Case Report of Making Diagnosis and Successful Surgical Treatment of Double Aortic Arch in Vietnam National Children’s Hospital
Hanh LTH1, Huyen TT1, Thanh DTM2*
1 Respiratory Department of Vietnam National Hospital of Pediatrics, Vietnam.
2 General, A Department of Vietnam National Hospital of Pediatrics, Vietnam.
*Corresponding Author
Doan Thi Mai Thanh,
General, A Department of Vietnam National Hospital of Pediatrics, Vietnam.
E-mail: maithanhnhp@gmail.com
Received: May 11, 2018; Accepted: May 29, 2018; Published: May 31, 2018
Citation: Hanh LTH, Huyen TT, Thanh DTM. Case Report of Making Diagnosis and Successful Surgical Treatment of Double Aortic Arch in Vietnam National Children’s Hospital. Int J Cardiol Res. 2018;5(1):101-103. doi: http://dx.doi.org/10.19070/2470-4563-1800017
Copyright: Thanh DTM© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A 3 years old girl presented with prolonged pneumonia which was poor response to usual treatment.
History: Normal past obstetric history, recurrent pneumonia since 1 year old, allergic to shrimp; no family history of atopy; history of foreign body aspiration was not mentioned.
Investigations: Big heart shadow on chest X-ray, tracheal stenosis and neglected foreign body were found by bronchoscopy. Double aortic arch was confirmed by echocardiography, 3D-MSCT and cardiac catheterization. Operation was performing successfully.
Conclusion: Foreign bodies and cardiovascular malformations are reasons should be noticed in children with persistent pneumonia.
2.Introduction
3.Case Presentation
3.1 Examination
3.2 Chest X-ray
3.3 Labs
4.Discussion
5.Conclusion
6.References
Keywords
Double Aortic Arch; Persistent Pneumonia; Children.
Introduction
Double aortic arch a vascular ring anomaly in which both embryonic aortic arches persist and encircle the trachea and esophagus is rare, presenting in just 1 of 1000 pregnancies [1]. The presentation of vascular rings often is nonspecific, including respiratory and GI features, which complicates the diagnosis.
In this case report, we present a child who has a double aortic arch vascular ring anomaly. We emphasize the importance of recognizing persistent stridor early and treating the underlying cause can, indeed, optimize outcomes in persistent pneumonia.
Case Presentation
KT is 3 years old girl was transferred to National Children’s Hospital (NCH) because of coughing persists for nearly 1 month. She was diagnosed with Pneumonia and treated in local hospital but had not been totally in control. She coughs both day and night as bouts, sometimes vomiting after coughing, wheezing from time to time, no apnea, and intermittent fever.
Alert. Well grown for her age. No pale. Normal chest. Normal airflow, wet riles in both lungs. Normal heart rate, no murmur. Rest of exam unremarkable.
Abnormal heart shadow, cardiothoracic ratio is 60%.
Mild elevated WBC and CRP. Eosinophile is under 4%. No anemia.
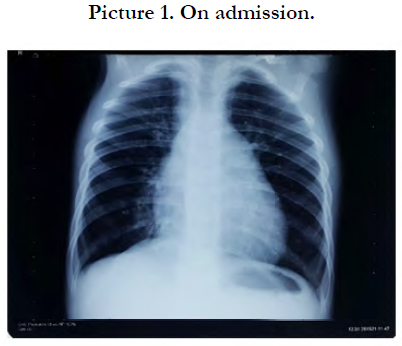

Picture 1. On admission.
Past history: full- term baby, normal delivery. Vaccinated uptodate. Normal BCG scar. She has had many time of pneumonia, bronchitis since she was 1 year old, but this episode is the longest. Mother said that KT was performed echocardiography 1 year ago in the provincial hospital and the result was normal. KT is allergic to shrimp (urticaria). No family history of atopic diseases. History of foreign body aspiration was not mentioned.
We decided to do a bronchoscopy to eliminate airway abnormalities as well as finding microorganism pathology. And we saw tracheal stenosis which is located 1cm above the carina, 1cm length, mostly on right side. We suspected that it is pressed from the outside causing half of the caliber narrowing. No tracheoesophageal fistula. Detection of a yellow foreign body in the bronchi of lower right lobe which looks like a seed 2x2 mm, purulent in the bronchial tube. We removed foreign body and performed the installation.
Then echocardiography was done two times and found rightsided aortic arch, however, they did not see the double aortic arch or sling.
The right-sided aortic arch was also recognized on MSCT; a blood vessel behind esophagus with diverticular form 11x8 mm was noted.
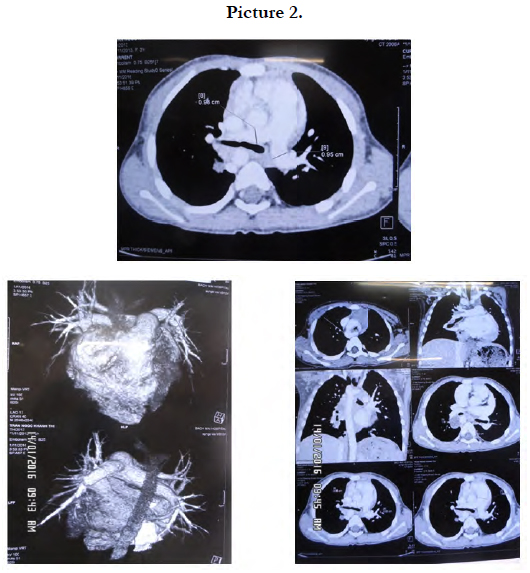
Picture 2.
Thus it can be concluded that KT had prolonged pneumonia due to neglected foreign body combine with anatomy abnormalities of the aortic arch.
After her pneumonia was treated stably, we did cardiac catheterization and saw the main aortic arch in the right side, the secondary in left side which branches left common carotid artery and left subclavian artery, Kommerell diverticulum in the thoracic aorta, no PDA.
KT had successful surgery (removed arterial ligament, left arch and diverticulum) and discharged with no cough, no wheezing. She gains weight and went to school as a normal child.
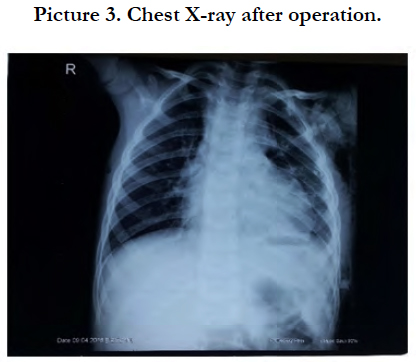

Picture 3. Chest X-ray after operation.
Discussion
There are many causes of prolonging cough such as tuberculosis, asthma (TB), GERD, especially foreign bodies in a three year-old child that often are missed out. KT has a history of food allergy, but a wheezing and allergic cough were not the outstanding symptoms, no family history of atopy, eosinophile was under 4%, so diagnostic of asthma was not persuaded.
History of recurrent pneumonia and big heart shadow on chest X-ray suggest congenital heart disease in this child (picture1). However, complicated and rare vascular abnormalities are not always determined on echocardiography.
Double aortic arches uncommon cardiology abnormality but it is one of the two most common forms of vascular ring. Airway compression increase with age so the more the child grows up, the more obvious clinical manifestation is. The severity of symptoms varies with the degree of tracheoesophageal compression. Unlike stridor caused by laryngomalacia, stridor associated with vascular ring anomaly does not worsen when the infant is placed in the supine position or when the infant cries and strains. Stridor caused by vascular ring anomalies worsens with feeding, similar to tracheomalacia and tracheoesophageal fistula [1].
If the clinical picture supports a diagnosis of vascular ring anomaly, several imaging studies may provide confirmation. Plain anterior and lateral chest radiographs and barium esophagography can confirm the presence of a vascular anomaly. Barium esophagography requires that the patient swallow a barium sulfate solution and that fluoroscopy images be taken promptly thereafter. The detection rate is lower in plain radiographs than in barium esophagography, but radiographs are useful in ruling out other respiratory symptoms [2].
Bronchoscopy can help identify the pulsatile compression of the posterior and lateral walls of the trachea associated with double aortic arch anomaly as well as allow for examination of the upper airway.
Echocardiography is used liberally in evaluating patients for vascular ring anomalies because it may be adequate for diagnosis and is less invasive than other modalities. Although the double aortic arch vascular ring anomaly usually occurs, without associated cardiovascular anomalies [3]. Echocardiography provides the added ability to rule out intracardiac anomalies [4].
MRI and CT are noninvasive imaging options that are helpful in planning for surgery. Prenatal diagnosis via ultrasonography also is available and is very accurate [5, 6].
The consequences of missing a double aortic arch diagnosis vary. In infants, tracheal compression may result in tracheomalacia and associated breathing difficulties. Older children often present with frequent lower respiratory tract infections because they have difficulty with clearing secretions from below the compressed portion of the trachea [5].
Conclusion
Standing in front of a patient with recurrent and prolonged pneumonia who has poor response to usual treatment, cardiovascular malformations are reasons should be noticed to find out and have timely intervention.
References
- Tuo G, Volpe P, Bava GL, Bondanza S, De Robertis V, et al. Prenatal diagnosis and outcome of isolated vascular rings. Am J Cardiol. 2009 Feb 1;103(3):416-9. PubMed PMID: 19166700.
- Umegaki T, Sumi C, Nishi K, Ikeda S, Shingu K. Airway management in an infant with double aortic arch. J Anesth. 2010 Feb;24(1):117-20. PubMed PMID: 20052496.
- Jeeyani HN, Prajapati VJ, Patel NH, Shah SB. Imaging features of double aortic arch shown by multidetector computed tomography angiography. Ann Pediatr Cardiol. 2010 Jul;3(2):169-70. PubMed PMID: 21234198.
- Alsenaidi K, Gurofsky R, Karamlou T, Williams WG, McCrindle BW. Management and outcomes of double aortic arch in 81 patients. Pediatrics. 2006 Nov;118(5):e1336-41. PubMed PMID: 17000782.
- Woods RK, Sharp RJ, Holcomb GW, Snyder CL, Lofland GK, et al. Vascular anomalies and tracheoesophageal compression: a single institution’s 25- year experience. Ann Thorac Surg. 2001 Aug;72(2):434-8. PubMed PMID: 11515879.
- Kellenberger CJ. Aortic arch malformations. Pediatr Radiol. 2010 Jun 1;40(6):876-84.





