Strongyloides Stercoralis: A Parasitic Infection That Can Persist Decades after Original Exposure
Rehman HU*, Kamrul R
Assistant Professor, Department of Academic Family Medicine, University of Saskatchewan, Canada.
*Corresponding Author
Rehman HU,
Clinical Associate Professor,
Department of Medicine, Regina,
Qu’Appelle Health Region,
Regina General Hospital, 1440 – 14th Avenue,
Regina, SK, S4P 0W5, Canada.
E-mail: habib31@sasktel.net
Received: June 23, 2014; Accepted: July 19, 2014; Published: July 26, 2014
Citation: Rehman HU, Kamrul R (2014) Strongyloides Stercoralis: A Parasitic Infection That Can Persist Decades after Original Exposure. Int J Clin Ther Diagn. 2(3), 48-51. doi: dx.doi.org/10.19070/2332-2926-140009
Copyright: Rehman HU© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Strongyloidiasis is a unique parasitic infection, which can cause hyperinfection or disseminated disease in immune suppressed patient several years after exposure due to the ability of the parasite to reproduce within the host. Prevalence rates vary widely. Most patients are asymptomatic. The most common risk factors for complications are immunosuppression caused by corticosteroids and infection with human T- lymphotropic virus type 1 (HTLV1).Diagnosis can be established by identifying the larvae in the stool; usually more than one sample is needed. But preferred diagnostic modality is serology. Treatment options for uncomplicated disease include Ivermectin, and Albendazole. Avoiding contact with infected soil can prevent disease.
2.Introduction
3.Epidemiology
4.Life Cycle
1.Free-living cycle
2.Parasitic cycle
5.Clinical Manifestations
6.Risk Factors for Dissemination
7.Diagnosis
8.Treatment
9.Post Treatment Follow up
10.Conclusion
11.References
Keywords
Strongyloides Stercoralis; Intestinal Parasites; Hyperinfection; Ivermectin; Albendazole.
Introduction
Intestinal parasites infect about one third of the world population.Strongyloides infection can continue for decades after a single exposure as subclinical infection or low-grade disease with nonspecific clinical manifestations. Immonucompromised patients can develop life threatening disseminated disease with case-fatality rates of over 70% .This infection has considerable public health implication to populations emigrating from developing areas of the world – where this parasite is prevalent – to industrialized areas of the world where they are non-endemic [1].
Epidemiology
Strongyloides stercoralis is a common intestinal nematode that affects 30–100 million people worldwide [2]. This parasite is found in the tropics, subtropics and in temperate areas and is endemicin Africa, the West Indies, Southeast Asia, Bangladesh, Pakistan, Central and South America. Clinicians need to be familiar with this disease because of the increased tourism and increasing number of immune suppressed patients worldwide [3].
Life Cycle
The Strongyloides life cycle is more complex than that of most nematodes with alternating free-living and parasitic cycles, and its potential for autoinfection and multiplication within the host [4]. Two types of cycles exist: Free-living cycle and Parasitic cycle.[Figure 1]
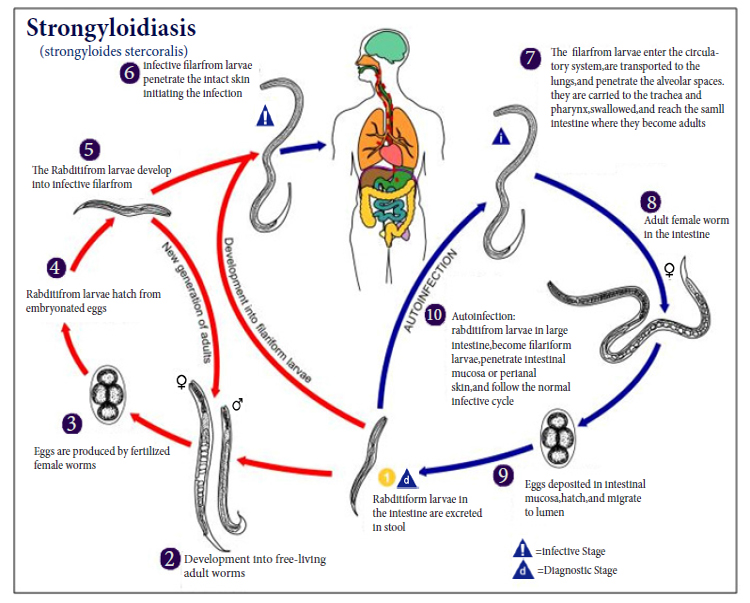
FIGURE 1. Life Cycle of Strongyloidiasis.
Source. US Centre for Disease control and Prevention/Alexander J. da Silva, PhD/Melanie Moser
The rhabditiform larvae passed in the stool can either molt twice and become infective filariform larvae or molt four times and becomefree living adult males and females that mate and produce eggs from which rhabditiform larvae hatch. The latter in turn can either develop into a new generation of free-living adults or into infective filariform larvae. The filariform larvae penetrate the human host skin to initiate the parasitic cycle.
Filariform larvae in contaminated soil penetrate intact human skin (usually the feet when people walk barefoot), and are transportedto the lungs where they penetrate the alveolar spaces; they are carried through the bronchial tree to the pharynx, are swallowed and then reach the small intestine. In the small intestine they molt twice and become adult female worms. The females live threaded in the epithelium of the small intestine and by parthenogenesis produce eggs, which yield rhabditiform larvae. The rhabditiform larvae can either be passed in the stool (see "Free-living cycle" above), or can cause autoinfection. In autoinfection, the rhabditiform larvae become infective filariform larvae, which can penetrate either the intestinal mucosa (internal autoinfection) or the skin of the perianal area (external autoinfection); in either case, the filariform larvae may follow the previously described route, being carried successively to the lungs, the bronchial tree, the pharynx, and the small intestine where they mature into adults; or they may disseminate widely in the body. To date, occurrence of autoinfection in humans with helminthic infections is recognized only in Strongyloides Stercorali and Capillaria Philippinensi infections In the case of Strongyloides, autoinfection may explain the possibility of persistent infections for many years in persons who have not been in an endemic area and of hyperinfections in immuno suppressed individuals.
Autoinfection can result in persistent infection for decades—up to 64 year after possible exposure in one report [5].
Clinical Manifestations
More than 50% of patients with chronic infection are asymptomatic, while others may show nonspecific symptoms such as diarrhea,nausea, and abdominal discomfort. Symptoms commonly involve gastrointestinal and respiratory tracts. Acute infection can result in a localized pruritic rash shortly after larval penetration [3]. Pulmonary symptoms include cough, dyspnea, hemoptysis and wheezing. Gastrointestinal (GI) symptoms develop several weeks later, just before appearance of the larvae in the stool. Chronic diarrhea, nausea, vomiting, progressive weight loss and abdominal discomfort are the most common GI symptoms. Dermatological manifestation like larvae currens (perianal rapidly moving and pruritic linear eruption) may also be found. About 75% of infected individuals have fluctuating eosinophilia.
Other common presentations are fever, gram negative/polymicrobial bacteremia due to migration of larvae through bowel wall [6]. Eosinophilia often absent in immune suppressed patients.
In patients with impaired cellular immunity (drug-induced or disease-associated), autoinfection may lead to a massive increase in parasite burden and dissemination to almost all organ systems, including the lungs, liver and central nervous system [7]. Hyperinfection and disseminated disease have been reported to occur in up to 2.5% of all cases of Strongyloides infection [3]. Hyperinfection syndrome or disseminated disease usually results in high mortality, but early diagnosis and timely therapy may result in improved patient outcomes. The clinical presentations of hyperinfection vary. Fever and chills may not always be present. The syndrome may result in malabsorption, paralytic ileus and ulcerative enteritis. Patients with hyperinfection who have peripheral eosinophilia appear to have a better prognosis than patients without peripheral eosinophilia [8]. Some patients with hyperinfection develop acute respiratory distress syndrome and may require intubation and mechanical ventilation. Alveolar hemorrhage has been reported in patients with Strongyloides hyperinfection after hematopoietic stem cell transplant [9].
Risk Factors for Dissemination
The risk factors for hyperinfection and disseminated disease are [10]:
1. Immunosuppressive therapy (particularly steroids which target T cells, have been documented as an important factor)
2. Human T-lymphotropic virus-1 (HTLV-1) infection
3. Solid organ transplantation
4. Hematologic malignant disease, especially lymphoma
5. Hypogammaglobulinemia
6. Chronic alcohol consumption
7. Uremia
8. Severe malnutrition
9. Diabetes mellitus.
Co-infection with HTLV-1 is an important risk factor for disseminated strogyloidosis. HTLV-1 is a retrovirus associated with adult T-cell leukemia and HTLV-1-associated myelopathy. In a review of 27 cases in the West Indies, HTLV-1 infection was the most common condition (71%) predisposing to dissemination [11]. In addition 6 of the 7 patients who died were HTLV-1 positive,which suggests that coinfection is may be a marker of a poor
prognosis.
Some areas of the world are endemic for both strongyloides and HTLV-1. Persons infected with the Human T cell lymphotropic virus (HTLV-1) have a modified immune response, which also complicates the treatment of Strongyloidiasis. As there is substantial association between HTLV-1 and strongyloidiasis it has been suggested to screen for the HTLV-1 if a patient found positive for Strongyloides infection and originate form an area with the high prevalence of HTLV-1 (South America, Caribbean, Japan, Africa) and/or patient who has persistent Strongyloidiasis that responds poorly to antiparasitic treatment [1]. In contrast, patients infected with HIV do not appear tobe at a higher risk for S. stercoralis hyperinfection. The organism was removed from a list of potential case definitions for AIDS in the late 1980s [3].
Diagnosis
Disseminated strongyloids infection carries a high fatality rate with the dissemination, so it is important to diagnose and treat the infection before initiating immunosuppressive therapy.
Since physicians may not be familiar with the disease, diagnosis is usually delayed. A case series included in an international survey report showed that immigrants from endemic areas with Strongyloides infections were frequently misdiagnosed for an average of 5 years in the US [12]. Moreover the sensitivity of stool examination for parasites is poor. Because of low parasite burden and intermittent larval excretion, single stool sample examination may miss70% or more of cases [1]. Diagnostic sensitivity increases to 50% with examination of 3 stool samples and is over 90% if 7 serial stool samples are examined [1].
Serologic testing with enzyme-linked immunosorbent assay is both sensitive and specific, with about 82%–95% sensitivity and 84%–92% specificity, and it can be an important diagnostic tool [2].
Eosinophilia is usually present in strongyloidiasis without hyperinfection, and is often absent in disseminated disease. Loutfy and colleagues found that 83% of patients with presumed strongyloidiasis had eosinophilia at the time of presentation [13]. Eosinopenia is now recognized as a marker of poor prognosis [2].
Patients who have visited or lived in endemic areas and present with GI symptoms (weight loss, diarrhea, abdominal pain, vomiting which is fitting with uncomplicated disease) or patient is asymptomatic but may be receiving corticosteroids or other immunosuppressive therapy in the near future need to be investigated with 3 serial stool samples screened for ova and parasites, and enzyme-linked immunosorbent assay (ELISA) for S.Stercoralis
serology [3].
Diagnostic procedure for patient who is unwell with pulmonary symptom (wheezing, respiratory distress), has gram negative or polymicrobial sepsis and has risk factors for disseminated disease will be blood and sputum culture for S. stercoralis, and culture of other specimen based on suspected organ involvement such as CSF and three serial stool samples screened for ova and parasites enzyme-linked immunosorbent assay (ELISA) for S.Stercoralis serology [2].
Treatment
Strongyloidiasis is a curable disease where early diagnosis and appropriate therapy can reduce associated mortality and improve patient outcomes.
The goals of therapy for strongyloidiasis are to treat symptomatic disease and prevent complications in asymptomatic disease by eradicating the organism to eliminate autoinfection that could lead to hyperinfection.
Treatment of strongyloidiasis depends on the patient's clinical status and underlying condition. Current treatment options for uncomplicated disease include thiabendazole, ivermectin, and albendazole. Thiabendazole at a dose of 25 mg/kg twice daily for 3 days (2 days in the US) was the standard of care for many years but produced significant adverse effects, especially nausea and dizziness. Ivermectin is much better tolerated than thiabendazole and has become the standard of care. Albendazole remains a potential alternative, but experience with its use is limited. According to the manufacturer of ivermectin, comparative international trials with albendazole showed an average cure rate of 84% versus 46%, respectively [3].
Patient with normal immune system who present with uncomplicated disease are treated with single drug ivermectin 200μg/kg once daily for 1 or 2 days or Albendazole 400 mg twice daily for 7 days. Treatment is repeated if necessary 2–3weeks after the first course to ensure eradication of infection.
Adverse effects of ivermectin are dizziness, pruritus and abdominal pain. Adverse effects of Albendazole are diarrhea, abdominal pain. In immune compromised patient treatment will be combination therapy with albendazole 400 mg twice daily for 7 d and ivermectin 200 μg/kg daily for 1–2 days. In cases of disseminated strongyloidiasis, albendazole and ivermectin are continued until there is evidence of parasitic clearance.
Test of cure with stool examination after therapy is insensitive, but monitoring a fall in Strongyloides antibody titres may be helpful.
Post Treatment Follow up
Several but not all studies have described Strongyloides antibody titers decline 6 to 12 month after successful treatment[1].So repeat serology can be done as a marker of clearance of this parasite. All treated individuals need to be followed clinically for persistent sign /symptom and need to ensure that eosinophil count return to normal limit within 6 month of receiving effective treatment.
Conclusion
Strongyloidiasis need to be recognised promptly in order to avoid disseminated and fatal infection. Though the primary site of Strongyloides infection is the gastrointestinal tract and associated symptoms such as abdominal pain and intermittent diarrhoea may be vague and if overlooked by the clinician, the diagnosis may be made only after dissemination and clinical deterioration of the patient. So it is important to obtain an appropriate travel and migration history from patients and to identify risk factors for disseminated infection for establishing early diagnosis.
References
- Pottie K, Greenaway C, Feightner J, Welch V,Swinkels H, et al. (2011) Evidence-based clinical guidelines for immigrants and refugees. CMAJ 183(12):824-925.
- Lim S, Katz K, Krajden S, Fuksa M, Keystone JS, et al. (2004) Complicated and fatal Strongyloides infection in Canadians: risk factors, diagnosis and management. CMAJ 171(5):479-84.
- Segarra-Newnham M. Manifestations (2007) diagnosis and treatment of Strongyloides stercoralis Infection. Ann Pharmacother 41:1992-2001.
- Centers for Disease Control and Prevention (2014 ) Strongyloidiasis.www.dpd.cdc.gov/dpdx/HTML/Strongyloidiasis.htm.
- Hauber HP, Galle J, Chiodini PL (2005) Fatal outcome of a hyperinfectionsyndrome despite successful eradication of Strongyloides with subcutaneousivermectin. Infection 33:383-6.
- Link K, Orenstein R (1999) Bacterial complications of strongyloidiasis: Streptococcus bovis meningitis. South Med J 92:728-31.
- Longworth DL, Weller PF (1986) Hyperinfection syndrome with strongyloidiasis. In: Remington JS, Swartz MN, editors. Current clinical topics in infectious diseases.New York: McGraw-Hill p. 1.
- Keiser PB, Nutman TB (2004) Strongyloidesstercoralis in the immunocompromised population.ClinMicrobiol Rev 17:208-17.
- Gupta S, Jain A, Fanning TV, Couriel DR, Jimenez CA, et al. (2006) An unusual cause of alveolar hemorrhage post hematopoietic stem cell transplantation: a case report. BMC Cancer 6:87.
- Concha R, Harrington W, Rogers AI (2005) Intestinalstrongyloidiasis: recognition, management, and determinants of outcomes. J ClinGastroenterol 39:203-11.
- Adedayo O, Grell G, Bellot P (2002) Hyperinfectivestrongyloidiasis in the medicalward: review of 27 cases in 5 years. South Med J 95(7):711-6.
- Boulware DR, Stauffer WM, Hendel-Paterson BR (2007) Maltreatment ofStrongyloides infection: case series and worldwide physicians-in-trainingsurvey. Am J Med 120:545-51.
- Loutfy MR, Wilson M, Keystone JS, Kain KC (2002) Serology and eosinophilcount in the diagnosis and management of strongyloidiasis in a nonendemicarea. Am J Trop Med Hyg 66:749-52.





