7): 1504-1510.
- Ravi S, Chaikof EL (2010) Biomaterials for vascular tissue engineering. Regen Med 5(1): 107-120.
- Shinoka T, Ma PX, Shum-Tim D, Breuer CK, Cusick RA, et al. (1996) Tissue-engineered heart valves. Autologous valve leaflet replacement study in a lamb model. Circulation 94(9 Suppl): II164-168.
- Sodian R, Hoerstrup SP, Sperling JS, Daebritz S, Martin DP, et al. (2000) Early in vivo experience with tissue-engineered trileaflet heart valves. Circulation 102(19 Suppl 3): III22-29.
- Sodian R, Sperling JS, Martin DP, Egozy A, Stock U, et al. (2000) Fabrication of a trileaflet heart valve scaffold from a polyhydroxyalkanoate biopolyester for use in tissue engineering. Tissue Eng 6(2): 183-188.
- Stock UA, Nagashima M, Khalil PN, Nollert GD, Herden T, et al. (2000) Tissue-engineered valved conduits in the pulmonary circulation. J Thorac Cardiovasc Surg 119(4 Pt 1): 732-740.
- Hoerstrup SP, Sodian R, Daebritz S, Wang J, Bacha EA, et al. (2000) Functional living trileaflet heart valves grown in vitro. Circulation 102(19 Suppl 3): III44-49.
- Park H, Radisic M, Lim JO, Chang BH, Vunjak-Novakovic G (2005) A novel composite scaffold for cardiac tissue engineering. In Vitro Cell Dev Biol Anim 41(7): 188-196.
- Masoumi N, Jean A, Zugates JT, Johnson KL, Engelmayr GC Jr (2013) Laser microfabricated poly(glycerol sebacate) scaffolds for heart valve tissue engineering. J Biomed Mater Res A 101(1): 104-114.
- Carletti E, Motta A, Migliaresi C (2011) Scaffolds for tissue engineering and 3D cell culture. Methods Mol Biol 695: 17-39.
- Gauvin R, Chen YC, Lee JW, Soman P, Zorlutuna P, et al. (2012) Microfabrication of complex porous tissue engineering scaffolds using 3D projection stereolithography. Biomaterials 33(15): 3824-3834.
- Leong KF, Cheah CM, Chua CK (2003) Solid freeform fabrication of threedimensional scaffolds for engineering replacement tissues and organs. Biomaterials 24(13): 2363-2378.
- Tseng H, Cuchiara ML, Durst CA, Cuchiara MP, Lin CJ, et al. (2013) Fabrication and mechanical evaluation of anatomically-inspired quasilaminate hydrogel structures with layer-specific formulations. Ann Biomed Eng 41(2): 398-407.
- Mei N, Chen G, Zhou P, Chen X, Shao ZZ, et al. (2005) Biocompatibility of Poly(epsilon-caprolactone) scaffold modified by chitosan--the fibroblasts proliferation in vitro. J Biomater Appl 19(4): 323-339.
- Weber B, Scherman J, Emmert MY, Gruenenfelder J, Verbeek R, et al. (2011) Injectable living marrow stromal cell-based autologous tissue engineered heart valves: first experiences with a one-step intervention in primates. Eur Heart J 32(22): 2830-2840.
- Eckert CE, Mikulis BT, Gottlieb D, Gerneke D, LeGrice I, et al. (2011) Three-dimensional quantitative micromorphology of pre- and post-implanted engineered heart valve tissues. Ann Biomed Eng 39(1): 205-222.
- Sant S, Iyer D, Gaharwar AK, Patel A, Khademhosseini A (2013) Effect of biodegradation and de novo matrix synthesis on the mechanical properties of valvular interstitial cell-seeded polyglycerol sebacate-polycaprolactone scaffolds. Acta Biomater 9(4): 5963-5973.
- Colazzo F, Sarathchandra P, Smolenski RT, Chester AH, Tseng YT, et al. (2011) Extracellular matrix production by adipose-derived stem cells: implications for heart valve tissue engineering. Biomaterials 32(1): 119-127.
- Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R, et al. (1999) Multilineage potential of adult human mesenchymal stem cells. Science 284(5411): 143-147.
- Hoerstrup SP, Zund G, Schoeberlein A, Ye Q, Vogt PR, et al. (1998) Fluorescence activated cell sorting: a reliable method in tissue engineering of a bioprosthetic heart valve. Ann Thorac Surg 66(5): 1653-1657.
- Kadner A, Hoerstrup SP, Zund G, Eid K, Maurus C, et al. (2002) A new source for cardiovascular tissue engineering: human bone marrow stromal cells. Eur J Cardiothorac Surg 21(6): 1055-1060.
- Ye X, Wang H, Zhou J, Li H, Liu J, et al. (2013) The effect of Heparin-VEGF multilayer on the biocompatibility of decellularized aortic valve with platelet and endothelial progenitor cells. PLoS One 8(1): e54622.
- Deng C, Dong N, Shi J, Chen S, Xu L, et al. (2011) Application of decellularized scaffold combined with loaded nanoparticles for heart valve tissue engineering in vitro. J Huazhong Univ Sci Technolog Med Sci 31(1): 88-93.
- Juthier F, Vincentelli A, Gaudric J, Corseaux D, Fouquet O, et al. (2006) Decellularized heart valve as a scaffold for in vivo recellularization: deleterious effects of granulocyte colony-stimulating factor. J Thorac Cardiovasc Surg 131(4): 843-852.
- Sell SA, McClure MJ, Garg K, Wolfe PS, Bowlin GL (2009) Electrospinning of collagen/biopolymers for regenerative medicine and cardiovascular tissue engineering. Adv Drug Deliv Rev 61(12): 1007-1019.
- Boland ED, Matthews JA, Pawlowski KJ, Simpson DG, Wnek GE, et al. (2004) Electrospinning collagen and elastin: preliminary vascular tissue engineering. Front Biosci 9: 1422-1432.





