Unprotected Distal LMCA Angioplasty with Simulataneous Kissing Stent (SKS) Technique in Left Dominant Coronary Circulation: A Nightmare for Interventionist
H.S. Natraj Setty*, T .R .Raghu, Jayashree Kharge, B.K. Geetha, Veeresh Patil Hebbal, Shivananda Patil, C. N. Manjunath
Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore, Karnataka, India.
*Corresponding Author
Dr. H.S.Natraj Setty MD DM,
H.no 493, 4th cross 7th main JP Nagar,
3rd phase Bangalore 69, Karnataka,
India.
Tel: 09845612322
Fax: 080-22977261
E-mail: drnatrajsetty75@gmail.com
Article Type: Case Report
Received: August 10, 2015 ; Accepted: September 24, 2015; Published: September 25, 2015
Citation: H.S.Natraj Setty, et al., (2015) Unprotected Distal LMCA Angioplasty with Simulataneous Kissing Stent (SKS) Technique in Left Dominant Coronary Circulation: A Nightmare for Interventionist. Int J Cardiol Res. 02(4), 37-40. doi: dx.doi.org/10.19070/2470-4563-150009
Copyright: H.S.Natraj Setty© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Left main coronary artery stenosis is the most challenging lesion in patients with acute coronary syndromes. Since the amount of myocardium at risk is very high, the patient is often in cardiogenic shock, and the risk of death is high and even more so in left dominant coronary system. Left main stenosis is a Class I indication for CABG -ACC/AHA guidelines and has been a relative contraindication to PCI. We report an elderly patient presenting with ACS with ECG showing ST elevation in lead a VR. Coronary angiogram revealed left dominant system with left main stenosis and ostioproximal LAD and LCX disease. Double stenting of the unprotected left main with bifurcation disease done with SKS technique with simultaneous stenting and post balloon dilatation was done with good results. Current guidelines still indicate CABG as optimal treatment for LMCA lesions. The choice of stenting technique for LMCA bifurcations should be based on bifurcation morphology.
2.Background
3.Case Report
4.Discussion
5.Conclusion
6.Human and/or Animal Rights statement
7.References
KeyWords
Unprotected Left Main Disease; Bifurcation Disease; PCI; SKS Technique.
Background
Left main coronary artery stenosis is the most challenging lesion in patients with acute coronary syndromes. Since the amount of myocardium at risk is very high, the patient is often in cardiogenic shock, and the risk of death is high and even more so in a left dominant coronary system.
Left main stenosis is a Class I indication for CABG - ACC/AHA guidelines and has been a relative contraindication to PCI. The important decision is to select an appropriate technique out of the various techniques for stenting (like T technique – classical and modified, Crush technique, Culotte technique, V stenting, SKS technique etc.).
Case Report
An elderly man aged 67 yrs, a smoker and hypertensive, presented with exertional angina since past 3 months and rest angina since morning. On admission, he was hemodynamically stable, his blood pressure was 160/80 mmHg and the heart rate 75/min. No symptoms of heart failure were observed. Electrocardiogram showed normal sinus rhythm with ST depression in leads I, aVL, V4-V6 and ST elevation in lead aVR. 2D- ECHO showed no regional wall motion abnormality and normal left ventricular function. His cardiac biomarkers: Troponin T and CKMB (creatinine kinase-MB type) were elevated. Patient was taken for coronary angiogram (CAG). CAG revealed left dominant circulation with 90% Distal LMCA stenosis (Figure 1). Ostioproximal LAD and LCX showed 50% - 60% stenosis. The non-dominant right coronary artery was without any significant lesions (Figure 2).
Since patient refused CABG, we decided to perform percutaneous coronary intervention of unprotected LMCA. A 7 French 3.5’ EBU (extra back up) guiding catheter was used. A 0.014’’ BMW guidewire was passed down the left anterior descending artery (LMCA-LAD) and (LMCA-LCX) and simultaneous predilated with 10 atm pressure (Figure 3).
Then we advanced 3.5x18mm Endeavor sprint Everolimus stent to LAD and 3x24mm Endeavor sprint Everolimus stent to LCX,
both stents were simultaneously deployed at 14 atm by simultaneous kissing stenting technique (Figure 4). The stents were then post-dilated simultaneously, with a 4.0 × 12 mm non-compliant balloon (LAD stent) and 3.5x10 mm non-compliant balloon (LCX stent), at the pressure of 18 atm. On angiography no residual stenosis noted (Figure 5). Patient was hemodynamically stable throughout the procedure and was discharged in a stable state with dual antiplatelets, statin, betablockers and ARB’s.
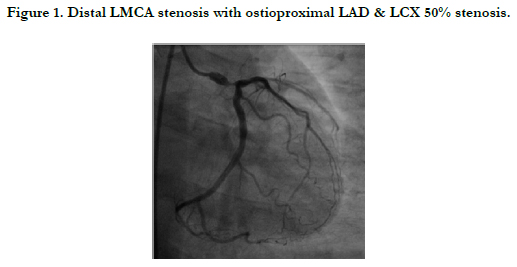
Figure 1. Distal LMCA stenosis with ostioproximal LAD & LCX 50% stenosis.
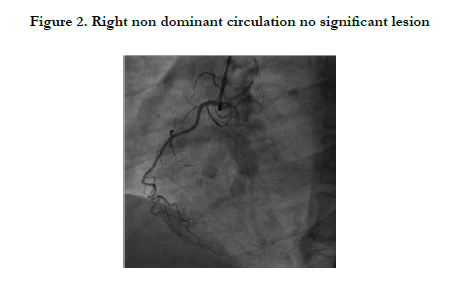
Figure 2. Right non dominant circulation no significant lesion
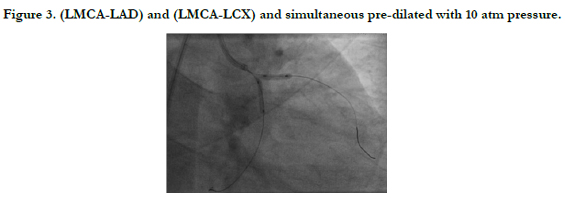
Figure 3. (LMCA-LAD) and (LMCA-LCX) and simultaneous pre-dilated with 10 atm pressure.
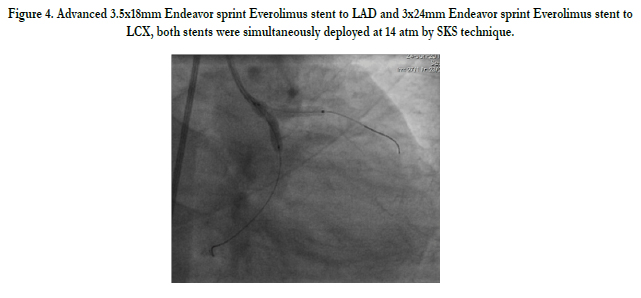
Figure 4. Advanced 3.5x18mm Endeavor sprint Everolimus stent to LAD and 3x24mm Endeavor sprint Everolimus stent to LCX, both stents were simultaneously deployed at 14 atm by SKS technique.
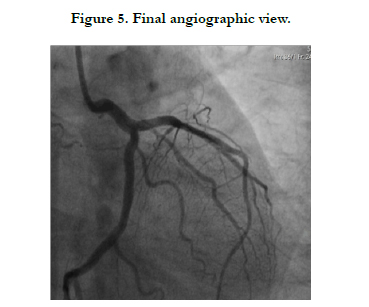
Figure 5. Final angiographic view.
Discussion
Left main coronary artery stenosis is the most challenging lesion in patients with acute coronary syndromes. Since the amount of myocardium at risk is very high, the patient is often in cardiogenic shock, and the risk of death is high and even more so in a left dominant coronary system.
Left main stenosis is a Class I indication for CABG ACC/AHA guidelines [1] and has been a relative contraindication to PCI partly because of catastrophic consequences of abrupt vessel closure and restenosis seen in the present and early stent era [2, 3]. Coronary artery bypass grafting(CABG) is currently the routine treatment for unprotected LMCA disease, but with the substantial progress in interventional techniques and equipment there is a growing body of evidence that LMCA lesions may be treated effectively and safely by interventionists [4, 5].
The evidence that was used to suggest that PCI is harmful at the time of guidelines synthesis was based on the literature published between 1997 and 2005 [6] and also from the ULTIMA (Unprotected Left Main Trunk Intervention Multicenter Assessment) registry [7].
Subsequently registries comparing DES (Drug Eluting Stent) to CABG surgery for ULMCAD appeared that provided new data regarding the comparative efficacy of DES to CABG surgery. Chieffo et al. [8] registry, Bologna et al. [9] registry, Lee et al. [5] registry and MAIN-COMPARE registry [10] showed that DES use in ULMCAD patients was associated with similar incidence of cardiac death and MI, but lower incidence of strokes, however the incidence of repeat revascularization increased. Similar results were seen with the two large randomized clinical trials: LE MANS Trial [4] and the SYNTAX Trial [11]. In SYNTAX Trial, the higher need for repeat revascularization in the DES group was significant only in patients with left main stenosis plus two or three vessel disease. It also showed that patients with low and intermediate SYNTAX score had similar MACCE rate compared with CABG group but had higher MACCE rates with higher SYNTAX score.
In the present case, as the patient refused for CABG, we decided to perform angioplasty of the unprotected left main coronary artery despite having on-site cardiac surgery.
Our decision also resulted from the fact that the patient had non ST-elevation myocardial infarction with ongoing angina, with a prominent unstable plaque in LMCA requiring urgent revascularization. The presence of a non-dominant right coronary artery, further increased the risk of the procedure. The medina classification of our patient with left main and bifurcation disease was [1, 10].
The next important decision was to select the appropriate technique out of the various techniques for stenting (like T technique – classical and modified, Crush technique, Culotte technique, V stenting, SKS technique etc.). The SKS technique seems well suited to treat our patient with LMCA bifurcation lesions for number of reasons. First the anatomy if LMCA bifurcation usually follows the pattern of one large vessel giving rise to two medium sized vessels both vessels being more than 2.5mm in size. This is suited for insertion of two stents with large bore in LMCA, where the two barrels are next to each other and smaller individual bores in each of the main branches. Second, the SKS can treat multiple disease segment in one pass. Third, the technique is simple and less time consuming. There is no requirement for rewiring through the side of the stent as in case of crush technique. Once the two main vessels have been wired, the wires can stay in the position through-out the procedure.
Conclusion
Current guidelines still indicate CABG as optimal treatment for LMCA lesions. However, the registries and randomized clinical trials have shown noninferiority of PCI in comparison with CABG in terms of MI, death and CVA events at medium term follow-up. The choice of stenting technique for LMCA bifurcations should be based on bifurcation morphology, size of the side branch, distribution of the disease and operator experience. Elective double stenting should be considered when the side branch Is large with large area of distribution and disease extending beyond the ostium. Double stenting with V-stenting and SKS may be considered when complex bifurcations involving large territories or in unstable patients whereas other techniques require recrossing the wire and hence complex, time consuming and also requires operator expertise.
Human and/or Animal Rights statement
Ethical committee clearance obtained, patient’s consent obtained.
References
- Eagle KA, Guyton RA, Davidoff R, Ewy GA, Fonger J, et al. (1999) ACC/ AHA guidelines for coronary artery bypass graft surgery: Executive summery and recommendations: A report of the ACC/AHA task force on practical guidelines (committee to revise the 1991 guidelines for coronary artery bypass graft surgery). Circulation 100: 1464-1480.
- O’keefe JH Jr, Hartzler GO, Rutherford BD, McConahay DR, Johnason WL, et al. (1989) Left main coronary angioplasty: Early and late results of 127 acute and elective procedures. Am J Cardiol 64(3): 144-147.
- Harlan JL, Meng RL (1987) Thrombosis of the left main coronary artery following percutaneous transluminal coronary angioplasty. Ann Thorac Surg 43(2): 220-223.
- Buszman PE, Kiesz SR, Bochenek A, Peszek-Przybyla E, Szkrobka I, et al. (2008) Acute and late outcomes of unprotected left main stenting in comparison with surgical revascularization. J Am Coll Cardiol 51(5): 538-545.
- Lee Ms, Kapoor N, Jamal F, Czer L, Aragon J, et al. (2006) Comparison of coronary artery bypass surgery with percutaneous coronary intervention with drug-eluting stents for unprotected left main coronary artery disease. J Am Coll Cardiol 47(4): 864-870.
- Smith SC Jr, Feldman TE, Hirshfeld JW Jr, Jacobs AK, Kern MJ, et al. (2006) ACC/AHA/SCAI 2005 guidelines update for PCI – summary article- a report of ACC/AHA task force on practice guidelines. J Am Coll Cardiol 47(1): 216-235.
- Ellis SG, Tamai H, Nobuyoshi M, Kosuga K, Colombo A, et al. (1997) Contemporary percutaneous treatment of unprotected left main coronary stenosis: initial results from a multicenter registry analysis 1994-1996. Circulation 96(11): 3867-3872.
- Chieffo A, Morici N, Maisano F, Bonizzoni E, Cosgrave J, et al. (2006) Percutaneous treatment with drug-eluting stent implantation versus bypass surgery for unprotected left main stenosis: A single center experience. Circulation 113(21): 2542-2547.
- Palmerini T, Marzocchi A, Marrozzini C, Ortolani P, Saia F, et al. (2006) Comparison between coronary angioplasty and coronary artery bypass surgery for the treatment of unprotected left main stenosis (Bologna registry). Am J Cardiol 98(1): 54-59.
- Seung KB, Park DW, Kim YH, Lee SW, Lee CW, et al. (2008) Stents versus caronary-artery bypass grafting for left main coronary artery disease. N Engl J Med 358(17): 1781-1792.
- Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, et al. (2009) For the SYNTAX Investigators. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med 360(10): 961-972.





